You might also like
- Gale Researcher Guide for: Overview of Sleep and Dreams in PsychologyFrom EverandGale Researcher Guide for: Overview of Sleep and Dreams in PsychologyNo ratings yet
- The Importance of Sleep for Normal Function and SurvivalDocument11 pagesThe Importance of Sleep for Normal Function and SurvivalSaravanan Jagan25% (4)
- Sleep and Other Interruptions of ConsciousnessDocument5 pagesSleep and Other Interruptions of ConsciousnessJovelyn NacinNo ratings yet
- States of ConsciousnessDocument3 pagesStates of ConsciousnessJoanne TolopiaNo ratings yet
- Harvard Health Guide to Sleep Stages and CyclesDocument11 pagesHarvard Health Guide to Sleep Stages and CyclesMariaNo ratings yet
- What Happens When You SleepDocument28 pagesWhat Happens When You SleepNaresh LalwaniNo ratings yet
- Biopsychology Report On SLEEPDocument31 pagesBiopsychology Report On SLEEPpsychcookieNo ratings yet
- Sleep and Sleep Disorders: Velayudhan Mohan KumarDocument8 pagesSleep and Sleep Disorders: Velayudhan Mohan KumarmeiutaNo ratings yet
- SleepDocument28 pagesSleepapi-534716659No ratings yet
- Sleep and RestDocument85 pagesSleep and RestJann ericka Jao100% (2)
- JC - How Sleep WorksDocument40 pagesJC - How Sleep WorksLe RaNo ratings yet
- (... Continued From REM Sleep & Remembering Dreams PT 1Document4 pages(... Continued From REM Sleep & Remembering Dreams PT 1nawazNo ratings yet
- Overview of Sleep DisordersDocument16 pagesOverview of Sleep DisordersRNo ratings yet
- Consciousness: # IntroDocument7 pagesConsciousness: # IntroDaizy DharewalNo ratings yet
- Suprachiasmatic Nucleus (SCN) - Clusters of Thousands of Cells That Receive Information AboutDocument7 pagesSuprachiasmatic Nucleus (SCN) - Clusters of Thousands of Cells That Receive Information AboutChiun Er AngNo ratings yet
- PAP VMK IndJChestDisDocument9 pagesPAP VMK IndJChestDisSmahil RNo ratings yet
- ITP-States of ConsciousnessDocument17 pagesITP-States of ConsciousnesspopiscanzNo ratings yet
- Day 11 Passage 2 SleepDocument3 pagesDay 11 Passage 2 SleepShahlo SattorovaNo ratings yet
- Sleep PresentationDocument25 pagesSleep PresentationmonicaNo ratings yet
- EEG Normal Sleep - StatPearls - NCBI BookshelfDocument7 pagesEEG Normal Sleep - StatPearls - NCBI BookshelfChandan ShandilNo ratings yet
- SLEEPDocument45 pagesSLEEPHemanth SNo ratings yet
- SLEEPDocument19 pagesSLEEPRegimae BartolomeNo ratings yet
- Brain Basics: Understanding Sleep: Sleep: A Dynamic ActivityDocument10 pagesBrain Basics: Understanding Sleep: Sleep: A Dynamic ActivitymonicaNo ratings yet
- Sleep - DMPDocument53 pagesSleep - DMPdharitri100% (1)
- What is consciousness and stages of sleepDocument6 pagesWhat is consciousness and stages of sleepSiobhan CorbettNo ratings yet
- The Effects of Sleep Deprivation Among CDocument38 pagesThe Effects of Sleep Deprivation Among CKate RefermosoNo ratings yet
- UNIT 1 Sleep & Rest-PatternDocument57 pagesUNIT 1 Sleep & Rest-Patternab tubeNo ratings yet
- SleepDocument31 pagesSleepSreelakshmi MsNo ratings yet
- Understanding Sleep: Essential for Well-BeingDocument9 pagesUnderstanding Sleep: Essential for Well-BeingsuviacesoNo ratings yet
- Phases of Sleep and Nervous SystemDocument12 pagesPhases of Sleep and Nervous SystemAsad SafdarNo ratings yet
- Sleep: Sleep Can Be Defined As A Normal State of Altered Consciousness DuringDocument17 pagesSleep: Sleep Can Be Defined As A Normal State of Altered Consciousness DuringappuvayalaNo ratings yet
- States of Brain Activity-: Sleep, Brain Waves, Epilepsy, PsychosesDocument60 pagesStates of Brain Activity-: Sleep, Brain Waves, Epilepsy, PsychosesashupathakaNo ratings yet
- PsychologyessayDocument4 pagesPsychologyessayThanh Thảo Huỳnh ThịNo ratings yet
- Sleep Disorders Lecture NotesDocument9 pagesSleep Disorders Lecture Notesrupal aroraNo ratings yet
