You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Beyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDocument54 pagesBeyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDilan GalaryNo ratings yet
- Retinoids in Dermatology: History, Mechanism and Clinical UsesDocument86 pagesRetinoids in Dermatology: History, Mechanism and Clinical UsesDilan GalaryNo ratings yet
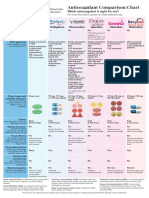
- Anticoagulant Comparison Chart: Which Anticoagulant Is Right For Me?Document1 pageAnticoagulant Comparison Chart: Which Anticoagulant Is Right For Me?Dilan GalaryNo ratings yet
- Simple PPS Form For Step 1.9Document1 pageSimple PPS Form For Step 1.9Dilan GalaryNo ratings yet
- CTC 72017Document1,662 pagesCTC 72017Dilan GalaryNo ratings yet
- Checklist Patient SafetyDocument15 pagesChecklist Patient SafetyKatherine Conlu Bengan100% (1)
- Rosuvastatin2012 017 PDFDocument17 pagesRosuvastatin2012 017 PDFDilan GalaryNo ratings yet
- CTC7 - Sample Chapter - Insomnia PDFDocument15 pagesCTC7 - Sample Chapter - Insomnia PDFFarid AhmedNo ratings yet
- Ivfluid Glines AdultDocument2 pagesIvfluid Glines AdultDilan Galary100% (1)
- AAEM RSA50DrugFactsEveryEPShouldKnow PDFDocument52 pagesAAEM RSA50DrugFactsEveryEPShouldKnow PDFalaam mahmoudNo ratings yet
- Intravenous Fluid Therapy in Adults in Hospital Algorithm Poster Set 191627821Document5 pagesIntravenous Fluid Therapy in Adults in Hospital Algorithm Poster Set 191627821Wira Sasmita P100% (1)
- Multiple SclerosisDocument20 pagesMultiple SclerosisDilan GalaryNo ratings yet
- CEBM Levels of Evidence 2.1Document1 pageCEBM Levels of Evidence 2.1Béla TóthNo ratings yet
- 2019apixaban PDFDocument9 pages2019apixaban PDFDilan GalaryNo ratings yet
- 2016 2017 Antimicrobial GuideDocument77 pages2016 2017 Antimicrobial GuideDee DeeNo ratings yet
- MesalazineDocument2 pagesMesalazineDilan GalaryNo ratings yet
- Ada PDFDocument204 pagesAda PDFMario BarbozaNo ratings yet
- Non Steroidal Anti-Inflammatory Drugs (NSAIDs)Document16 pagesNon Steroidal Anti-Inflammatory Drugs (NSAIDs)Dilan GalaryNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cover Letter and Thank You Letter ExamplesDocument7 pagesCover Letter and Thank You Letter Examplesf675ztsf100% (2)
- Risk Management Framework and ProcessDocument16 pagesRisk Management Framework and ProcessIuliana T.No ratings yet
- Civ Pro I - 2011 TahaDocument27 pagesCiv Pro I - 2011 TahaACDCNo ratings yet
- LM1 Toc 25141Document1 pageLM1 Toc 25141Sotiris AthinaiosNo ratings yet
- The Myth of Scientific Miracles in The KoranDocument13 pagesThe Myth of Scientific Miracles in The KoranDoctor Jones33% (3)
- Dokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFDocument2 pagesDokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFPayal SethiNo ratings yet
- BS en 01062-3-2008 PDFDocument12 pagesBS en 01062-3-2008 PDFjohnNo ratings yet
- Burwitz Teaching ResumeDocument2 pagesBurwitz Teaching Resumeapi-300437677No ratings yet
- Public Service Commission, West Bengal: Notice Inviting Expression of Interest For Enlistment As LawyersDocument3 pagesPublic Service Commission, West Bengal: Notice Inviting Expression of Interest For Enlistment As LawyersITI JobNo ratings yet
- Guided Reading Assessment The Giraffe Pelly and Me p19 38Document4 pagesGuided Reading Assessment The Giraffe Pelly and Me p19 38Joshua JamesNo ratings yet
- Background Surya NepalDocument11 pagesBackground Surya NepalUjibpradhan67% (3)
- Assessment 2 Stat20053 Descriptive Statistics - CompressDocument2 pagesAssessment 2 Stat20053 Descriptive Statistics - CompressDon RatbuNo ratings yet
- Challenges in Sensory Integration and Processing in The Child WithDocument6 pagesChallenges in Sensory Integration and Processing in The Child WithDanyela SchlosserNo ratings yet
- Huntington, The Hispanic Challenge PDFDocument17 pagesHuntington, The Hispanic Challenge PDFUguccionepisaNo ratings yet
- Lecture 2 2014 Random Errors in Chemical AnalysisDocument24 pagesLecture 2 2014 Random Errors in Chemical AnalysisRobert EdwardsNo ratings yet
- Labman PDFDocument76 pagesLabman PDFJames OnsachiNo ratings yet
- The Killing Fields of Assam: Myth and Reality of Its Muslim ImmigrationDocument10 pagesThe Killing Fields of Assam: Myth and Reality of Its Muslim ImmigrationAlHittin100% (1)
- WtA - 01 - Forgotten Lessons PDFDocument8 pagesWtA - 01 - Forgotten Lessons PDFHyperion DriverNo ratings yet
- Tang Re CIA 2 enDocument20 pagesTang Re CIA 2 enDimitris TsagkoudisNo ratings yet
- APES Tragedy of The Commons Lab Activity: Purpose: ObjectiveDocument4 pagesAPES Tragedy of The Commons Lab Activity: Purpose: ObjectivejakeingerNo ratings yet
- Ch1 - Part I - Meaning of ResearchDocument36 pagesCh1 - Part I - Meaning of ResearchKirubel MulugetaNo ratings yet
- Mr. Doherty Builds His Dream LifeDocument32 pagesMr. Doherty Builds His Dream LifeglacenatNo ratings yet
- ReportDocument3 pagesReportPrecious Anne MacalinoNo ratings yet
- Environmental Sustainability Assessment of An Academic Institution in Calamba CityDocument29 pagesEnvironmental Sustainability Assessment of An Academic Institution in Calamba CityAmadeus Fernando M. PagenteNo ratings yet
- Nicholas Kaldor On Adam Smith and Allyn Young: Review of Political EconomyDocument20 pagesNicholas Kaldor On Adam Smith and Allyn Young: Review of Political EconomyAdolfo MedranoNo ratings yet
- Solution Manual For Introductory Econometrics A Modern Approach 5th Edition by WooldridgeDocument35 pagesSolution Manual For Introductory Econometrics A Modern Approach 5th Edition by Wooldridgecarter.tweese.8gud100% (40)
- Historical CriticismDocument1 pageHistorical CriticismPatricia Ann Dulce Ambata67% (3)
- FCE - Exam: B2 First For SchoolsDocument26 pagesFCE - Exam: B2 First For SchoolsNele Loubele PrivateNo ratings yet
- Guía BaccettiDocument11 pagesGuía BaccettiPercy Andree Bayona GuillermoNo ratings yet
- Racionalidad Acotada 1Document4 pagesRacionalidad Acotada 1Hector J. RubiniNo ratings yet