You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Cybersecurity Advisory - Scattered SpiderDocument14 pagesCybersecurity Advisory - Scattered SpiderHendra ArfiantoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sanskrit StoriesDocument28 pagesSanskrit StoriesNikhil Gandhi74% (27)
- Manual Piaggio X9 125 Espanol: Read/DownloadDocument2 pagesManual Piaggio X9 125 Espanol: Read/Downloadjuako0% (4)
- "A Man, A Plan, A Computer: Eric Albert," by Helene HovanecDocument4 pages"A Man, A Plan, A Computer: Eric Albert," by Helene HovanecpspuzzlesNo ratings yet
- Ice ScrambbleDocument15 pagesIce ScrambbleJay ArNo ratings yet
- Cocoa Training Manual PDFDocument122 pagesCocoa Training Manual PDFOlukunle AlabetutuNo ratings yet
- Cadbury UK Limited and Ors Vs Lotte India CorporatD140361COM390343Document14 pagesCadbury UK Limited and Ors Vs Lotte India CorporatD140361COM390343Siddharth soniNo ratings yet
- Final Report Allied BankDocument70 pagesFinal Report Allied BankIfzal Ahmad100% (6)
- Dune v1 002Document36 pagesDune v1 002Ade IrwansyahNo ratings yet
- Completed Unit II 17.7.17Document113 pagesCompleted Unit II 17.7.17Dr.A.R.KavithaNo ratings yet
- PPA StructuringDocument34 pagesPPA StructuringRaj Tha100% (1)
- 7 Direct Cost of Scope Creep in GovernmentalDocument13 pages7 Direct Cost of Scope Creep in GovernmentalBereket MosisaNo ratings yet
- RFC 3193 - Securing L2TP Using IPsecDocument28 pagesRFC 3193 - Securing L2TP Using IPsecAlphariusNo ratings yet
- Management in Problematic SoilsDocument7 pagesManagement in Problematic SoilsBalaji KartheekNo ratings yet
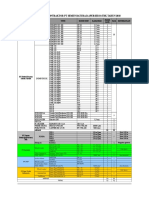
- Populasi Alat Kontraktor PT Semen Baturaja (Persero) TBK Tahun 2018Document1 pagePopulasi Alat Kontraktor PT Semen Baturaja (Persero) TBK Tahun 2018Dwiki KurniawanNo ratings yet
- Lecture 2 - FrequencyDocument35 pagesLecture 2 - Frequencypt.22.132No ratings yet
- 802-CBN-00-PR-CE-LIFTING PROCEDURE-049-B of Civil Construction and Infrastructure Works, Stage 2Document12 pages802-CBN-00-PR-CE-LIFTING PROCEDURE-049-B of Civil Construction and Infrastructure Works, Stage 2Agus SupriadiNo ratings yet
- Khizer Javed: Warehouse, Logistics & Supply ChainDocument5 pagesKhizer Javed: Warehouse, Logistics & Supply ChainAlmeenay HussainNo ratings yet
- Premier 300Document2 pagesPremier 300Malitha PeirisNo ratings yet
- A Vision-Based Method For The Detection of Missing Rail FastenersDocument6 pagesA Vision-Based Method For The Detection of Missing Rail FastenersShivaprasad.b.kNo ratings yet
- English Paper 1 UPSRDocument20 pagesEnglish Paper 1 UPSRCynthia Theseira100% (2)
- Design Process of Energy Effective Shredding Machines For Biomass TreatmentDocument5 pagesDesign Process of Energy Effective Shredding Machines For Biomass TreatmentAhmed ShawkiNo ratings yet
- Static Aeroelasticity: I H I I BL H L H U LL LL L Ul I I L U I I L 1Document1 pageStatic Aeroelasticity: I H I I BL H L H U LL LL L Ul I I L U I I L 1OSCARDELTANo ratings yet
- NN43001-106-B1 05.01 Fundamentals Features and ServicesDocument606 pagesNN43001-106-B1 05.01 Fundamentals Features and ServicesNashriq NashNo ratings yet
- Meet Zhang YimingDocument5 pagesMeet Zhang YimingJhuliane RalphNo ratings yet
- Cap 344.table of ContentDocument4 pagesCap 344.table of ContentPikying CheungNo ratings yet
- 2017-03-31 CEG To DOJ (Anti-Magnitsky FARA Violations)Document106 pages2017-03-31 CEG To DOJ (Anti-Magnitsky FARA Violations)Andrew JordanNo ratings yet
- Transdermal Drug Delivery System ReviewDocument8 pagesTransdermal Drug Delivery System ReviewParth SahniNo ratings yet
- Chapter I IntroductionDocument17 pagesChapter I IntroductionAdnan MazariNo ratings yet
- Executive Summary DOP Submrsible Dredge PumpDocument24 pagesExecutive Summary DOP Submrsible Dredge PumpingartgNo ratings yet