You might also like
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Advarse Drug ReactionDocument9 pagesAdvarse Drug ReactionAyanNo ratings yet
- Clin Pharmacy ADRDocument24 pagesClin Pharmacy ADRAnonymous DgPsK0oQNo ratings yet
- Clin Pharmacy ADRDocument36 pagesClin Pharmacy ADRAnonymous DgPsK0oQNo ratings yet
- Adverse Drug Reactions 23 24 1Document37 pagesAdverse Drug Reactions 23 24 1Hasan kahhalehNo ratings yet
- Adverse Eeffects of Drugs and Their Management in PaediatricsDocument6 pagesAdverse Eeffects of Drugs and Their Management in PaediatricsRinchin ChhotenNo ratings yet
- Adr NewDocument43 pagesAdr Newshyamsundermaurya987No ratings yet
- ADRs - Classification, Mechanism, Predisposing Factors & Causality AssessmentDocument7 pagesADRs - Classification, Mechanism, Predisposing Factors & Causality AssessmentAman UpadhyayNo ratings yet
- Adverse Eeffects of Drugs and Their Management in PaediatricsDocument6 pagesAdverse Eeffects of Drugs and Their Management in PaediatricsRinchin ChhotenNo ratings yet
- PHARMACOVIGILANCEDocument46 pagesPHARMACOVIGILANCEshak4567100% (3)
- Pharmaco Vig Gi LanceDocument34 pagesPharmaco Vig Gi Lancebagir_dm10No ratings yet
- A Presentation On Adr Due To AntibioitcsDocument18 pagesA Presentation On Adr Due To AntibioitcsAnta SharmaNo ratings yet
- Adverse Drug ReactionDocument6 pagesAdverse Drug ReactionBilwaBhavendraNo ratings yet
- IndexDocument3 pagesIndexAasNo ratings yet
- Adr and ManagementDocument48 pagesAdr and ManagementDhanush G V DhanushNo ratings yet
- Adverse Drug Reactions and InteractionsDocument6 pagesAdverse Drug Reactions and InteractionsAlvina HafidiatiNo ratings yet
- ADR Final1Document10 pagesADR Final1Rubina BisankheNo ratings yet
- Monitoring Efek Samping Obat (MESO)Document25 pagesMonitoring Efek Samping Obat (MESO)Nienies NurikaNo ratings yet
- Adverse Drug Reactions: BackgroundDocument10 pagesAdverse Drug Reactions: BackgroundPat YenNo ratings yet
- Cardiovascular Drugs May Cause Oral Adverse ReactionsDocument19 pagesCardiovascular Drugs May Cause Oral Adverse ReactionsSuci RahmiNo ratings yet
- Adverse Drug Reaction-Causality Assessment: International Journal of Research in Pharmacy and ChemistryDocument7 pagesAdverse Drug Reaction-Causality Assessment: International Journal of Research in Pharmacy and ChemistryLalo MaldonadoNo ratings yet
- AbriefguidetoadrsDocument5 pagesAbriefguidetoadrsSri HariNo ratings yet
- Adverse Drug Reactions: Sudhakar LakavathDocument41 pagesAdverse Drug Reactions: Sudhakar LakavathSudhakar LakavathNo ratings yet
- Adverse Drug Reactions ExplainedDocument41 pagesAdverse Drug Reactions ExplainedPopi Sopiah100% (1)
- Adversedrugreactionmonitoringandreporting Pertemuan 14-15Document33 pagesAdversedrugreactionmonitoringandreporting Pertemuan 14-15Ani RahayuNo ratings yet
- Improving Patient Care: Clarifying Adverse Drug Events: A Clinician's Guide To Terminology, Documentation, and ReportingDocument8 pagesImproving Patient Care: Clarifying Adverse Drug Events: A Clinician's Guide To Terminology, Documentation, and ReportingAgustiantyNo ratings yet
- PharmacologyDocument5 pagesPharmacologySaqline MondalNo ratings yet
- Guidance On Adverse Drug ReactionsDocument5 pagesGuidance On Adverse Drug Reactionssoraoto arashinaNo ratings yet
- RRLDocument30 pagesRRLbealinniNo ratings yet
- Adr Management and MonitoringDocument5 pagesAdr Management and MonitoringRaju NiraulaNo ratings yet
