THE SULTAN REVIEW
GROUP
3RD FLR. HIGHLAND LUMBER BLDG. #2213-2219 ESPAÑA BLVD.,
SAMPALOC, MANILA
LANDLINE: 731-0677 / 731-0642 MOBILE: 09178360123
EMAIL: sultanreviewgroup@gmail.com
WEBSITE: www.sultanreviewgroup.net
SRG E-Learning NPTE Module: Gait Analysis
Gait
qualitative term
rhythmical alternating movement of UE (reciprocal arm swing) and LE with trunk
Gait cycle
quantitative term
heel strike of one foot to heel strike of the same foot
functional unit of gait
Other name: Stride length: Normal: 30 inches vs. Step length – Heel strike of one foot to heel strike of the
opposite foot: N: 30 inches
Sinusoidal
Elements/Variables in Gait analysis:
1. Kinematics – ROM, position
2. Kinetics – Internal kinetics – muscle responsible
i. Hip – Flexors (iliopsoas); Extensors (gluteus maximus)
ii. Knee – Quadriceps Femoris; hamstrings
iii. Ankle – Pre-tibials; Gastrocnemius-Soleus Complex
-- External Kinetics – Ground Reaction Force (moment)
*Concentric movements: power and speed
*Eccentric movements: controlled, slow, antagonist of ground reaction force
Ground Reaction Force
ANT POST
Hip F E
Knee E F
Ankle D PF
STANCE VS. SWING
Stance: 60% of Gait Cycle
Swing: 40% of Gait Cycle
Traditional Rancho Los Amigos
Heel strike Initial Contact
Footflat Loading Response
STANCE Midstance Midstance
Heel off Terminal stance
Toe off Pre-swing
Acceleration Initial swing
SWING Midswing Mid-swing
Deceleration Terminal swing
SINGLE VS. DOUBLE SUPPORT
Single support: 80 %
Double support: 20 %
Part of the gait cycle with the lowest COG (muscle don’t spend much energy)
o To avoid decrease in COG: pelvis rotation (4 deg on each side)
o Versus: Highest COG: Midstance
To avoid increase in COG: pelvic list, drop, tilt (any determinant that INC COG is
occurring at midstance)
Gluteus medius & Gluteus minimus (2 mm, 4 deg) peak of activity
SRG E-Learning NPTE Module: Gait Analysis
This material is for the exclusive use of SULTAN REVIEW GROUP and its students. No part of this material may be reproduced
without permission from SULTAN REVIEW GROUP.
GAIT ANALYSIS
HIP KNEE ANKLE
Heel strike 30 F Ecc of G E Ecc of Ham Neutral Con of PT
Foot flat 20 F Ecc of G 20 F Ecc of Quad 15 PF Ecc of PT
Midstance N 10-15 F Ecc of Quad 5 DF Ecc of Calf
Heel off 10 HE Ecc of IP 0 15 DF Ecc of Calf
Toe off 20 HE Ecc of IP 40 F Ecc of Quad 20 Con of Calf
Acceleration N Con of IP 50 F Con of Ham N Con of PT
Midswing 20 F Con of IP 60 F Con of Ham N Con of PT
Deceleration 30 F Ecc of G E Ecc of Ham N Con of PT
PEAK OF ACTIVITY
HIP
Iliopsoas: Toe off: to oppose flexor moment: 2 nd: initial swing
Gluteus Maximus: Heel strike to oppose extensor moment
KNEE
Quadriceps: After heelstrike; @ toe off
Hamstrings: Deceleration
ANKLE
Pre-tibials:After heel trike foot slapping
Steppage gait: during swing compensatory increase hip and knee flexion
Gastroc-Soleus Complex: Push-off calcaneal gait – no push off
SRG E-Learning NPTE Module: Gait Analysis
This material is for the exclusive use of SULTAN REVIEW GROUP and its students. No part of this material may be reproduced
without permission from SULTAN REVIEW GROUP.
DETERMINANTS OF GAIT
1. Pelvic rotation
Period of double support on stance side
INC COG
INC step length
2. Heel rise
DEC COG
6-8 mm
3. Pelvic tilt/list; pelvic obliquity
COG 2 mm; Gmed & Gmin
4. Knee flexion on stance phase
DEC COG
5. Ankle foot mechanism
F E
Knee DF PF
Eve Inv
6. Lateral displacement of the pelvis
Side to side
Movement of pelvis on stance side
PATHOLOGIC GAIT
A. Ankle
a. Foot slap – after heelstrike; weakness of Pre-tibials
b. Foot drag - swing
c. Steppage gait – swing; compensatory (excessive hip and knee flexion)
d. Equinus gait – toes first (PT paralysis)
e. Calcaneal gait – (-) push off (GS complex paralysis)
B. Knee
a. Buckling gait – after heel strike; Quadriceps weakness; Femoral nerve lesion
b. Cheerleader’s gait – toe off; to prevent foot from reaching thigh
c. Stiff knee: no decelaration; weak hamstrings
d. Genu recurvatum Swedish Knee Cage
i. PF spasticity
ii. Achilles tendon shortening
iii. Quads spasticity
iv. Hamstring weakness
e. Excessive knee flexion
i. DF spasticity
ii. PF weakness
iii. Hamstring contracture
iv. Quadriceps weakness
v. Long limbs
vi. Hip flexion contracture
C. Others
a. Lurching gait/Jacknife gait: heel strike; weakness of Gmax compensation: hyperextension of trunk
b. Gmed gait: Unilateral: Trendelenburg; Bilateral: Waddling gait/wobbling gait/maewest gait
c. Antalgic Gait: due to pain
i. DEC stance
ii. DEC step length
d. Psoatic Limp: FABER; LCPD
e. Ataxic Gait: Motor or sensory – awkward gait
i. Motor: cerebellum; hypotonicity; station gait/staggering gait/drummer’s gait
ii. Sensory: posterior column: tabetic gait/gait of spinal ataxia
f. Parkinsonian gait
i. Festinating gait
ii. Shuffling gait
g. Circumduction Gait/Helicopad
i. Hip hiking with circumduction
SRG E-Learning NPTE Module: Gait Analysis
This material is for the exclusive use of SULTAN REVIEW GROUP and its students. No part of this material may be reproduced
without permission from SULTAN REVIEW GROUP.
