You might also like
- Correcting Mold Misinformation MythsDocument8 pagesCorrecting Mold Misinformation MythshazmatlinkNo ratings yet
- Indoor Mold Exposure Health Effects and ImmunotherapyDocument15 pagesIndoor Mold Exposure Health Effects and ImmunotherapyAtlas CerboNo ratings yet
- Zagadjivaci SonjaDocument4 pagesZagadjivaci SonjaАнђела КостићNo ratings yet
- The Toxicant Induction of Irritant Asthma, Rhinitis, and Related ConditionsFrom EverandThe Toxicant Induction of Irritant Asthma, Rhinitis, and Related ConditionsNo ratings yet
- Review Bioaerosol Health Effects and Exposure Assessment: Progress and ProspectsDocument14 pagesReview Bioaerosol Health Effects and Exposure Assessment: Progress and ProspectsTri MawarniNo ratings yet
- Review of Literature - Anusha BhandarkarDocument26 pagesReview of Literature - Anusha BhandarkarAnushaNo ratings yet
- Biology Advances in Applied Microbiology Fungi and The Indoor Environment (2004)Document462 pagesBiology Advances in Applied Microbiology Fungi and The Indoor Environment (2004)suanigioNo ratings yet
- Ousing AS A OF Ealth: EterminantsDocument6 pagesOusing AS A OF Ealth: EterminantsMac Vince HipolitoNo ratings yet
- Childhood Asthma Etiology and EpidemiologyDocument24 pagesChildhood Asthma Etiology and EpidemiologyEstella100% (1)
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Ispa Pada Orang Dewasa Di Desa Besuk Kecamatan Bantaran Kabupaten ProbolinggoDocument10 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Ispa Pada Orang Dewasa Di Desa Besuk Kecamatan Bantaran Kabupaten ProbolinggoirfanNo ratings yet
- Fungi and Health - Baxi2016 - Volume 4, Issue 3, May-June 2016, Pages 396-404Document9 pagesFungi and Health - Baxi2016 - Volume 4, Issue 3, May-June 2016, Pages 396-404Choi KhoironNo ratings yet
- TerminologyDocument7 pagesTerminologyshantanulcNo ratings yet
- Environmental and Occupational AllergiesDocument11 pagesEnvironmental and Occupational AllergiesRatna WindyaningrumNo ratings yet
- 1991 - Darke, Guinan, Gold - Allergy and AsthmaDocument13 pages1991 - Darke, Guinan, Gold - Allergy and AsthmaPJ Chalet BookNo ratings yet
- Mycosis As Co-Infection Among Tuberculosis Infected Patients in Some Countries: A Systematic ReviewDocument8 pagesMycosis As Co-Infection Among Tuberculosis Infected Patients in Some Countries: A Systematic Reviewsyifa18No ratings yet
- Theories of DiseaseDocument6 pagesTheories of DiseaseTobi OladipupoNo ratings yet
- admin,+114+Layout+JR+7 (1) +DR +catur+ (P 152157)Document6 pagesadmin,+114+Layout+JR+7 (1) +DR +catur+ (P 152157)Tito TrisaputraNo ratings yet
- A Review by The Forum of International Respiratory SocietiesEnvironmental Committee, Part 1Document8 pagesA Review by The Forum of International Respiratory SocietiesEnvironmental Committee, Part 1lidysNo ratings yet
- Pediatric Allergy Immunology - 2023 - BiagioniDocument11 pagesPediatric Allergy Immunology - 2023 - BiagioniMiguel Angel DionicioNo ratings yet
- Learning Materials 1Document34 pagesLearning Materials 1mirabel IvanaliNo ratings yet
- EVOLUTIONARY ASPECTS OF DISEASE AVOIDANCE The Role of Disease in the Development of Complex SocietyFrom EverandEVOLUTIONARY ASPECTS OF DISEASE AVOIDANCE The Role of Disease in the Development of Complex SocietyNo ratings yet
- Bacteria Infection of The Respiratory TractDocument8 pagesBacteria Infection of The Respiratory TractChidi EmmanuelNo ratings yet
- CROOK, BURTON - Indoor Moulds, Sick Building Syndrome and Building Related IllnessDocument8 pagesCROOK, BURTON - Indoor Moulds, Sick Building Syndrome and Building Related Illnessvrtzio100% (1)
- Asthma: Whom Does It Affect?Document11 pagesAsthma: Whom Does It Affect?Ken KennyNo ratings yet
- Sick Building Syndrome: Janis Jansz, Curtin University, Perth, WA, AustraliaDocument4 pagesSick Building Syndrome: Janis Jansz, Curtin University, Perth, WA, AustraliaWanda ZakariaNo ratings yet
