You might also like
- Parent Training in Autism Spectrum Disorder - What's in A Name - PDFDocument20 pagesParent Training in Autism Spectrum Disorder - What's in A Name - PDFFarbodNo ratings yet
- AP Psych Anatomy The Brain - Coloring Worksheet - Visual MapDocument2 pagesAP Psych Anatomy The Brain - Coloring Worksheet - Visual MapTiffany GallinaNo ratings yet
- 2022 ITECritiqueDocument80 pages2022 ITECritiqueJon LetkoNo ratings yet
- Pattern Classification SlideDocument45 pagesPattern Classification SlideTiến QuảngNo ratings yet
- Educ 311: Facilitating Learner - Centered Teaching: Divine Grace V. Galorio Beed-IiiDocument3 pagesEduc 311: Facilitating Learner - Centered Teaching: Divine Grace V. Galorio Beed-IiiDivine Grace Villanueva Galorio100% (2)
- Consumer Behavior: Consumer Perception and PositioningDocument22 pagesConsumer Behavior: Consumer Perception and PositioningMarium RazaNo ratings yet
- Duration of Dual Antiplatelet Therapy in Acute Coronary SyndromeDocument8 pagesDuration of Dual Antiplatelet Therapy in Acute Coronary SyndromeCaro GasparNo ratings yet
- Methods of Coronary Revascularization - Things May Not Be As They SeemDocument3 pagesMethods of Coronary Revascularization - Things May Not Be As They SeemWilliam MakdinataNo ratings yet
- Colchicine in Coronary Artery Disease (NEJM, 2020) PDFDocument10 pagesColchicine in Coronary Artery Disease (NEJM, 2020) PDFthe_leoNo ratings yet
- 1 s2.0 S0914508717302745 Main PDFDocument5 pages1 s2.0 S0914508717302745 Main PDFAdriani HartantoNo ratings yet
- Troponin Assays: More Questions Than Answers?: Doi: 10.1111/j.1742-6723.2009.01225.xDocument2 pagesTroponin Assays: More Questions Than Answers?: Doi: 10.1111/j.1742-6723.2009.01225.xprashsubbuNo ratings yet
- Hauser Et Al Rituximab in Relapsing-Remitting Multiple SclerosisDocument3 pagesHauser Et Al Rituximab in Relapsing-Remitting Multiple SclerosisHenrique OliveiraNo ratings yet
- Burger Et Al 2023 C Reactive Protein and Risk of Incident Heart Failure in Patients With Cardiovascular DiseaseDocument13 pagesBurger Et Al 2023 C Reactive Protein and Risk of Incident Heart Failure in Patients With Cardiovascular DiseaseKardiologi ManadoNo ratings yet
- 6 Antithrombotic Therapy in Patients With Infective EndocarditisDocument12 pages6 Antithrombotic Therapy in Patients With Infective Endocarditisabdeali hazariNo ratings yet
- 2002, Feb - Persistence of The Prothrombotic State After Acute Coronary Syndromes Implications For TreatmentDocument12 pages2002, Feb - Persistence of The Prothrombotic State After Acute Coronary Syndromes Implications For TreatmentErnestoNo ratings yet
- Covid Asociado A CoagulopatiaDocument2 pagesCovid Asociado A CoagulopatiaNahui IcatlNo ratings yet
- New Pathways in The Treatment For Menopausal Hot Flushes: CommentDocument3 pagesNew Pathways in The Treatment For Menopausal Hot Flushes: CommentAlifia DamayantiNo ratings yet
- Thrasivoulos: Cardiomyopathy in Children: Importance of Aetiology in PrognosisDocument2 pagesThrasivoulos: Cardiomyopathy in Children: Importance of Aetiology in PrognosisDede MarizalNo ratings yet
- Nejmoa2021372 PDFDocument10 pagesNejmoa2021372 PDFNiki MawraNo ratings yet
- Kolkisin PathwayDocument8 pagesKolkisin PathwayAndreas Erick HaurissaNo ratings yet