- Drug Interaction:: Age, GeneticsDocument87 pagesDrug Interaction:: Age, GeneticsMiranda MetriaNo ratings yet
- Adrs 150226194556 Conversion Gate02Document56 pagesAdrs 150226194556 Conversion Gate02Ayu WijiNo ratings yet
- Principles of Drug Therapy For The Elderly PatientDocument16 pagesPrinciples of Drug Therapy For The Elderly PatientGalih Maygananda Putra100% (1)
- Adverse Drug Reactions: Key PointsDocument6 pagesAdverse Drug Reactions: Key PointsOvi RifaniNo ratings yet
- E151 Medicationerrors-QJMDocument10 pagesE151 Medicationerrors-QJMRestu AriyusNo ratings yet
- Adverse Drug Reactions ExplainedDocument71 pagesAdverse Drug Reactions ExplainedVaibhav ThoratNo ratings yet
- AdrDocument9 pagesAdrvizzladNo ratings yet
- Ksmu Department of Clinical PharmacologyDocument15 pagesKsmu Department of Clinical PharmacologyLucas Victor AlmeidaNo ratings yet
- Adverse Drug ReactionDocument7 pagesAdverse Drug ReactionufahadNo ratings yet
- ADRs, Reporting and Causality AssessmentDocument37 pagesADRs, Reporting and Causality AssessmentRaymond ManjengwaNo ratings yet
- Adverse Drug ReactionsDocument21 pagesAdverse Drug ReactionsRohit100% (1)
- 1.adverse Drug ReactionDocument42 pages1.adverse Drug ReactionSV. Trần Hữu ThắngNo ratings yet
- Pharmacogenomics:: Increasing The Safety and Effectiveness of Drug TherapyDocument12 pagesPharmacogenomics:: Increasing The Safety and Effectiveness of Drug TherapyFlorentina GasttiNo ratings yet
- Medication Error PDFDocument61 pagesMedication Error PDFChelsea Ritz MendozaNo ratings yet
- Adverse Drug Reactions ExplainedDocument108 pagesAdverse Drug Reactions ExplainedBinod Sah100% (2)
- Clinical Pharmacology IntroductionDocument24 pagesClinical Pharmacology IntroductionSunilNo ratings yet
- ADR Monitoring and ReportingDocument13 pagesADR Monitoring and ReportingKinjal GamitNo ratings yet
- Adverse Drug Reactions NotesDocument4 pagesAdverse Drug Reactions NoteskarthikeyanpgtNo ratings yet
- Clinical Therapeutics and Drug-Induced DiseaseDocument4 pagesClinical Therapeutics and Drug-Induced DiseasewaterprincessNo ratings yet
- 13 - Adverse Drug Reactions CausesDocument4 pages13 - Adverse Drug Reactions CausesRojas Evert AlonsoNo ratings yet
- Pharmacodynamics: BIOL 122 DR Hemant MehtaDocument13 pagesPharmacodynamics: BIOL 122 DR Hemant MehtaRavinder KaurNo ratings yet
- E151 Medicationerrors-QJMDocument10 pagesE151 Medicationerrors-QJMWens BambutNo ratings yet
- PharmacovigilanceDocument43 pagesPharmacovigilanceTanoy SahaNo ratings yet
- Brief Notes On PharmacovigilanceDocument78 pagesBrief Notes On Pharmacovigilancejay100% (1)
- ADRsDocument56 pagesADRsFarina FaraziNo ratings yet
- Hospital Formulary: Astralis Medical GroupDocument36 pagesHospital Formulary: Astralis Medical GroupJade MBNo ratings yet
- Introduction To Pharmacokinetics and Pharmacodynamics 2022Document20 pagesIntroduction To Pharmacokinetics and Pharmacodynamics 2022احمد علىNo ratings yet
- Drug Hypersensitivity: Mja Practice Essentials - AllergyDocument6 pagesDrug Hypersensitivity: Mja Practice Essentials - AllergyFrida AnggaNo ratings yet
- 6 ABC of Drug-Related Problems PDFDocument9 pages6 ABC of Drug-Related Problems PDFMadalinaMadaNo ratings yet
- 1.adverse Drug ReactionsDocument18 pages1.adverse Drug ReactionsVitalis MbuyaNo ratings yet
- PMDT 2017 Doctors Training ListDocument1 pagePMDT 2017 Doctors Training Listgaikwaduv98No ratings yet
- AICDocument6 pagesAICgaikwaduv98No ratings yet
- Adverse Drug ReactionsDocument14 pagesAdverse Drug Reactionsgaikwaduv98No ratings yet