- DR Steven Lin - The Five Stages of Sleep and Brain Wave CyclesDocument22 pagesDR Steven Lin - The Five Stages of Sleep and Brain Wave CyclesChristina SuhadiNo ratings yet
- Unit 9 - Sleep and Wakefulness... NotesDocument10 pagesUnit 9 - Sleep and Wakefulness... NotesKristine Nicole FloresNo ratings yet
- Sleep and its disturbances: An overviewDocument83 pagesSleep and its disturbances: An overviewSatbir GillNo ratings yet
- Why We Need Sleep: Biological Rhythms and RestorationDocument7 pagesWhy We Need Sleep: Biological Rhythms and RestorationVivek KushwahaNo ratings yet
- Chapter 5Document28 pagesChapter 5Mehroob CheemaNo ratings yet
- Overview of Sleep & Sleep Disorders: Review ArticleDocument15 pagesOverview of Sleep & Sleep Disorders: Review ArticlePrima Akli SetyoNo ratings yet
- Project SleepDocument6 pagesProject SleepDan Emanuel AntonesăNo ratings yet
- Brain Basics Sleep 6 10 08 PDF 508 PDFDocument16 pagesBrain Basics Sleep 6 10 08 PDF 508 PDFYrah Gaille VasquezNo ratings yet
- ConsciousnessDocument43 pagesConsciousnessSaiNo ratings yet
- Brs Lesson 4 - Ultradian RhytmsDocument11 pagesBrs Lesson 4 - Ultradian Rhytmsapi-288749075No ratings yet
- SleepDocument14 pagesSleepmoiezsatyaniNo ratings yet
- How the Brain Experiences Sleep and DreamsDocument3 pagesHow the Brain Experiences Sleep and DreamsVianca EpinoNo ratings yet
- Sleep Deprivation: Dr. Abdul-Monim Batiha Assistant Professor Critical Care Nursing Philadelphia UniversityDocument90 pagesSleep Deprivation: Dr. Abdul-Monim Batiha Assistant Professor Critical Care Nursing Philadelphia UniversityJyotiNo ratings yet
- Neural Circuitry of Wakefulness and SleepDocument40 pagesNeural Circuitry of Wakefulness and Sleepribamar CoutinhoNo ratings yet
- Psych Chapter 9 HeheDocument11 pagesPsych Chapter 9 Hehemadeline.carter22No ratings yet
- Ibrahim - Qossay BM Case Analysis: Almer Viquiera CabidaDocument8 pagesIbrahim - Qossay BM Case Analysis: Almer Viquiera CabidaQusai BassamNo ratings yet
- An Analysis of The Benefits and Advantages of NREM3 SleepDocument6 pagesAn Analysis of The Benefits and Advantages of NREM3 Sleepapi-635102354No ratings yet
- Alvászavar És MigrénDocument10 pagesAlvászavar És MigrénLindenberger BoriszNo ratings yet
- Assignment Pengantar PsikologiDocument8 pagesAssignment Pengantar PsikologiMitzshawn Fairy's IVNo ratings yet
- Sleep Disorders - Lecture Notes 13: Clinical Psychology (Bournemouth University)Document10 pagesSleep Disorders - Lecture Notes 13: Clinical Psychology (Bournemouth University)rupal aroraNo ratings yet
- Introduction To Psychology Version 3 0 3rd Stangor Solution ManualDocument11 pagesIntroduction To Psychology Version 3 0 3rd Stangor Solution ManualBradGonzalezrgeys100% (46)
- ASSIGNMENT OF ENDOCRINOLOGYDocument12 pagesASSIGNMENT OF ENDOCRINOLOGYSaba RiazNo ratings yet
- 3 EdbDocument8 pages3 Edbshiv shankarNo ratings yet
- 3 EdbDocument8 pages3 Edbshiv shankarNo ratings yet
- CBSE Class 12 Chemistry - Alchohols, Phenols and Ethers Chapter Notes PDFDocument10 pagesCBSE Class 12 Chemistry - Alchohols, Phenols and Ethers Chapter Notes PDFshiv shankarNo ratings yet
- New Doc 2019-09-05 12.31.23-1Document2 pagesNew Doc 2019-09-05 12.31.23-1shiv shankarNo ratings yet
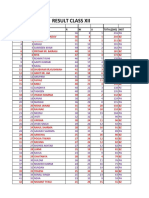
- ResultDocument2 pagesResultshiv shankarNo ratings yet
- Optical Fibre: Physics Investigatory ProjectDocument22 pagesOptical Fibre: Physics Investigatory ProjectSurendar MVNo ratings yet
- Chap2 Physics Top 10Document2 pagesChap2 Physics Top 10AL SuryaNo ratings yet
- Physics Investigatory Project (XII) Tangent GalvanometerDocument16 pagesPhysics Investigatory Project (XII) Tangent Galvanometermuskaan2270% (105)