- Ehab 268Document2 pagesEhab 268yori yarson tonNo ratings yet
- Estudio JúpiterDocument6 pagesEstudio JúpiterSANCHOSKYNo ratings yet
- A Case Series of Intracardiac Thrombosis Revealing Behcets Disease in Moroccan PatientsDocument4 pagesA Case Series of Intracardiac Thrombosis Revealing Behcets Disease in Moroccan PatientsIJAR JOURNALNo ratings yet
- Use of Neutrophil Count in Early Diagnosis and Risk Stratification of AMIDocument9 pagesUse of Neutrophil Count in Early Diagnosis and Risk Stratification of AMIratihNo ratings yet
- Analisis de EC Grupo XDocument10 pagesAnalisis de EC Grupo XMarcelo MaldonadoNo ratings yet
- Ejm 04900 Case - Report CetinDocument3 pagesEjm 04900 Case - Report CetinShwan OmarNo ratings yet
- Avances en Sepsis Art Ing 2022Document10 pagesAvances en Sepsis Art Ing 2022roman rodriguezNo ratings yet
- Vijayalakshmi 2008Document7 pagesVijayalakshmi 2008Rakesh DashNo ratings yet
- Ketamine and Intracranial Pressure: No Contraindication Except HydrocephalusDocument3 pagesKetamine and Intracranial Pressure: No Contraindication Except Hydrocephaluslidwina143No ratings yet
- Secondary Antibiotic Prophylaxis For Latent Rheumatic Heart DiseaseDocument11 pagesSecondary Antibiotic Prophylaxis For Latent Rheumatic Heart DiseasejvsenenNo ratings yet
- Colchicina Enfermedad Coronaria. NEJM 2022Document10 pagesColchicina Enfermedad Coronaria. NEJM 2022Carlos Alberto Cardenas degolladoNo ratings yet
- Adjuvant Steroid Therapy in Community-Acquired Pneumonia: What 'S New in Infectious DiseasesDocument3 pagesAdjuvant Steroid Therapy in Community-Acquired Pneumonia: What 'S New in Infectious DiseasesDianNo ratings yet
- Statin Intolerance, Bempedoic Acid, and Cardiovascular OutcomesDocument4 pagesStatin Intolerance, Bempedoic Acid, and Cardiovascular OutcomesAnderson Joel GomezNo ratings yet
- Cetin 2016Document10 pagesCetin 2016Della Puspita SariNo ratings yet
- 1 Out of 7 WHODocument2 pages1 Out of 7 WHOgnaneshwar nNo ratings yet
- RF RHDDocument3 pagesRF RHDAl- Mondjid LeeNo ratings yet
- Kidney News Article p20 7Document2 pagesKidney News Article p20 7ilgarciaNo ratings yet
- Cei0121 0270Document5 pagesCei0121 0270Nur WahyuniNo ratings yet
- Myocarditis: Leslie T. Cooper Jr. and Kirk U. KnowltonDocument21 pagesMyocarditis: Leslie T. Cooper Jr. and Kirk U. KnowltonAnonymous cdLyeXKBNo ratings yet
- On-Treatment Function Testing of Platelets and Long-Term Outcome of Patients With Peripheral Arterial Disease Undergoing Transluminal AngioplastyDocument8 pagesOn-Treatment Function Testing of Platelets and Long-Term Outcome of Patients With Peripheral Arterial Disease Undergoing Transluminal AngioplastyGono GenieNo ratings yet
- Cocot TrialDocument9 pagesCocot TrialAngelEduardoVillarrealGiraldoNo ratings yet
- Efectos adversos relacionados con el uso de corticosteroides en la sepsis, el síndrome de dificultad respiratoria aguda y la neumonía adquirida en la comunidad: una revisión sistemática y un metanálisisDocument12 pagesEfectos adversos relacionados con el uso de corticosteroides en la sepsis, el síndrome de dificultad respiratoria aguda y la neumonía adquirida en la comunidad: una revisión sistemática y un metanálisisRousNo ratings yet