- Term Paper Pop202 Id 2021-2-80-027Document14 pagesTerm Paper Pop202 Id 2021-2-80-027MH ULLASHNo ratings yet
- Emerging and Reemerging Infectious DiseasesDocument13 pagesEmerging and Reemerging Infectious DiseasesSayu100% (1)
- Etm 12 04 2383Document4 pagesEtm 12 04 2383mukhlis akmalNo ratings yet
- Environmental Research: Review ArticleDocument7 pagesEnvironmental Research: Review ArticleMaria Jose Altamirano CastroNo ratings yet
- The Common Cold Current Therapy and Natural HistoDocument6 pagesThe Common Cold Current Therapy and Natural HistoNur Wahdania PutriNo ratings yet
- Chemical and Biological Health Hazards and Control: Inhalable DustsDocument33 pagesChemical and Biological Health Hazards and Control: Inhalable DustsDeva DNo ratings yet
- Review of Literature on Asthma Definition, Types, Diagnosis and TreatmentsDocument23 pagesReview of Literature on Asthma Definition, Types, Diagnosis and TreatmentsPurple Ivy GuarraNo ratings yet
- Epidimiology Chapter 4Document24 pagesEpidimiology Chapter 4Sarika YadavNo ratings yet
- Injection Anthrax-A New Outbreak in Heroin Users: Original ArticleDocument6 pagesInjection Anthrax-A New Outbreak in Heroin Users: Original ArticleWikan PutridewiNo ratings yet
- West SARS Epidemic 2003Document29 pagesWest SARS Epidemic 2003RafiamNo ratings yet
- ACTIVITY-3 finalDocument3 pagesACTIVITY-3 finalAira Clair AlcanoNo ratings yet
- Article in Press: Allergens, Air Pollutants, and Childhood Allergic DiseasesDocument6 pagesArticle in Press: Allergens, Air Pollutants, and Childhood Allergic DiseasesYLLWNo ratings yet
- COVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsFrom EverandCOVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsNo ratings yet
- Hubungan Faktor Risiko Umur, Jenis Kelamin Dan Kepadatan Hunian Dengan Kejadian Penyakit TB Paru Di Desa Wori Kecamatan WoriDocument9 pagesHubungan Faktor Risiko Umur, Jenis Kelamin Dan Kepadatan Hunian Dengan Kejadian Penyakit TB Paru Di Desa Wori Kecamatan Woriclarico cullenNo ratings yet
- The Role of Global Air Pollution in Aging and Disease: Reading Smoke SignalsFrom EverandThe Role of Global Air Pollution in Aging and Disease: Reading Smoke SignalsNo ratings yet
- Siemens 2017Document17 pagesSiemens 2017Ario HalkiNo ratings yet
- Asthma 2Document8 pagesAsthma 2Evangelist Stephen NziokaNo ratings yet
- Biology 1101 Final PaperDocument8 pagesBiology 1101 Final Paperelias.gathekia17No ratings yet
- Nihms 1055752Document13 pagesNihms 1055752ani putkaradzeNo ratings yet
- Historical background of coronavirusesDocument7 pagesHistorical background of coronavirusesClarice Faye CantilNo ratings yet
- A Comparative Study of Acquiring Pneumonitis Among Smokers and Passive Smokers With AscariasisDocument32 pagesA Comparative Study of Acquiring Pneumonitis Among Smokers and Passive Smokers With AscariasisJim AsenciNo ratings yet
- Bubonic Plague Research PaperDocument10 pagesBubonic Plague Research PaperKristie ChengNo ratings yet
- Is Mold Toxicity Really A ProbDocument6 pagesIs Mold Toxicity Really A Probmtb75qbw4rNo ratings yet
- Global Indoor Health Network: Common Toxins in Our Homes, Schools and WorkplacesDocument78 pagesGlobal Indoor Health Network: Common Toxins in Our Homes, Schools and Workplacesapi-202939585No ratings yet
- Pneumococcal Pneumonia: Causes, Risks, PreventionDocument7 pagesPneumococcal Pneumonia: Causes, Risks, PreventionShalini DoraisingamNo ratings yet
- Epidemiology As A PopulationDocument4 pagesEpidemiology As A PopulationvalentinaNo ratings yet
- Mold Health Issues-2017Document11 pagesMold Health Issues-2017pseto100% (1)
- Asthma: Signs and SymptomsDocument7 pagesAsthma: Signs and SymptomsPavitrra SubbramaniyamNo ratings yet
- Dapus No 36 BaruDocument16 pagesDapus No 36 BarupnkNo ratings yet
- Infeccion Focal Newman1996Document8 pagesInfeccion Focal Newman1996Lucía LGNo ratings yet
