You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Blueprints QA Pediatrics For Step 3 1Document59 pagesBlueprints QA Pediatrics For Step 3 1Moataz Trabeh100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 978 3 659 75192 9 PDFDocument298 pages978 3 659 75192 9 PDFshravan38No ratings yet
- Chapter 1 - Introduction To GeologyDocument37 pagesChapter 1 - Introduction To GeologynnsNo ratings yet
- RE-DUAL PCI: Dual Antithrombotic Therapy With Dabigatran After Percutaneous Coronary Intervention in Patients With Atrial FibrillationDocument20 pagesRE-DUAL PCI: Dual Antithrombotic Therapy With Dabigatran After Percutaneous Coronary Intervention in Patients With Atrial FibrillationMoataz TrabehNo ratings yet
- Acute Promyelocytic LeukemiaDocument16 pagesAcute Promyelocytic LeukemiaMoataz TrabehNo ratings yet
- English Tests For Infectious DiseasesDocument82 pagesEnglish Tests For Infectious DiseasesMoataz TrabehNo ratings yet
- Ghicavîi Victor: - Name: Creliciuc Maria - Age: 64ani (15/04/1949) - Location: KishinauDocument30 pagesGhicavîi Victor: - Name: Creliciuc Maria - Age: 64ani (15/04/1949) - Location: KishinauMoataz TrabehNo ratings yet
- Corticosteroids For Treatment of Sore Throat: Systematic Review and Meta-Analysis of Randomised Trials BMJ 2017Document13 pagesCorticosteroids For Treatment of Sore Throat: Systematic Review and Meta-Analysis of Randomised Trials BMJ 2017Moataz TrabehNo ratings yet
- 5 Reticuolocyte CountDocument11 pages5 Reticuolocyte CountMoataz TrabehNo ratings yet
- TTTTDocument26 pagesTTTTMoataz TrabehNo ratings yet
- 8 - Anti Allergic DrugsDocument8 pages8 - Anti Allergic DrugsMoataz TrabehNo ratings yet
- B-Selective: I Group: Nonsteroidal Anti-Inflammatory Drugs (Nonsteroidal Ntiinflammatory)Document6 pagesB-Selective: I Group: Nonsteroidal Anti-Inflammatory Drugs (Nonsteroidal Ntiinflammatory)Moataz TrabehNo ratings yet
- 13 - Antibiotic III Nalidixic AcidDocument7 pages13 - Antibiotic III Nalidixic AcidMoataz TrabehNo ratings yet
- 1 DiurethicsDocument8 pages1 DiurethicsMoataz TrabehNo ratings yet
- Imle A 03 03 2015Document82 pagesImle A 03 03 2015Moataz TrabehNo ratings yet
- 05.psychiatry Fixed by E.G E.KDocument54 pages05.psychiatry Fixed by E.G E.KMoataz Trabeh100% (1)
- 5 Digestive IDocument11 pages5 Digestive IMoataz TrabehNo ratings yet
- PediatricsDocument84 pagesPediatricsMoataz TrabehNo ratings yet
- 2012 f550 Manual PDFDocument450 pages2012 f550 Manual PDFJuma RefaccionariasNo ratings yet
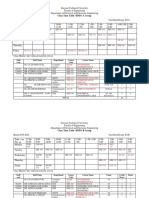
- HND-Class Time Table 1.1Document7 pagesHND-Class Time Table 1.1rajalingamNo ratings yet
- Data Dependences: CS 524 - High-Performance ComputingDocument20 pagesData Dependences: CS 524 - High-Performance Computingmarifs2002No ratings yet
- Köppen Climate Classification PDFDocument21 pagesKöppen Climate Classification PDFJohann S M MendezNo ratings yet
- Temperature of Mass ConcreteDocument41 pagesTemperature of Mass Concreterahmat amaik0% (1)
- IECEx CML 17.0023X 0Document9 pagesIECEx CML 17.0023X 0KittyNo ratings yet
- Fun Projects 02 ChapterDocument3 pagesFun Projects 02 ChaptertihomihoNo ratings yet
- CamNorte APTCDocument17 pagesCamNorte APTCStella Marie VillagenNo ratings yet
- Thesis About Zero Waste ManagementDocument6 pagesThesis About Zero Waste Managementpattyjosephpittsburgh100% (2)
- Crystallinity and Transition Temperatures in PolymersDocument46 pagesCrystallinity and Transition Temperatures in PolymersghenisNo ratings yet
- Assignment For Diwali BreakDocument16 pagesAssignment For Diwali BreakArshNo ratings yet
- Neogene PeriodDocument20 pagesNeogene PeriodErikh James MestidioNo ratings yet
- Finfet: (Fin Shaped Field Effect Transistor)Document14 pagesFinfet: (Fin Shaped Field Effect Transistor)Harish Kumar PuvvadaNo ratings yet
- Gen Chem 2Document2 pagesGen Chem 2Trisha Camille MacarioNo ratings yet
- HS8251 2marks - by WWW - Learnengineering.inDocument21 pagesHS8251 2marks - by WWW - Learnengineering.inDwaranath SrinivasanNo ratings yet
- Stress Corrosion Cracking PDFDocument48 pagesStress Corrosion Cracking PDFPako RosasNo ratings yet
- 09 082Document22 pages09 082Gerson FloresNo ratings yet
- Schneider Sustainability Deck 05.23.23Document16 pagesSchneider Sustainability Deck 05.23.23SchneiderNo ratings yet
- 湖北省武汉外国语学校2023 2024学年高一上学期阶段性诊断测试英语试卷Document9 pages湖北省武汉外国语学校2023 2024学年高一上学期阶段性诊断测试英语试卷yun xingNo ratings yet
- Hyrule Warriors - Age of Calamity - Weapons & Resources (Comments Enabled)Document20 pagesHyrule Warriors - Age of Calamity - Weapons & Resources (Comments Enabled)꧁TAKAYUKINo ratings yet
- Factors and Multiples #NotesDocument12 pagesFactors and Multiples #NotesVijayalakshmi ISAMNo ratings yet
- In The Living Room Furniture Prepositions of Place CLT Communicative Language Teaching Resources Fun 89740Document13 pagesIn The Living Room Furniture Prepositions of Place CLT Communicative Language Teaching Resources Fun 89740Алена ТерскаяNo ratings yet
- Wakatipu Trails MapDocument2 pagesWakatipu Trails Mapmiller999No ratings yet
- The Advantages & Disadvantages of Using Biological Weapons For TerrorismDocument6 pagesThe Advantages & Disadvantages of Using Biological Weapons For TerrorismChenideNo ratings yet
- Group 6Document10 pagesGroup 6LINDOHNo ratings yet
- Optoma ES522 (DP-2400) EX532 (DP-3400) ServiceManual 20090630Document123 pagesOptoma ES522 (DP-2400) EX532 (DP-3400) ServiceManual 20090630Rafael PlazaNo ratings yet
- Dallas Music Shop Zagreb CD LagerDocument174 pagesDallas Music Shop Zagreb CD Lagervjeran rukavinaNo ratings yet
- Skoda Maintenance Package - Terms and Conditions DocumentDocument1 pageSkoda Maintenance Package - Terms and Conditions DocumentSuman SahaNo ratings yet