ii. Arthrogenic Gait (stiff hip and knee gait)
NORMAL:
1. Cadence: 90-120 steps per minute; INC in Females
2. Walking speed: 3ph
3. Toe out: 7 degrees; DEC in INC speed of walking
SRG E-Learning NPTE Module: Gait Analysis
This material is for the exclusive use of SULTAN REVIEW GROUP and its students. No part of this material may be reproduced
without permission from SULTAN REVIEW GROUP.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- TL Design Manual - Rev0.5Document64 pagesTL Design Manual - Rev0.5Syed Ahsan Ali Sherazi100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Astable MultivibratorDocument38 pagesAstable MultivibratorSherry Sher0% (1)
- Idustrial Q & ADocument6 pagesIdustrial Q & ARegie SalidagaNo ratings yet
- MEC 4402 LAB 2 Speed Characteristics of The Ricardo E.6 EngineDocument10 pagesMEC 4402 LAB 2 Speed Characteristics of The Ricardo E.6 EngineJoseph Mwansa100% (1)
- 2 Quarter: Understanding OverexertionDocument15 pages2 Quarter: Understanding OverexertionJhon Keneth NamiasNo ratings yet
- Trimix Injection InstructionsDocument3 pagesTrimix Injection InstructionsInfolad1No ratings yet
- Biomedicines 11 00128Document13 pagesBiomedicines 11 00128dmandatari7327No ratings yet
- Foster Wheeler ContractsDocument29 pagesFoster Wheeler ContractsCane Cirpo100% (1)
- Legal Medicine Questionaire MendiolaDocument5 pagesLegal Medicine Questionaire MendiolaBhell MendiolaNo ratings yet
- Iteration Method NotesDocument13 pagesIteration Method Notes20-317 RithvikNo ratings yet
- Jurol Sbo StudilitDocument6 pagesJurol Sbo Studilitmarcellino wijayaNo ratings yet
- Mohamed Yr 10 Physics Exam (Midterm)Document15 pagesMohamed Yr 10 Physics Exam (Midterm)victor bettNo ratings yet
- Moana Movie ReviewDocument3 pagesMoana Movie ReviewChazmin SantosNo ratings yet
- A Colorimetric Method For The Determination of Serum Glutamic Oxalacetic and Glutamic Pyruvic TransaminasesDocument8 pagesA Colorimetric Method For The Determination of Serum Glutamic Oxalacetic and Glutamic Pyruvic TransaminasesTuan NguyenNo ratings yet
- Three-Phase Tefc High Efficiency Motor: Eff1 / Ie2Document8 pagesThree-Phase Tefc High Efficiency Motor: Eff1 / Ie2Gea Mandiri ciptaNo ratings yet
- SIDEROS - Down Draft TablesDocument2 pagesSIDEROS - Down Draft TablesDaniel AustinNo ratings yet
- Relative Strangers by Paula Garner Chapter SamplerDocument39 pagesRelative Strangers by Paula Garner Chapter SamplerCandlewick PressNo ratings yet
- Adambakkam 2 StreetDocument16 pagesAdambakkam 2 StreetManiNo ratings yet
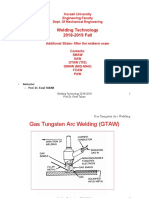
- Welding Technology GTAW GMAW FCAW PAW Nov 2020Document87 pagesWelding Technology GTAW GMAW FCAW PAW Nov 2020ENZO PEREZNo ratings yet
- ABENDI & ASME Workshop - N Finney W Hembree - Section VDocument114 pagesABENDI & ASME Workshop - N Finney W Hembree - Section VMarciel AmorimNo ratings yet
- An Efficient Micropropagation Protocol For Eclipta AlbaDocument6 pagesAn Efficient Micropropagation Protocol For Eclipta AlbaSuprabuddha KunduNo ratings yet
- Chapter-2 PERCEPTIONDocument29 pagesChapter-2 PERCEPTIONSuman BhandariNo ratings yet
- Space Gamer 05 PDFDocument16 pagesSpace Gamer 05 PDFsam mckenzieNo ratings yet
- Guidelines/acute Diarrhea/acute Diarrhea EnglishDocument4 pagesGuidelines/acute Diarrhea/acute Diarrhea EnglishBLOK 16 Angkatan 2018No ratings yet
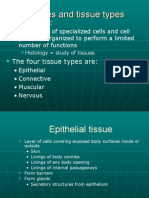
- Tissues and Tissue TypesDocument42 pagesTissues and Tissue TypesMustafa Akbar100% (1)
- Texila American University: Article Review GuidelineDocument10 pagesTexila American University: Article Review GuidelinecindyNo ratings yet
- 40 Cau Part 5 Kem Loi Giai Chi TietDocument14 pages40 Cau Part 5 Kem Loi Giai Chi TietTrần DũngNo ratings yet
- POLS235 Exam 1Document6 pagesPOLS235 Exam 1defran 262No ratings yet
- Introduction To Probability TheoryDocument207 pagesIntroduction To Probability TheoryRahulNo ratings yet
- UntitledDocument6 pagesUntitledBrenda M. Martínez GonzálezNo ratings yet