You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ray Huang - 1587 - A Year of No Significance - The Ming Dynasty in Decline-Yale University Press (1982)Document309 pagesRay Huang - 1587 - A Year of No Significance - The Ming Dynasty in Decline-Yale University Press (1982)Saint NarcissusNo ratings yet
- MH0ihh081h6754910230616041100202 PDFDocument2 pagesMH0ihh081h6754910230616041100202 PDFLogan GoadNo ratings yet
- Castlevania d20Document387 pagesCastlevania d20Logan Goad100% (1)
- PLANIT Group - Code of Business Ethics and Conduct PolicyDocument10 pagesPLANIT Group - Code of Business Ethics and Conduct PolicyLogan GoadNo ratings yet
- Castlevania d20Document387 pagesCastlevania d20Logan Goad100% (1)
- Drug Screening Consent Form 2014Document1 pageDrug Screening Consent Form 2014Logan GoadNo ratings yet
- Manual: DE User InformationDocument48 pagesManual: DE User InformationOliprayer PopcornianNo ratings yet
- Lithomancer PDFDocument5 pagesLithomancer PDFLogan GoadNo ratings yet
- Lithomancer PDFDocument5 pagesLithomancer PDFLogan GoadNo ratings yet
- Central Ozarks Medical Center: Consent For Patient PortalDocument1 pageCentral Ozarks Medical Center: Consent For Patient PortalLogan GoadNo ratings yet
- Creature Loot PDF - GM Binder PDFDocument96 pagesCreature Loot PDF - GM Binder PDFLogan Goad88% (8)
- Animal AdaptationsDocument17 pagesAnimal AdaptationsStacy Koesser100% (1)
- BULLET SWAGING SUPPLY 8.5x11Document1 pageBULLET SWAGING SUPPLY 8.5x11Ramon BrazNo ratings yet
- CV M Haekal Jimi FariziDocument1 pageCV M Haekal Jimi FariziFariz QintharaNo ratings yet
- The Modernization of Iran and The Development of The Persian Carpet Industry The Neo-Classical Era in The Persian Carpet Industry 1925 - 45Document29 pagesThe Modernization of Iran and The Development of The Persian Carpet Industry The Neo-Classical Era in The Persian Carpet Industry 1925 - 45miguel6789No ratings yet
- Esquire - October 2016 UKDocument180 pagesEsquire - October 2016 UKSpuxyNo ratings yet
- Magnification SystemsDocument8 pagesMagnification Systemsgalal2720006810No ratings yet
- Story: No Word Function English Meaning Pashto Meaning ExampleDocument29 pagesStory: No Word Function English Meaning Pashto Meaning ExampleMuhammad Ab BariNo ratings yet
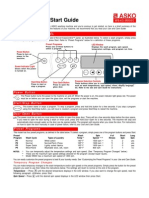
- ASKO Washer Quick Start GuideDocument2 pagesASKO Washer Quick Start GuideJim FischerNo ratings yet
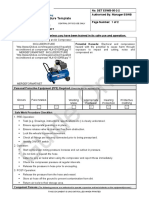
- Air Compressor ProcedureDocument2 pagesAir Compressor ProcedurePerwez21No ratings yet
- Full Circle Skirt - Make A Circle Skirt Pattern! - The Creative CuratorDocument27 pagesFull Circle Skirt - Make A Circle Skirt Pattern! - The Creative CuratorDamaris G100% (1)
- Mems PDFDocument136 pagesMems PDFadelll lNo ratings yet
- Ancient Finnish CostumesDocument69 pagesAncient Finnish CostumesGulyás Bence100% (1)
- New Nicu Blue BookDocument17 pagesNew Nicu Blue BookYatin Mehta100% (1)
- WWW Successcds Net Cce Cbse Class Xii English The Rattrap HTMLDocument36 pagesWWW Successcds Net Cce Cbse Class Xii English The Rattrap HTMLLolo MutuNo ratings yet
- Black Wings and Stolen Things - Kayleigh KingDocument490 pagesBlack Wings and Stolen Things - Kayleigh Kingmisbah shahid0% (3)
- Atlanta Apparel2012.SmlDocument64 pagesAtlanta Apparel2012.Smlzoomerfins22No ratings yet
- 1.put The Verbs Into The Correct Form, Past Continuous or Past SimpleDocument4 pages1.put The Verbs Into The Correct Form, Past Continuous or Past SimplemarianNo ratings yet
- FOREVER YOURS by Mdutyana NonkoloDocument517 pagesFOREVER YOURS by Mdutyana NonkoloAmanda t mbawaNo ratings yet
- Orn37 2 HeardmuseumfairDocument4 pagesOrn37 2 Heardmuseumfairapi-275090135No ratings yet
- Gà2Document9 pagesGà2Le Thi Thanh Van100% (4)
- Industrial Music and CultureDocument12 pagesIndustrial Music and CultureMarina Busic100% (2)
- Tide Fact Sheet EDUQASDocument4 pagesTide Fact Sheet EDUQASsarahledwidge1No ratings yet
- Trioflex Datasheet English 01Document2 pagesTrioflex Datasheet English 01jonodo89No ratings yet
- PRIMARY RESEARCH TERM 3 (AutoRecovered)Document5 pagesPRIMARY RESEARCH TERM 3 (AutoRecovered)Hà HảiNo ratings yet
- Where Is Hefty HidingDocument16 pagesWhere Is Hefty HidingericmanhonchanNo ratings yet
- (WotLK 3.3.5) Resto Shaman Gearing by TeamyDocument48 pages(WotLK 3.3.5) Resto Shaman Gearing by TeamyFerdi VaroroNo ratings yet
- ONW4-01 - Prisoners of WarDocument73 pagesONW4-01 - Prisoners of WarRafael França100% (1)
- Black Suits You - Novoneel ChakrabortyDocument221 pagesBlack Suits You - Novoneel ChakrabortyEshita AgarwalNo ratings yet