- Changes to Customs Rules Prevent Viruses from Foreign FaunaDocument16 pagesChanges to Customs Rules Prevent Viruses from Foreign FaunaJuan Carlos UriarteNo ratings yet
- Bates 1995 The Effects of Air Pollution On ChildrenDocument5 pagesBates 1995 The Effects of Air Pollution On ChildrenFelia AlyciaNo ratings yet
- Spoilage and Heating of Stored Agri Products PDFDocument98 pagesSpoilage and Heating of Stored Agri Products PDFGospodin RajkovićNo ratings yet
- Water Activity and CoffeeDocument2 pagesWater Activity and CoffeeGambia TostadoresNo ratings yet
- College Chemistry Science Experiment PaperDocument15 pagesCollege Chemistry Science Experiment Paperapi-637236743No ratings yet
- Pharmaceutical Microbiology: PHAR443BDocument98 pagesPharmaceutical Microbiology: PHAR443BAlfrida Putri PuspitaNo ratings yet
- Oil SeedDocument12 pagesOil SeedMohamed Mohamed AbdulhayNo ratings yet
- Cold Room Cleaning and Maintenance ProcedureDocument2 pagesCold Room Cleaning and Maintenance ProceduremasssssoudNo ratings yet
- Introduction To Food and Water MicrobiologyDocument38 pagesIntroduction To Food and Water MicrobiologyAMNA ADILNo ratings yet
- Major scientific and technological developments that shaped daily lifeDocument4 pagesMajor scientific and technological developments that shaped daily lifeMichelle Delgado67% (3)
- The D7 Guide to Safer, More Efficient RemediationDocument19 pagesThe D7 Guide to Safer, More Efficient RemediationJainil Panchal100% (1)
- Science 7: EssentialDocument11 pagesScience 7: EssentialHeba FaroukNo ratings yet
- Dried Figs: Packing, Transporting and Risk FactorsDocument23 pagesDried Figs: Packing, Transporting and Risk Factorshttp://www.scribd.comNo ratings yet
- Microbiology of Milk and It's ContaminantsDocument26 pagesMicrobiology of Milk and It's ContaminantsKavin ANo ratings yet
- BIOLOGY INVESTIGATORY PROJECT- mold growthDocument11 pagesBIOLOGY INVESTIGATORY PROJECT- mold growthGowri SureshNo ratings yet
- Fdim142 PDFDocument181 pagesFdim142 PDFBoooooooseNo ratings yet
- Biological To Physical Hazards Complete ReviewerDocument42 pagesBiological To Physical Hazards Complete ReviewerJman MontoyaNo ratings yet
- Mold ToxinsDocument7 pagesMold ToxinsMikiatlantul100% (1)
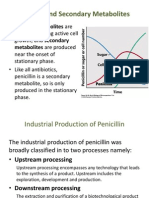
- Primary vs Secondary Metabolites in Penicillin ProductionDocument6 pagesPrimary vs Secondary Metabolites in Penicillin Productionzuzuzazazizi0% (1)
- Organisation of An Ecosystem Part I QuestionsDocument77 pagesOrganisation of An Ecosystem Part I QuestionsLenka CarterNo ratings yet
- Guidelines on Preventing Mould Growth in Buildings JKR MalaysiaDocument44 pagesGuidelines on Preventing Mould Growth in Buildings JKR MalaysiaAlex Chin60% (5)
- Shelf Life Date Marking GuidanceDocument33 pagesShelf Life Date Marking GuidancewiljowNo ratings yet
- Fermented Plant Juice Leguminous CropsDocument13 pagesFermented Plant Juice Leguminous CropsAlgeragen Tagoon VelascoNo ratings yet
- Contamination and Spoilage of Meat and Meat ProductsDocument12 pagesContamination and Spoilage of Meat and Meat ProductsAronjamesNo ratings yet
- 00A 097 Comprehensive Microbial Identification With OdinDocument5 pages00A 097 Comprehensive Microbial Identification With OdingombasgNo ratings yet
- The Magic Mushroom Growers GuideDocument30 pagesThe Magic Mushroom Growers GuidebuboynanayNo ratings yet
- Mold ExperimentDocument13 pagesMold ExperimentDianecute M. Bacalla67% (6)
- Storage and Quality Testing of Bakery ProductsDocument7 pagesStorage and Quality Testing of Bakery ProductsPamilaNo ratings yet
- Food Spoilage Microorganisms and Their PreventionDocument10 pagesFood Spoilage Microorganisms and Their PreventionShahriar Shamim100% (2)
- RTP 2500 FR ADocument2 pagesRTP 2500 FR ASoopNo ratings yet
- Okinawa Black Galingale CultivationDocument11 pagesOkinawa Black Galingale CultivationAgung Satriya WibowoNo ratings yet