You might also like
- Massage Waiver and Consent FormDocument1 pageMassage Waiver and Consent FormReinalin Hernandez ErasgaNo ratings yet
- Massage Client Intake Form PDFDocument2 pagesMassage Client Intake Form PDFSheila LaingNo ratings yet
- 50 Ideas For Massage and Spa Promotion by Gael WoodDocument56 pages50 Ideas For Massage and Spa Promotion by Gael Woodnahv_08100% (2)
- Business Plan Massage TherapyDocument17 pagesBusiness Plan Massage Therapygintembalu100% (2)
- Massage Intake Form With DiagramDocument2 pagesMassage Intake Form With DiagramMr.NievesNo ratings yet
- Massage Business PlanDocument8 pagesMassage Business PlannavdeepNo ratings yet
- Relax and Rejuvenate with Massage TypesDocument21 pagesRelax and Rejuvenate with Massage TypesArt Robin NagpacanNo ratings yet
- Medical Massage ManualDocument3 pagesMedical Massage ManualPeter Sosa100% (1)
- Massage Client Waiver Form 1 2Document1 pageMassage Client Waiver Form 1 2api-516845106No ratings yet
- Learner Guide - SIBBBOS402A: Provide Body TreatmentsDocument80 pagesLearner Guide - SIBBBOS402A: Provide Body TreatmentsAtif MahmoodNo ratings yet
- Massage Career Guide 071Document24 pagesMassage Career Guide 071Jaythza M SanchezNo ratings yet
- Client Intake Form: Date Patient Last: First Initial Address City Zip Date of Birth Phone CellDocument6 pagesClient Intake Form: Date Patient Last: First Initial Address City Zip Date of Birth Phone Celljayson_tamayo2No ratings yet
- ITEC Level 4 Certificate in Sports Massage Therapy Purpose V1Document2 pagesITEC Level 4 Certificate in Sports Massage Therapy Purpose V1bbjoyweNo ratings yet
- Massage Therapy Business Plan ExampleDocument22 pagesMassage Therapy Business Plan ExampleSergei Biriukov100% (1)
- Sinus Massage By: Sushumna Mahesh What Is Sinus Pain?Document5 pagesSinus Massage By: Sushumna Mahesh What Is Sinus Pain?Julenda NikijuluwNo ratings yet
- Design of A Tuned Intake Manifold - H. W. Engelman (ASME Paper 73-WA/DGP-2)Document9 pagesDesign of A Tuned Intake Manifold - H. W. Engelman (ASME Paper 73-WA/DGP-2)david_luzNo ratings yet
- Client Intake Form - Therapeutic Massage: Personal InformationDocument4 pagesClient Intake Form - Therapeutic Massage: Personal InformationANT lib100% (1)
- Self Massage Therapy PDFDocument26 pagesSelf Massage Therapy PDFMatthewNo ratings yet
- Massage Therapy EffectsDocument12 pagesMassage Therapy EffectsEkalevi FahlepieNo ratings yet
- Client Intake FormDocument2 pagesClient Intake FormPeter Sosa100% (1)
- Sports massage consent formDocument1 pageSports massage consent formAndriusjoNo ratings yet
- New Client Intake FormDocument1 pageNew Client Intake FormTori BaileyNo ratings yet
- Structured Touch MassageDocument5 pagesStructured Touch Massagegfrankel72No ratings yet
- Caring Home Care Skills AssessmentDocument3 pagesCaring Home Care Skills AssessmentPraj100% (1)
- Massage Therapy - Workplace Massage - Chair Massage - Stress Management - Stress - Relaxation - Massage - T PDFDocument1 pageMassage Therapy - Workplace Massage - Chair Massage - Stress Management - Stress - Relaxation - Massage - T PDFnaveenNo ratings yet
- Massage TherapistsDocument15 pagesMassage Therapists4foryouukNo ratings yet
- Rate AnalysisDocument46 pagesRate AnalysisbulganinganguliNo ratings yet
- Massage Client Info SheetDocument3 pagesMassage Client Info SheetNicci AllenNo ratings yet
- Rehabilitation Team RolesDocument4 pagesRehabilitation Team RolesFrance PenalbaNo ratings yet
- Massage Intake and Agreement Form CoreDocument2 pagesMassage Intake and Agreement Form CoreCraig JohnsonNo ratings yet
- Client InformationDocument2 pagesClient InformationJonathanAllenLMTNo ratings yet
- F825 - Hotcakes Baby Cardigan FinalDocument2 pagesF825 - Hotcakes Baby Cardigan Finaladina100% (1)
- Intake FormDocument1 pageIntake Formapi-358259684No ratings yet
- Client Intake Form - Therapeutic MassageDocument2 pagesClient Intake Form - Therapeutic MassagePeter SosaNo ratings yet
- Indian Head MassageDocument49 pagesIndian Head MassagekoekemoerNo ratings yet
