You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- An Introduction To Thermal Physics - 1Document237 pagesAn Introduction To Thermal Physics - 1PranayYadav100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- XRD Test1 title under 40 charsDocument6 pagesXRD Test1 title under 40 charsChuah Chong YangNo ratings yet
- EML500 Instruction ManualDocument85 pagesEML500 Instruction Manualtoumassis_p100% (5)
- 1.4 Notes - Even and Odd FunctionsDocument2 pages1.4 Notes - Even and Odd FunctionsJohn MixerNo ratings yet
- Small Animal Dosimetry Dosimetric Models vs. Specific DosimetryDocument58 pagesSmall Animal Dosimetry Dosimetric Models vs. Specific DosimetryMadalina-Elena CostacheNo ratings yet
- The Activity Calibrator: A.O.U. "Ospedali Riuniti" Di Trieste S.C. Di Fisica SanitariaDocument36 pagesThe Activity Calibrator: A.O.U. "Ospedali Riuniti" Di Trieste S.C. Di Fisica SanitariaMadalina-Elena CostacheNo ratings yet
- Introduction To Microdosimetry!: Manuel Bardiès, INSERM UMR 892, Nantes, France Manuel - Bardies@Document32 pagesIntroduction To Microdosimetry!: Manuel Bardiès, INSERM UMR 892, Nantes, France Manuel - Bardies@Madalina-Elena CostacheNo ratings yet
- Monday, 12 April Tuesday, 13 April Wednesday, 14 AprilDocument1 pageMonday, 12 April Tuesday, 13 April Wednesday, 14 AprilMadalina-Elena CostacheNo ratings yet
- Topics: Introduction To PET PhysicsDocument22 pagesTopics: Introduction To PET PhysicsMadalina-Elena CostacheNo ratings yet
- B D I T Bexxar Dosimet Ttry: George Sgouros, Ph.D. G GDocument34 pagesB D I T Bexxar Dosimet Ttry: George Sgouros, Ph.D. G GMadalina-Elena CostacheNo ratings yet
- 3D-RD Imaging-D I T Dosimetry - Based: George Sgouros, Ph.D. G GDocument40 pages3D-RD Imaging-D I T Dosimetry - Based: George Sgouros, Ph.D. G GMadalina-Elena CostacheNo ratings yet
- Extranodal Involvment in LymphomaDocument15 pagesExtranodal Involvment in LymphomaMadalina-Elena CostacheNo ratings yet
- Wayne Dyer4Document205 pagesWayne Dyer4Cristian Catalina100% (3)
- Wayne Dyer4Document205 pagesWayne Dyer4Cristian Catalina100% (3)
- Beta Emitters Dosimetry at the Microscopic ScaleDocument39 pagesBeta Emitters Dosimetry at the Microscopic ScaleMadalina-Elena CostacheNo ratings yet
- Table of RadionucleidsDocument311 pagesTable of RadionucleidsompsdaNo ratings yet
- Mehmet T. Kitapci (Auth.) - Atlas of Sectional Radiological Anatomy For PET - CT-Springer-Verlag New York (2012)Document121 pagesMehmet T. Kitapci (Auth.) - Atlas of Sectional Radiological Anatomy For PET - CT-Springer-Verlag New York (2012)Florentina MovilaNo ratings yet
- Pediatric RadiotherapyDocument365 pagesPediatric RadiotherapyMadalina-Elena Costache100% (1)
- Numerical Integration MethodsDocument6 pagesNumerical Integration MethodsOsama HassanNo ratings yet
- Intermolecular Forces: Types and IdentificationDocument9 pagesIntermolecular Forces: Types and IdentificationRadzmiya SulaymanNo ratings yet
- Newton's Cart LabDocument4 pagesNewton's Cart LabMartin MeierNo ratings yet
- Chapter II Fluid MachineryDocument90 pagesChapter II Fluid MachineryFad TajudinNo ratings yet
- MT BitsDocument12 pagesMT BitsKundan KumarNo ratings yet
- Linear Combination and Dependence of VectorsDocument5 pagesLinear Combination and Dependence of VectorsPragathi SundarNo ratings yet
- Effect of Substituents On Basicity of PyridineDocument5 pagesEffect of Substituents On Basicity of PyridineMehar SanaNo ratings yet
- Aircraft Basics and PerformanceDocument21 pagesAircraft Basics and Performanced_gunaNo ratings yet
- Some Parametric Solutions To The Navier-Lame Equation in Cylindrical Coordinates Using Buchwald Displacement PotentialsDocument30 pagesSome Parametric Solutions To The Navier-Lame Equation in Cylindrical Coordinates Using Buchwald Displacement PotentialsraveneyesdeadNo ratings yet
- Full Syllabus Neet Test 2Document23 pagesFull Syllabus Neet Test 2Tanmay Barui100% (1)
- 1 Reaction KineticsDocument41 pages1 Reaction KineticsZIAJIANo ratings yet
- IartDocument141 pagesIartbelenNo ratings yet
- Theory of Machine Student ManualDocument72 pagesTheory of Machine Student ManualWellington LimaNo ratings yet
- Spherical CoordinatesDocument7 pagesSpherical CoordinatesEdvardo PagvaiNo ratings yet
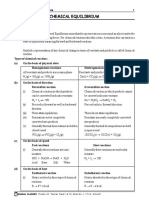
- Chemical Equilibrium ExplainedDocument68 pagesChemical Equilibrium Explainedhappy100% (1)
- Jee 2003Document61 pagesJee 2003BHOOMI BNo ratings yet
- Circular Motion GuideDocument10 pagesCircular Motion GuideEdgardo Leysa100% (1)
- Flow Instrumentation 101: Dave SchmittDocument62 pagesFlow Instrumentation 101: Dave SchmittAhmed HusseinNo ratings yet
- Catia BookDocument207 pagesCatia Bookfightsquad100% (2)
- ESP - Steag Session 1 Part 1Document40 pagesESP - Steag Session 1 Part 1bharath attaluriNo ratings yet
- MCQ's Chap 12Document4 pagesMCQ's Chap 12Arham MunirNo ratings yet
- Chapter 1Document99 pagesChapter 1Hariharan C.VNo ratings yet
- Ch1 Introduction Heat PDFDocument44 pagesCh1 Introduction Heat PDFSaritha devi VoddepalliNo ratings yet
- Ward Leonard Product BrochureDocument69 pagesWard Leonard Product Brochuregold_mundoNo ratings yet
- Bond Work Index Report AnalysisDocument5 pagesBond Work Index Report AnalysisalinoriNo ratings yet
- Belt FrictionDocument2 pagesBelt FrictionMuhammad HaziqNo ratings yet