- Investigatory ProjectDocument16 pagesInvestigatory Projectlittl miss72% (18)
- Professional EthicsDocument2 pagesProfessional EthicsKoushik MeduriNo ratings yet
- ISnack - Sec A Group6Document11 pagesISnack - Sec A Group6Avik BorahNo ratings yet
- A History of The Methodist Episcopal Church Volume I (Nathan D.D.bangs)Document244 pagesA History of The Methodist Episcopal Church Volume I (Nathan D.D.bangs)Jaguar777xNo ratings yet
- Roulette WarfareDocument2 pagesRoulette WarfareAsteboNo ratings yet
- Concept of Peace in Peace Studies: A Short Historical SketchDocument14 pagesConcept of Peace in Peace Studies: A Short Historical SketchTrieu Huy HaNo ratings yet
- 1988 Ojhri Camp Disaster in PakistanDocument3 pages1988 Ojhri Camp Disaster in PakistanranasohailiqbalNo ratings yet
- R69 Sepulveda V PelaezDocument2 pagesR69 Sepulveda V PelaezfranceheartNo ratings yet
- Prosthetics OrthoticsDocument9 pagesProsthetics OrthoticsSameeha AbbassNo ratings yet
- The Impact of Cultural Intelligence On Global BusinessDocument5 pagesThe Impact of Cultural Intelligence On Global BusinessAna Mihaela IstrateNo ratings yet
- Reflection Chap 07Document3 pagesReflection Chap 07Fizza JunaidNo ratings yet
- Gomez FL Bar Complaint v. PerezDocument6 pagesGomez FL Bar Complaint v. PerezJudgeHSNo ratings yet
- Demand for E-ZPass and Gas GuzzlersDocument11 pagesDemand for E-ZPass and Gas GuzzlersYonn Me Me KyawNo ratings yet
- Conditions of Contract For: ConstructionDocument30 pagesConditions of Contract For: Constructionvladimir100% (2)
- Presentation1 150221070554 Conversion Gate01Document75 pagesPresentation1 150221070554 Conversion Gate01yellymarlianapatuNo ratings yet
- BS NursingDocument5 pagesBS NursingDenise Louise PoNo ratings yet
- Math 7 - Week 2 SummativeDocument1 pageMath 7 - Week 2 SummativeBrian Mary0% (1)
- Building Machine Learning Systems With Python - Second Edition - Sample ChapterDocument32 pagesBuilding Machine Learning Systems With Python - Second Edition - Sample ChapterPackt PublishingNo ratings yet
- Eco 2203-1 (Notes To Date)Document102 pagesEco 2203-1 (Notes To Date)Joseph KhaembaNo ratings yet
- In Partial Fulfilment of The Requirements in Research Methods ClassDocument10 pagesIn Partial Fulfilment of The Requirements in Research Methods ClasstaniatotsNo ratings yet
- Element Six v. Novatek Et. Al.Document26 pagesElement Six v. Novatek Et. Al.PriorSmartNo ratings yet
- Written Assignment Week 4Document5 pagesWritten Assignment Week 4Thai50% (2)
- Sources of Strength For Mental Wellness by Sheryl Boswell, Youth Mental Health Canada (YMHC)Document11 pagesSources of Strength For Mental Wellness by Sheryl Boswell, Youth Mental Health Canada (YMHC)Youth Mental Health CanadaNo ratings yet
- Vibrational Behaviour of The Turbo Generator Stator End Winding in CaseDocument12 pagesVibrational Behaviour of The Turbo Generator Stator End Winding in Casekoohestani_afshin50% (2)
- Guia de Instrucciones para Piloto - Garmin 1000Document57 pagesGuia de Instrucciones para Piloto - Garmin 1000Cesar Gaspar BaltazarNo ratings yet
- Duration of Labor: Group1Document19 pagesDuration of Labor: Group1ABEGAIL BALLORANNo ratings yet
- SysEng 5212-EE5370 Course Outline Spring 2017Document4 pagesSysEng 5212-EE5370 Course Outline Spring 2017Bojian CaoNo ratings yet
- Success Factors For Augmented Reality Business ModelsDocument36 pagesSuccess Factors For Augmented Reality Business ModelsAsutosh GuptaNo ratings yet
- The Irrefutable Laws of Leadership SummaryDocument6 pagesThe Irrefutable Laws of Leadership Summarycoachersland100% (3)
- Foreigners, Pharaonic Egypt: Kate LiszkaDocument3 pagesForeigners, Pharaonic Egypt: Kate LiszkaSongNo ratings yet
- Oxford Quantum Theory Lecture NotesDocument92 pagesOxford Quantum Theory Lecture Notest ElderNo ratings yet