You might also like
- NASM-CPT Study Guide: Domain 1: Basic and Applied Sciences andDocument49 pagesNASM-CPT Study Guide: Domain 1: Basic and Applied Sciences andsonia100% (3)
- ACE Personal Trainer Manual, 4 Edition: Communication and Teaching TechniquesDocument51 pagesACE Personal Trainer Manual, 4 Edition: Communication and Teaching TechniquesLouis TrầnNo ratings yet
- 101 Personal Trainer MistakesDocument25 pages101 Personal Trainer Mistakesmochjodhy75% (4)
- NASM GuideDocument206 pagesNASM Guidejajasod0% (1)
- NASM One Repetition Max Conversion (IRM) Chart (PDF, 34k)Document4 pagesNASM One Repetition Max Conversion (IRM) Chart (PDF, 34k)Ni Dien NiNo ratings yet
- PES Study GuideDocument38 pagesPES Study GuideChristos100% (1)
- ACE Personal Trainer QuizesDocument47 pagesACE Personal Trainer Quizesdeepanshi100% (1)
- Fitness Training ProgramDocument6 pagesFitness Training Programkdb.3790No ratings yet
- 5 Strategies For Choosing ExercisesDocument5 pages5 Strategies For Choosing ExercisesFabianinhoLacerdaNo ratings yet
- Strength and Conditioning PDFDocument116 pagesStrength and Conditioning PDFsoniaNo ratings yet
- 101 Personal Trainer Mistakes Reference ListDocument7 pages101 Personal Trainer Mistakes Reference ListJelena MilicevicNo ratings yet
- Personal Training Contract Agreement PDFDocument1 pagePersonal Training Contract Agreement PDFpraveenNo ratings yet
- 24 The-Performance-Digest-Issue-24-October-18Document39 pages24 The-Performance-Digest-Issue-24-October-18Soylo Amado RubioNo ratings yet
- Firstbeat Understanding Athlete Stress and Recovery 241018Document18 pagesFirstbeat Understanding Athlete Stress and Recovery 241018sashiNo ratings yet
- 47 Random Personal Trainer TipsDocument6 pages47 Random Personal Trainer TipsJa VerrinderNo ratings yet
- Transformation Specialist Chapter PreviewDocument17 pagesTransformation Specialist Chapter Previewsayee100% (1)
- Afaa Candidate Handbook 9 2018Document36 pagesAfaa Candidate Handbook 9 2018tesfamichaelNo ratings yet
- Goals and Strategies of Stabilization Training: Phase 1: Corrective Exercise TrainingDocument15 pagesGoals and Strategies of Stabilization Training: Phase 1: Corrective Exercise TrainingGeorge Ost100% (1)
- Core Strength Manual PDFDocument20 pagesCore Strength Manual PDFKenny Omoya Arias100% (1)
- Train Like A Soccer German StarDocument5 pagesTrain Like A Soccer German StarSteven MonárrezNo ratings yet
- Gray Cook Self Limiting ExerciseDocument7 pagesGray Cook Self Limiting ExerciseWaldir Martins NetoNo ratings yet
- Nasm Essentials Workshop Presentation - (pdf-2mb) PDFDocument57 pagesNasm Essentials Workshop Presentation - (pdf-2mb) PDFJean Freitas Lima100% (2)
- Strength Training For KidsDocument8 pagesStrength Training For KidsMike HaughtNo ratings yet
- 16 Lasting Laws Online TrainingDocument19 pages16 Lasting Laws Online TrainingNeuropotts0% (1)
- Personal Training Nutrition Questionnaire Web VersionDocument3 pagesPersonal Training Nutrition Questionnaire Web VersionRachamalla SatyanadhNo ratings yet
- Fitness Business SuccessDocument12 pagesFitness Business Successshinsei40No ratings yet
- Primal Academy For Sports Science Answer Keys Paper 1Document10 pagesPrimal Academy For Sports Science Answer Keys Paper 1praveenNo ratings yet
- WEEK 6 Muscular SystemDocument17 pagesWEEK 6 Muscular SystemMarjorie Lyka LingatNo ratings yet
- Primal Academy For Sports Science Answer Keys Paper 3: Question AssessmentDocument20 pagesPrimal Academy For Sports Science Answer Keys Paper 3: Question AssessmentpraveenNo ratings yet
- Identifying Points Master TungDocument88 pagesIdentifying Points Master Tungangel 1958No ratings yet
- Nasm Opt For Fitness Annual Program Design - (pdf-27k) PDFDocument1 pageNasm Opt For Fitness Annual Program Design - (pdf-27k) PDFRui Cunha100% (1)
