You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
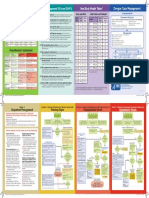
- DengueCheatSheet ENG-PDocument2 pagesDengueCheatSheet ENG-PSilva Neta OktariNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- JR Analisis Faktor ASLI PDFDocument8 pagesJR Analisis Faktor ASLI PDFSilva Neta OktariNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Journal of Air Transport Management: Anne Graham, Frances Kremarik, Willy KruseDocument5 pagesJournal of Air Transport Management: Anne Graham, Frances Kremarik, Willy KruseSilva Neta OktariNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- JR Analisis Faktor ASLI PDFDocument8 pagesJR Analisis Faktor ASLI PDFSilva Neta OktariNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Benefit of Minocycline On Negative Symptoms PDFDocument10 pagesThe Benefit of Minocycline On Negative Symptoms PDFSilva Neta OktariNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- PR A Comparison of The Dose of Anesthetic Agents and The Effective Interval From The Block Procedure To Skin Incision For Ultrasound-Guided Supraclavicular Brachial Plexus Block in UpperDocument4 pagesPR A Comparison of The Dose of Anesthetic Agents and The Effective Interval From The Block Procedure To Skin Incision For Ultrasound-Guided Supraclavicular Brachial Plexus Block in UpperSilva Neta OktariNo ratings yet
- Resume Mini Cex SILVA CholelitiasisDocument3 pagesResume Mini Cex SILVA CholelitiasisSilva Neta OktariNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Chi Et Al-2017-Journal of The European Academy of Dermatology and VenereologyDocument13 pagesChi Et Al-2017-Journal of The European Academy of Dermatology and VenereologySilva Neta OktariNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Glucose and Insulin-Related Traits, Type 2 Diabetes and RiskDocument7 pagesGlucose and Insulin-Related Traits, Type 2 Diabetes and RiskSilva Neta OktariNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Tak SosialisasiDocument10 pagesTak SosialisasidwiajaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Articles: BackgroundDocument13 pagesArticles: BackgroundSilva Neta OktariNo ratings yet
- Calcitonin As An Analgesic Agent Review of Mechanisms of Action and Clinical Applications PDFDocument11 pagesCalcitonin As An Analgesic Agent Review of Mechanisms of Action and Clinical Applications PDFSilva Neta OktariNo ratings yet
- Glucose and Insulin-Related Traits, Type 2 Diabetes and RiskDocument7 pagesGlucose and Insulin-Related Traits, Type 2 Diabetes and RiskSilva Neta OktariNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Benefit of Minocycline On Negative Symptoms PDFDocument10 pagesThe Benefit of Minocycline On Negative Symptoms PDFSilva Neta OktariNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Benefit of Minocycline On Negative SymptomsDocument10 pagesThe Benefit of Minocycline On Negative SymptomsSilva Neta OktariNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nasopharyngeal Branchial CystDocument2 pagesNasopharyngeal Branchial CystSilva Neta OktariNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Dry EyeDocument22 pagesDry EyeSilva Neta Oktari100% (1)
- A Sense of BelongingDocument107 pagesA Sense of BelongingVijayalaxmi N. Varnekar80% (15)
- Asynch Module 1 Hum102Document2 pagesAsynch Module 1 Hum102Aphaedes AlcalaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Best Antonyms and Synonyms For SSC CGLDocument13 pagesBest Antonyms and Synonyms For SSC CGLSiddharth Jain100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mini Lesson 8 - UranusDocument2 pagesMini Lesson 8 - Uranuscaity_andrews17No ratings yet
- Friend, hobby, holiday memoriesDocument4 pagesFriend, hobby, holiday memoriesHiếu Nguyễn Minh100% (2)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Introduction To Psychology 10th Edition Plotnik Test Bank 1Document38 pagesIntroduction To Psychology 10th Edition Plotnik Test Bank 1norma100% (47)
- Religious ExperienceDocument53 pagesReligious ExperienceDO BY100% (1)
- Teen MarriageDocument23 pagesTeen MarriageDeneshwaran Balarajan0% (1)
- Administrative and Labour Law Syllabus: Industrial Organization Engineering Degree Academic Year 2012-2013Document8 pagesAdministrative and Labour Law Syllabus: Industrial Organization Engineering Degree Academic Year 2012-2013Antonio Ignacio Jimenez LopezNo ratings yet
- Ehli Daimonion 2017Document17 pagesEhli Daimonion 2017Vojtěch HladkýNo ratings yet
- Chapter - 2 Advertising and SemioticsDocument28 pagesChapter - 2 Advertising and Semioticsanon_589589998100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- More 2 Cyber Homework CambridgeDocument7 pagesMore 2 Cyber Homework Cambridgeafeutvfeg100% (1)
- My Application Letter (Kharisma)Document6 pagesMy Application Letter (Kharisma)Ica AnnisaNo ratings yet
- Children's Use of Technology and Social MediaDocument5 pagesChildren's Use of Technology and Social MediaJunel SildoNo ratings yet
- English Short Daily LiturgyDocument3 pagesEnglish Short Daily LiturgyAs Serpentes Comem CacaNo ratings yet
- Sorbom, Dag (1974)Document11 pagesSorbom, Dag (1974)evgtsNo ratings yet
- Hbo Final ExamDocument1 pageHbo Final ExambebensonNo ratings yet
- Deleuze Studies, Volume 1 Issue 2Document102 pagesDeleuze Studies, Volume 1 Issue 2Aragorn EloffNo ratings yet
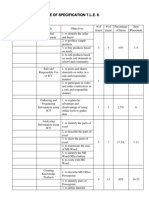
- Table of Specification T.L.E. 6Document3 pagesTable of Specification T.L.E. 6Autumn Thorn SebastianNo ratings yet
- HR Policy For Hotel IndustriesDocument5 pagesHR Policy For Hotel IndustriesHR Forum India78% (9)
- Addressing Workplace Harassment Through Policy ReformDocument10 pagesAddressing Workplace Harassment Through Policy ReformNo FaNo ratings yet
- SHS Alumni Hall of Fame Nomination FormDocument2 pagesSHS Alumni Hall of Fame Nomination FormjtwatsonkyNo ratings yet
- Chapter Scheme & Synopsis GuidelinesDocument8 pagesChapter Scheme & Synopsis GuidelinesVishwa N100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Employee Development and Growth - InditexDocument7 pagesEmployee Development and Growth - Inditexquanghao1991No ratings yet
- Scribd For Self-Improvement: A Roadmap To Personal GrowthDocument2 pagesScribd For Self-Improvement: A Roadmap To Personal GrowthABDESSALEM AGHRIBNo ratings yet
- Unit 3Document11 pagesUnit 3banaz.aliNo ratings yet
- Organizational DevelopmentDocument12 pagesOrganizational DevelopmentShara Tumambing MA PsyNo ratings yet
- The Power of Courtesy: How Politeness Can Gain Respect, Inspire Kindness and Strengthen RelationshipsDocument3 pagesThe Power of Courtesy: How Politeness Can Gain Respect, Inspire Kindness and Strengthen Relationshipswardah farainNo ratings yet
- Paranthropology Vol 2 No 3Document64 pagesParanthropology Vol 2 No 3Jack Hunter100% (1)
- The Ultimate Tarot JournalDocument47 pagesThe Ultimate Tarot Journalbelnyc92% (77)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)