- Consent For Laser Hair RemovalDocument2 pagesConsent For Laser Hair RemovalCassi CrumNo ratings yet
- Marcias Esthetics Client Intake FormDocument4 pagesMarcias Esthetics Client Intake Formapi-194244218No ratings yet
- Client Info FormDocument2 pagesClient Info FormkamalsalmanNo ratings yet
- Pocedure ConsentDocument2 pagesPocedure ConsentJack TedescoNo ratings yet
- Swedish Massage InfoDocument5 pagesSwedish Massage InfoJoy CelestialNo ratings yet
- Basic MassageDocument3 pagesBasic MassageAlex Olivar100% (1)
- Client Consultation Form - Pedicure AppoinmentDocument3 pagesClient Consultation Form - Pedicure AppoinmentMicheal McDowellNo ratings yet
- MASSAGE EVIDENCE REVIEWDocument7 pagesMASSAGE EVIDENCE REVIEWRashoode Al-mezieneNo ratings yet
- Adding True Bypass To A Vintage Big MuffDocument8 pagesAdding True Bypass To A Vintage Big MuffOliver SuttonNo ratings yet
- BROCHURE - Massage Therapy Final BrochureDocument2 pagesBROCHURE - Massage Therapy Final Brochurerlczech0348No ratings yet
- Business Plan SampleDocument8 pagesBusiness Plan SamplekenyamontgomeryNo ratings yet
- Plasma ChemistryDocument6 pagesPlasma ChemistryArief RomadhonNo ratings yet
- Business & Insurance Info: PresentsDocument17 pagesBusiness & Insurance Info: PresentsАлексNo ratings yet
- Wellness Massage NC II CGDocument15 pagesWellness Massage NC II CGsanchezromanNo ratings yet
- TLE Daily Lesson LogsDocument129 pagesTLE Daily Lesson LogsJellianne Cabualan91% (46)
- Complementary TherapiesDocument7 pagesComplementary TherapiesNilamdeen Mohamed ZamilNo ratings yet
- Learner-Centered PhilosophyDocument3 pagesLearner-Centered PhilosophyEverly Oballo100% (1)
- OrlDocument186 pagesOrlMuli MaroshiNo ratings yet
- Wellness Massage CG PDFDocument11 pagesWellness Massage CG PDFRahnelyn B BonillaNo ratings yet
- The Role of Massage in Sports Performance and Rehabilitation - CurDocument17 pagesThe Role of Massage in Sports Performance and Rehabilitation - CurTamas KalmarNo ratings yet
- Beauty Nail Care CGDocument17 pagesBeauty Nail Care CGCris MacSol100% (2)
- RF 08 Transfer Related Issue - LISDocument8 pagesRF 08 Transfer Related Issue - LISMark Anthony TangarNo ratings yet
- MassageTherapy IntakeFormDocument2 pagesMassageTherapy IntakeFormslbecker01No ratings yet
- Deep Tissue MassageDocument5 pagesDeep Tissue MassageNanokoSanchezOrtizNo ratings yet
- S. Cole HW499 Unit 5 Power Point Massage TherapyDocument9 pagesS. Cole HW499 Unit 5 Power Point Massage TherapySifon ColeNo ratings yet
- G8 Develop and Maintain Effectiveness at WorkDocument4 pagesG8 Develop and Maintain Effectiveness at WorkcarmenNo ratings yet
- Draping, Positioning & Pregnancy Positions: PresentsDocument22 pagesDraping, Positioning & Pregnancy Positions: PresentsАлексNo ratings yet
- Holistic Massage TreatmentDocument5 pagesHolistic Massage TreatmentLawrence Cada Nofies100% (1)
- Massage Therapy List of ToolsDocument7 pagesMassage Therapy List of Toolsandy123_appNo ratings yet
- Massage intake formDocument1 pageMassage intake formTreicy AguileraNo ratings yet
- Client Intake Form - NailsDocument2 pagesClient Intake Form - NailsGGenZ ConsultingNo ratings yet
- Bamboo Massage - An IntroductionDocument9 pagesBamboo Massage - An IntroductionBenjie EugenioNo ratings yet
- Conent Waiver of LiabilityDocument1 pageConent Waiver of Liabilityapi-263560654No ratings yet
- Home Health CodesDocument2 pagesHome Health CodesMia JacksonNo ratings yet
- Types of Massage Techniques ExplainedDocument35 pagesTypes of Massage Techniques ExplainedDuppala Sateesh KumarNo ratings yet
- SF6 - 2022 - 1781764 - Quezon National High SchoolDocument1 pageSF6 - 2022 - 1781764 - Quezon National High SchoolEverly OballoNo ratings yet
- Streamline Unenrollment ProcessDocument8 pagesStreamline Unenrollment ProcessJOHN MARK LAMBINO0% (1)
- Aguinaldo Aquino Garcia Laurel Macapagal Magsaysay Marcos Osmena Quirino RoxasDocument4 pagesAguinaldo Aquino Garcia Laurel Macapagal Magsaysay Marcos Osmena Quirino RoxasEverly OballoNo ratings yet
- Chapter 1-1Document28 pagesChapter 1-1Everly OballoNo ratings yet
- Wellness Massage Module 1-EDITEDDocument17 pagesWellness Massage Module 1-EDITEDEverly OballoNo ratings yet