- 8 ISSA Professional Nutrition Coach Hand Sized Portion Guide ClientDocument2 pages8 ISSA Professional Nutrition Coach Hand Sized Portion Guide ClientAlexandra Ares100% (1)
- Functional Movement Screen and Y-Balance Test: Validity in Hamstring Injury Risk Prediction?Document74 pagesFunctional Movement Screen and Y-Balance Test: Validity in Hamstring Injury Risk Prediction?NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Energy Systems and Physical ActivityDocument20 pagesEnergy Systems and Physical ActivityLA TarangcoNo ratings yet
- Endurance PeriodisationDocument14 pagesEndurance PeriodisationGlenn JohnstonNo ratings yet
- Your Conditioning Program Does Not Have To Be Sport-Specific - StrongFirstDocument5 pagesYour Conditioning Program Does Not Have To Be Sport-Specific - StrongFirstGrobelNo ratings yet
- NASM ProspectusDocument8 pagesNASM ProspectusKumar VasanthNo ratings yet
- Bench Press ArticleDocument5 pagesBench Press ArticleRehab TrainerNo ratings yet
- Question Paper 3Document26 pagesQuestion Paper 3praveenNo ratings yet
- Coaching Breakthroughs Lesson 1Document50 pagesCoaching Breakthroughs Lesson 1MayNo ratings yet
- Answer Key 4Document22 pagesAnswer Key 4praveenNo ratings yet
- NASM Candidate HandbookDocument44 pagesNASM Candidate HandbookSamuel Morales Jr.No ratings yet
- OPT-corrective Exercise Template PDFDocument1 pageOPT-corrective Exercise Template PDFsoniaNo ratings yet
- Chap 3 PDFDocument35 pagesChap 3 PDFQuốc HuyNo ratings yet
- Weekly Meal Planner: Monday FridayDocument9 pagesWeekly Meal Planner: Monday FridayChris DohertyNo ratings yet
- Six Figure TrainerDocument22 pagesSix Figure Trainerdirtyfrank99No ratings yet
- CareerGuide PT PDFDocument13 pagesCareerGuide PT PDFRakesh ThakurNo ratings yet
- Missouri Physical Fitness Assessment ManualDocument22 pagesMissouri Physical Fitness Assessment ManualYuvrajsinh PadheriyaNo ratings yet
- Personal Training For The 21st Century - ACEDocument30 pagesPersonal Training For The 21st Century - ACENikolovskiNikolaKoleNo ratings yet
- MENTOR SESSION 1 MARY Format Oet For NursingDocument7 pagesMENTOR SESSION 1 MARY Format Oet For NursingAnjana VargheseNo ratings yet
- NCSF Personal Trainer Exam Candidate HandbookDocument28 pagesNCSF Personal Trainer Exam Candidate HandbookThe Fitness CoachNo ratings yet
- NASMDocument12 pagesNASMSai VenkatNo ratings yet
- Start Here: How to Have Success with ANY Diet and Fitness ProgramFrom EverandStart Here: How to Have Success with ANY Diet and Fitness ProgramNo ratings yet
- Personal Trainer Magazine PDFDocument54 pagesPersonal Trainer Magazine PDFdixieakerszNo ratings yet
- 2 Cases, Client Profile-Steve RogersDocument11 pages2 Cases, Client Profile-Steve Rogerstestbank100% (4)
- NSCA Tools and Resources PDFDocument3 pagesNSCA Tools and Resources PDFkunal mishraNo ratings yet
- 1 - Sis40215 CPT Case Studies 3Document61 pages1 - Sis40215 CPT Case Studies 3Aarti J0% (2)
- Become A NESTA Certified Personal TrainerDocument1 pageBecome A NESTA Certified Personal Trainernesta certifiedNo ratings yet
- ACE Personal Trainer Sample QuestionsDocument2 pagesACE Personal Trainer Sample QuestionsFitness Tutor for the ACE & NSCA Exams0% (1)
- MC SPF Q1102 Fitness-TrainerDocument13 pagesMC SPF Q1102 Fitness-TrainerAnilNo ratings yet
- Evidence-Based Strength & HypertrophyDocument6 pagesEvidence-Based Strength & HypertrophyAnže BenkoNo ratings yet
- 2c Sport-Specific Nutrition Main Document May 2021Document9 pages2c Sport-Specific Nutrition Main Document May 2021Martin WechselbergerNo ratings yet
- BM Flyers Online PDFDocument2 pagesBM Flyers Online PDFConnor RiceNo ratings yet
- Basketball (Pre Assessment)Document2 pagesBasketball (Pre Assessment)Raymon Villapando BardinasNo ratings yet