- Comparative Clinical Characteristics of Rheumatic Heart Disease Patients Undergoing Surgical Valve ReplacementDocument13 pagesComparative Clinical Characteristics of Rheumatic Heart Disease Patients Undergoing Surgical Valve ReplacementElvira AnitaNo ratings yet
- Lodoco PilotDocument8 pagesLodoco PilotAndreas Erick HaurissaNo ratings yet
- Acute Pericarditis: Clinical PracticeDocument8 pagesAcute Pericarditis: Clinical PracticeGaby Alejandra Ordonez AndradeNo ratings yet
- Cafaro 2023 Cardiovascular Risk in Systemic AutDocument2 pagesCafaro 2023 Cardiovascular Risk in Systemic AutSilvia PeresNo ratings yet
- Old and New Therapeutic Strategies in Systemic SclerosisDocument6 pagesOld and New Therapeutic Strategies in Systemic SclerosisJosé Javier Morales NúñezNo ratings yet
- Accidente Cerebrovascular Criptogénico Yforamen Oval Permea 2018Document9 pagesAccidente Cerebrovascular Criptogénico Yforamen Oval Permea 2018federico saldariniNo ratings yet
- Cryptogenic Stroke and Patent Foramen Ovale: Review Topic of The WeekDocument8 pagesCryptogenic Stroke and Patent Foramen Ovale: Review Topic of The WeekferrevNo ratings yet
- Actualización-Endocarditis-bacteriana AmJMed 2020Document6 pagesActualización-Endocarditis-bacteriana AmJMed 2020msq.cv5919No ratings yet
- Httpsinnovareacademics Injournalsindex Phpijppsarticledownload2221213586Document3 pagesHttpsinnovareacademics Injournalsindex Phpijppsarticledownload2221213586Gusti Ayu Sattwika PramitaNo ratings yet
- 2022 Cardiac SarcoidosisDocument7 pages2022 Cardiac SarcoidosisAnaNo ratings yet
- Laporan Kasus-Acute Embolic Stroke As The Sole Presentation of Infective Endocarditis in Mitral Valve ProlapseDocument2 pagesLaporan Kasus-Acute Embolic Stroke As The Sole Presentation of Infective Endocarditis in Mitral Valve ProlapseSari Novianty SilitongaNo ratings yet
- Procal Vs MasccDocument7 pagesProcal Vs MasccRoshan MathewNo ratings yet
- CURE TrialDocument9 pagesCURE TrialCristina PazmiñoNo ratings yet
- Clinical Use of High-Sensitivity Cardiac Troponin in Patients With Suspected Myocardial InfarctionDocument17 pagesClinical Use of High-Sensitivity Cardiac Troponin in Patients With Suspected Myocardial InfarctionQuốc ViệtNo ratings yet
- Nej Mo A 1912388Document9 pagesNej Mo A 1912388dralourdesreyespediatraNo ratings yet
- Pneumonia 4Document10 pagesPneumonia 4furqan92No ratings yet
- Stemcell CardiovascularDocument29 pagesStemcell CardiovascularAdi WijayantoNo ratings yet
- 2041.full AritmiaDocument17 pages2041.full AritmiaDeltaphierhoNo ratings yet
- Clinical Research: Heart Failure/cardiomyopathyDocument8 pagesClinical Research: Heart Failure/cardiomyopathyNoel Saúl Argüello SánchezNo ratings yet
- Medical Progress: T M H CDocument11 pagesMedical Progress: T M H CpvsvrNo ratings yet
- Cardiogenic Shock in Children 2024Document14 pagesCardiogenic Shock in Children 2024Pediatrician Suhail NaikNo ratings yet
- Heart Disease and Cancer: CirculationDocument4 pagesHeart Disease and Cancer: CirculationDewi AyuNo ratings yet
- 2017 ESC/EACTS Guidelines For The Management of Valvular Heart DiseaseDocument54 pages2017 ESC/EACTS Guidelines For The Management of Valvular Heart Diseaseeppy syafriNo ratings yet
- Role of DentistDocument5 pagesRole of Dentisteppy syafriNo ratings yet
- Pi Is 1875957213001903Document5 pagesPi Is 1875957213001903eppy syafriNo ratings yet