- Answer Sheet TLE NAIL WELLNESS MASSAGEDocument3 pagesAnswer Sheet TLE NAIL WELLNESS MASSAGEEverly OballoNo ratings yet
- My Teaching PhilosophyDocument4 pagesMy Teaching PhilosophyEverly OballoNo ratings yet
- Wellness Massage ModuleDocument1 pageWellness Massage ModuleEverly OballoNo ratings yet
- MPS Sy 2021-2022Document4 pagesMPS Sy 2021-2022Everly OballoNo ratings yet
- juv-CV (1) FinalDocument2 pagesjuv-CV (1) FinalEverly OballoNo ratings yet
- Cleaning Tools Uses Identification QuizDocument2 pagesCleaning Tools Uses Identification QuizEverly OballoNo ratings yet
- First Quarter Summative Test in Wellness Massage 10 Name: - Grade & SectionDocument2 pagesFirst Quarter Summative Test in Wellness Massage 10 Name: - Grade & SectionEverly OballoNo ratings yet
- Section: Rizal Subject: Adviser: Subject Teacher: Contact NumberDocument14 pagesSection: Rizal Subject: Adviser: Subject Teacher: Contact NumberEverly OballoNo ratings yet
- Reflexology ChartDocument1 pageReflexology ChartEverly OballoNo ratings yet
- Hello Kitty ProgramDocument1 pageHello Kitty ProgramEverly OballoNo ratings yet
- NPT Pipe Thread Sizes and TapersDocument1 pageNPT Pipe Thread Sizes and TapersRajesh J BharadwajNo ratings yet
- Well Rounded.: 360 CassetteDocument12 pagesWell Rounded.: 360 CassetteMonty Va Al MarNo ratings yet
- Partial Discharge - Open ElectricalDocument2 pagesPartial Discharge - Open ElectricalBHALAJI BIRLANo ratings yet
- Thermal Performance of Air-Cooled Condensing Units by CFD SimulationDocument2 pagesThermal Performance of Air-Cooled Condensing Units by CFD SimulationFauziah JeraiNo ratings yet
- RCS England Trainees Guide To A Quality Improvement Project 2021Document17 pagesRCS England Trainees Guide To A Quality Improvement Project 2021Wee K WeiNo ratings yet
- Essotherm 500 PDFDocument8 pagesEssotherm 500 PDFdonyaNo ratings yet
- Bosch EBike Product Catalogue MY2021 enDocument92 pagesBosch EBike Product Catalogue MY2021 enIvanNo ratings yet
- QRP Yu1lm SDR-RX TXDocument299 pagesQRP Yu1lm SDR-RX TXD BNo ratings yet
- Liebert AC4 Controller ManualDocument88 pagesLiebert AC4 Controller ManualGreg WilliamsNo ratings yet
- Manual Hoist ProductsDocument40 pagesManual Hoist Productskavin bhagavathyNo ratings yet
- Rajagiri Public School Unit Test PhysicsDocument3 pagesRajagiri Public School Unit Test PhysicsNITHINKJOSEPHNo ratings yet
- The Future - G&VDocument6 pagesThe Future - G&VManuelHerreraMontoyaNo ratings yet
- Computational Models For Trunk Trajectory Planning and Load Distribution: A Test-Bed For Studying Various Clinical Adaptation and Motor Control Strategies of Low Back Pain PatientsDocument13 pagesComputational Models For Trunk Trajectory Planning and Load Distribution: A Test-Bed For Studying Various Clinical Adaptation and Motor Control Strategies of Low Back Pain PatientsOTorresGonzalezNo ratings yet
- Kyocera Fs-6900 Parts ManualDocument28 pagesKyocera Fs-6900 Parts ManualNic CowpeNo ratings yet
- Am 363 PDFDocument4 pagesAm 363 PDFsunsirNo ratings yet
- 2008 Infosys Model QuestionsDocument23 pages2008 Infosys Model Questionsapi-3824713No ratings yet
- Errata Introduction To Quantum Mechanics, David Griffiths, 2nd Ed.Document3 pagesErrata Introduction To Quantum Mechanics, David Griffiths, 2nd Ed.Marcel BezerraNo ratings yet
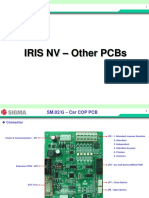
- 07 IRIS NV PCB OtherDocument15 pages07 IRIS NV PCB OtherArnaldo cordovaNo ratings yet
- Brief History About Volley BallDocument1 pageBrief History About Volley BallAmbrad, Merlyn H.No ratings yet
- Basics of Scientific Writing, Scientific Research, and Elementary Data AnalysisDocument12 pagesBasics of Scientific Writing, Scientific Research, and Elementary Data Analysisburhan sabirNo ratings yet
- Pasture FatteningDocument15 pagesPasture FatteningKartika PurnamasariNo ratings yet
- Recycle ProgramDocument2 pagesRecycle ProgramKaps BlazeNo ratings yet
- Experimental Monitoring of The Humber Bridge UsingDocument7 pagesExperimental Monitoring of The Humber Bridge Using정주호No ratings yet