- Largeandsmallmuscles PDFDocument4 pagesLargeandsmallmuscles PDFsoniaNo ratings yet
- JaneJohnson Tipsandtricksforthelumbarspine1Document5 pagesJaneJohnson Tipsandtricksforthelumbarspine1soniaNo ratings yet
- SOCIology of Health and IllnessDocument27 pagesSOCIology of Health and IllnessEmmanuelNo ratings yet
- Avascular Necrosis of The HipDocument22 pagesAvascular Necrosis of The Hipbjpalmer100% (2)
- Madcow and Mad "Human" DiseaseDocument15 pagesMadcow and Mad "Human" DiseaseMaruli PandjaitanNo ratings yet
- Camp of Swarna Bindu PrashanaDocument10 pagesCamp of Swarna Bindu PrashanaAditya BansalNo ratings yet
- COVID BIology, by Godwin Paul v. EfondoDocument2 pagesCOVID BIology, by Godwin Paul v. EfondoGodwin Paul EfondoNo ratings yet
- Safe Food HandlerDocument24 pagesSafe Food HandlermaddieecomeauNo ratings yet
- Husi:: Notifikasaun Moras Ka Moras Ne'ebe Akontese Ho SurtuDocument18 pagesHusi:: Notifikasaun Moras Ka Moras Ne'ebe Akontese Ho SurtuTīťťhūś Cårvåłhø100% (1)
- Nitin Chauhan MedicalDocument3 pagesNitin Chauhan Medicalprashantp7819980No ratings yet
- Detailed Lesson Plan in Mapeh 10 Health: Prepared By: Michele G. Bayaca Practice TeacherDocument9 pagesDetailed Lesson Plan in Mapeh 10 Health: Prepared By: Michele G. Bayaca Practice TeacherChristine Sara Dada0% (1)
- Risk FactorsDocument6 pagesRisk Factorsnataarajan praveenNo ratings yet
- SE - Brufen 200400600 - PILDocument9 pagesSE - Brufen 200400600 - PILSrechko MilichNo ratings yet
- 3-Sumran Ali, MPA (Hefei-China) PDFDocument16 pages3-Sumran Ali, MPA (Hefei-China) PDFWahyu WibowoNo ratings yet
- VaccinesDocument11 pagesVaccinesZora DNo ratings yet
- Bm33 11 Co Infectionsandco Morbidities Report enDocument15 pagesBm33 11 Co Infectionsandco Morbidities Report enUtary Rezki SakinahNo ratings yet
- Ireland: Vaccination Certificate Deimhniú VacsaínitheDocument1 pageIreland: Vaccination Certificate Deimhniú Vacsaínithetamil ponumaniNo ratings yet
- Infection Prevention and Control Workbook Final Version Sept 2019 PDFDocument113 pagesInfection Prevention and Control Workbook Final Version Sept 2019 PDFRahmiati LaoNo ratings yet
- Pit AnjaDocument6 pagesPit AnjaAbdullah Misini100% (1)
- Ayurveda 11 2 1Document3 pagesAyurveda 11 2 1someshNo ratings yet
- LeukocytosisDocument2 pagesLeukocytosisNeoMedicaNo ratings yet
- Weekly Output 1ST English For Academics and Professional Purposes 2021-2022 Date: NAME: Von Drahcir R. AmoresDocument4 pagesWeekly Output 1ST English For Academics and Professional Purposes 2021-2022 Date: NAME: Von Drahcir R. AmoresVon AmoresNo ratings yet
- Skrining Tuberkulosis (TB) Paru: Field Epidemiology and Training Program (FETP) Universitas Gadjah MadaDocument6 pagesSkrining Tuberkulosis (TB) Paru: Field Epidemiology and Training Program (FETP) Universitas Gadjah MadaYulia FondaNo ratings yet
- Microbiology Syllabus and Recommended Books For MBBSDocument3 pagesMicrobiology Syllabus and Recommended Books For MBBSRehaab MohiuddinNo ratings yet
- Pendingan Aspek Medis - Maret 2020Document33 pagesPendingan Aspek Medis - Maret 2020AdraNo ratings yet
- Is Metabolic Syndrome Associated With The Risk of Recurrent Stroke: A Meta-Analysis of Cohort StudiesDocument6 pagesIs Metabolic Syndrome Associated With The Risk of Recurrent Stroke: A Meta-Analysis of Cohort Studieszefri suhendarNo ratings yet
- Day 13 REDCOPDocument46 pagesDay 13 REDCOPPrabin ChaudharyNo ratings yet
- Diverticular Disease Treatment in Pune - Kaizen Gastro CareDocument4 pagesDiverticular Disease Treatment in Pune - Kaizen Gastro CareKaizen Gastro CareNo ratings yet
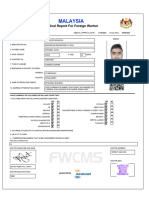
- Malaysia: Medical Report For Foreign WorkerDocument1 pageMalaysia: Medical Report For Foreign Workerjubayer9250bossNo ratings yet