- Adverse Drug ReactionsDocument14 pagesAdverse Drug Reactionsgaikwaduv98No ratings yet
- AICDocument6 pagesAICgaikwaduv98No ratings yet
- BLS & AclsDocument29 pagesBLS & AclswcgokulNo ratings yet
- Chapter 17 Pulmonary HypertensionDocument10 pagesChapter 17 Pulmonary HypertensionSuwandi AlghozyNo ratings yet
- National Guidelines For Management of Animal BitesDocument10 pagesNational Guidelines For Management of Animal Bitesgaikwaduv98No ratings yet
- ADR Reportin SOPDocument12 pagesADR Reportin SOPgaikwaduv98No ratings yet
- Q.C in YemenDocument6 pagesQ.C in YemenWafa BadullaNo ratings yet
- Drug Excipients InteractionDocument19 pagesDrug Excipients InteractionHussein Talal KenaanNo ratings yet
- Uniformity of Dosage Units BP 2011 & USP 34Document26 pagesUniformity of Dosage Units BP 2011 & USP 34Anonymous SDUIPeqXNo ratings yet
- Epoprostenol Important Information About Change in Formulation of FlolanDocument5 pagesEpoprostenol Important Information About Change in Formulation of FlolanNur FitrianaNo ratings yet
- Benadryl N Tagamet Dose and Frequency ChartDocument1 pageBenadryl N Tagamet Dose and Frequency Chartrjkl6No ratings yet
- Email worksheet for license renewal applicationDocument42 pagesEmail worksheet for license renewal applicationHazel BisaNo ratings yet
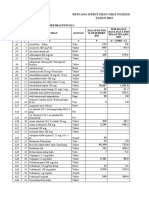
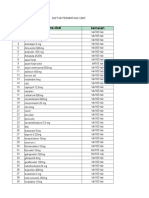
- Rencana Kebutuhan Obat Puskesmas Tahun 2023Document33 pagesRencana Kebutuhan Obat Puskesmas Tahun 2023Putu LitariNo ratings yet
- Flugal DS NewDocument1 pageFlugal DS NewshakilNo ratings yet
- Disintegration TestingDocument9 pagesDisintegration TestingganeshaexactNo ratings yet
- Email Worksheet Application Form OverviewDocument15 pagesEmail Worksheet Application Form OverviewdrchughNo ratings yet
- Efavirenz Chem OlympicsDocument1 pageEfavirenz Chem OlympicsdreamingsnowNo ratings yet
- Drug InteractionDocument18 pagesDrug InteractionBp hoNo ratings yet
- Web Non Subsidized Fully Manufactured LocallyDocument16 pagesWeb Non Subsidized Fully Manufactured LocallyA GhNo ratings yet
- Improving Drug Candidates by Design: Focus on Physicochemical PropertiesDocument37 pagesImproving Drug Candidates by Design: Focus on Physicochemical PropertiesBen ZoeNo ratings yet
- Bulan Februari 2022Document45 pagesBulan Februari 2022Yogie 1290No ratings yet
- Drug Inspection SchedulingDocument4 pagesDrug Inspection SchedulingpdgcssNo ratings yet
- 6th Sem SyllabusDocument20 pages6th Sem SyllabusManish YadavNo ratings yet
- Final Feedback European Medicine Agency Ema Eu Commission Request Evaluate Impact Removal Titanium - enDocument11 pagesFinal Feedback European Medicine Agency Ema Eu Commission Request Evaluate Impact Removal Titanium - enValentin ParaschivNo ratings yet
- DSP 16 - 08 - 23Document34 pagesDSP 16 - 08 - 23Iffa FelasyifaNo ratings yet
- Anti Retro Viral Drugs ClassificationDocument19 pagesAnti Retro Viral Drugs Classification王慧媚100% (1)
- Quintus SlidesCarnivalDocument103 pagesQuintus SlidesCarnivalmiles sbNo ratings yet
- Stok 05 Februari 2022 Ogb KFDocument36 pagesStok 05 Februari 2022 Ogb KFAy u Purnama WijayantiNo ratings yet
- Investigational DrugsDocument25 pagesInvestigational Drugsamjad.46987No ratings yet
- Permintaan Obat Bulan April 2023Document8 pagesPermintaan Obat Bulan April 2023Putri Nurma SariNo ratings yet
- 2010-2014 B.Pharm Course Schedules and Subject DetailsDocument9 pages2010-2014 B.Pharm Course Schedules and Subject DetailsHimanshu GuptaNo ratings yet