- Large Oral Ulcer of Tongue Related To Dental Trauma: Scientific Articles Case ReportDocument4 pagesLarge Oral Ulcer of Tongue Related To Dental Trauma: Scientific Articles Case Reporteppy syafriNo ratings yet
- Lower Back PainDocument3 pagesLower Back Paineppy syafriNo ratings yet
- Persistent Vegetative StateDocument14 pagesPersistent Vegetative StateMuhammad Abdul RahmanNo ratings yet
- NIMHANS MPHIL, PHD APPLICATION NOTIFICATION - PeppGuideDocument6 pagesNIMHANS MPHIL, PHD APPLICATION NOTIFICATION - PeppGuideswathy sudheerNo ratings yet
- Ekene's Persuasive EssayDocument2 pagesEkene's Persuasive Essayballerchick49311716No ratings yet
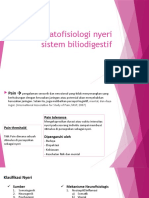
- Patofisiologi Nyeri Sistem BiliodigestifDocument22 pagesPatofisiologi Nyeri Sistem BiliodigestifNathaniaNo ratings yet
- Johannes OdendahlDocument17 pagesJohannes OdendahlMARIA ANGELICA ACOSTA MEZANo ratings yet
- Artificial Neural Network: Vardhaman College of EngineeringDocument35 pagesArtificial Neural Network: Vardhaman College of EngineeringravvalavamsiNo ratings yet
- Awr2 Trabajo-FinalDocument33 pagesAwr2 Trabajo-FinalCamila Ramos farajaNo ratings yet
- Learning Agility in Military ContextDocument29 pagesLearning Agility in Military ContextDinda CattleyaNo ratings yet
- Brain Fingerprinting: Geethika Muppa 06771A0528 4-2, CSE February 26, 2010Document21 pagesBrain Fingerprinting: Geethika Muppa 06771A0528 4-2, CSE February 26, 2010gpurple89No ratings yet
- MBTIDocument13 pagesMBTIShaina Mae CaminocNo ratings yet
- Mntessori ReportDocument6 pagesMntessori ReportSantiago RiaNo ratings yet
- 3 Designing Learning ExperiencesDocument61 pages3 Designing Learning ExperiencesMarness BautistaNo ratings yet
- Module 17 Socio Emotional Development of PreschoolersDocument4 pagesModule 17 Socio Emotional Development of PreschoolersJhermaine Audrey Gomez0% (2)
- Nature vs. NurtureDocument1 pageNature vs. NurtureMaria Olivia MercadoNo ratings yet
- Facial Action Coding System PDFDocument2 pagesFacial Action Coding System PDFAlan0% (1)
- 14 Reasons Teachers Should Keep A Reflective JournalDocument6 pages14 Reasons Teachers Should Keep A Reflective JournalSheeza JavedNo ratings yet
- TEXT BOOK - Book - Stangor.complete - OptimizedDocument479 pagesTEXT BOOK - Book - Stangor.complete - OptimizedDaniel GetahunNo ratings yet
- Stress Management Lesson PlanDocument1 pageStress Management Lesson Planapi-531037084No ratings yet
- Austin, E. J. (2004) - An Investigation of The Relationship Between Trait Emotional Intelligence and Emotional TaskDocument10 pagesAustin, E. J. (2004) - An Investigation of The Relationship Between Trait Emotional Intelligence and Emotional TaskMarceloFrancoNo ratings yet
- Craig and Banker 1994Document44 pagesCraig and Banker 1994Kanwal RashidNo ratings yet
- Mapulang Lupa National High SchoolDocument21 pagesMapulang Lupa National High SchoolMaribeth Lagang TaniNo ratings yet
- Vimp 1Document21 pagesVimp 1shubham RahateNo ratings yet
- Ch3 TB PinelDocument27 pagesCh3 TB Pinelpixelpaisley12No ratings yet
- Fluency Overview: Fluency Is The Ability To Read Text With Accuracy, SpeedDocument12 pagesFluency Overview: Fluency Is The Ability To Read Text With Accuracy, SpeedMartinArciniegaNo ratings yet
- Methods of Research (Lecture)Document20 pagesMethods of Research (Lecture)LJ TagataNo ratings yet