- Prescription: Aneri Desai Department of PharmaceuticsDocument31 pagesPrescription: Aneri Desai Department of Pharmaceuticsaneri desaiNo ratings yet
- Painkillers 5.9.12Document4 pagesPainkillers 5.9.12Saerom Yoo EnglandNo ratings yet
- Approved Drug Products 2012 SuplimDocument46 pagesApproved Drug Products 2012 SuplimMada madalinaNo ratings yet
- Consumer guide to Pharmaniaga Paracetamol TabletDocument2 pagesConsumer guide to Pharmaniaga Paracetamol TabletWei HangNo ratings yet
- UntitledDocument2 pagesUntitledarevicNo ratings yet
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryFrom EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNo ratings yet
- Easyway Express: Stop Smoking and Quit E-CigarettesFrom EverandEasyway Express: Stop Smoking and Quit E-CigarettesRating: 5 out of 5 stars5/5 (15)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildFrom EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildRating: 3.5 out of 5 stars3.5/5 (9)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionFrom EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionRating: 4.5 out of 5 stars4.5/5 (2)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsFrom EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNo ratings yet
- Sober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholFrom EverandSober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholRating: 4.5 out of 5 stars4.5/5 (127)
- Stop Drinking Now: The original Easyway methodFrom EverandStop Drinking Now: The original Easyway methodRating: 5 out of 5 stars5/5 (28)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Breathing Under Water: Spirituality and the Twelve StepsFrom EverandBreathing Under Water: Spirituality and the Twelve StepsRating: 4.5 out of 5 stars4.5/5 (41)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionFrom EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionRating: 5 out of 5 stars5/5 (63)
- Total Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDFrom EverandTotal Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDRating: 4 out of 5 stars4/5 (8)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousFrom EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousRating: 5 out of 5 stars5/5 (22)
- Drop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)From EverandDrop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)Rating: 4.5 out of 5 stars4.5/5 (52)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerFrom EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerRating: 5 out of 5 stars5/5 (8)
- Food of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionFrom EverandFood of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionRating: 4.5 out of 5 stars4.5/5 (117)
- Drunk-ish: A Memoir of Loving and Leaving AlcoholFrom EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholRating: 4 out of 5 stars4/5 (6)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.From EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Rating: 4 out of 5 stars4/5 (7)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingFrom EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingRating: 5 out of 5 stars5/5 (11)
- The Language of Letting Go: Daily Meditations on CodependencyFrom EverandThe Language of Letting Go: Daily Meditations on CodependencyRating: 4.5 out of 5 stars4.5/5 (18)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryFrom EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryRating: 5 out of 5 stars5/5 (47)