You might also like
- Framework, Scope and TrendsDocument25 pagesFramework, Scope and TrendsKinjal Vasava100% (5)
- Futuristic NursingDocument14 pagesFuturistic NursingHarpreet Dhatt50% (4)
- Nursing Practice Framework Scope and TrendsDocument9 pagesNursing Practice Framework Scope and TrendsAru Verma100% (3)
- Independent Nurse Midwifery PractitionerDocument2 pagesIndependent Nurse Midwifery PractitionerShubhi Vaivhare100% (2)
- Seminar On Standing Orders and Protocols and Use of Selected Life SavingDocument18 pagesSeminar On Standing Orders and Protocols and Use of Selected Life SavingmalathiNo ratings yet
- Dvance Ursing Ractice: Seminar ON Professional Organizations, Unions and Self DefenceDocument19 pagesDvance Ursing Ractice: Seminar ON Professional Organizations, Unions and Self DefenceValarmathiNo ratings yet
- Surgical MenopauseDocument12 pagesSurgical MenopausePabhat Kumar100% (1)
- Vision, Mission and Objectives in Nursing ManagementDocument56 pagesVision, Mission and Objectives in Nursing ManagementPriyaNo ratings yet
- Independent Midwifery PracticeDocument18 pagesIndependent Midwifery Practiceneeta rajesh bhide100% (3)
- Theories, Models in ObgDocument83 pagesTheories, Models in ObgSyama Aneesh100% (1)
- Patterns of Nursing Care Delivery in IndiaDocument22 pagesPatterns of Nursing Care Delivery in IndiaJeenaJohn100% (2)
- Biologic and Psychosocial Dynamics in Disease CausationDocument35 pagesBiologic and Psychosocial Dynamics in Disease Causationlivelinami100% (4)
- Risk Approach of Obstetrical CareDocument5 pagesRisk Approach of Obstetrical CareKinjal Vasava75% (4)
- Independent Practice IssuesDocument7 pagesIndependent Practice IssuesPradip Chougale100% (5)
- Obstetrics and Gynaecology TheoriesDocument25 pagesObstetrics and Gynaecology TheoriesSANANo ratings yet
- Annotated Bibliography of Obstetrics & Gynaecology ResourcesDocument4 pagesAnnotated Bibliography of Obstetrics & Gynaecology ResourcesKaku ManishaNo ratings yet
- Principles and Techniques of CounsellingDocument22 pagesPrinciples and Techniques of Counsellingchetankumarbhumireddy100% (1)
- Preventive Obstetrics: Presented By-Itismita Biswal M, Sc. Nursing (1) Yr Obstetrics & Gynaecological NursingDocument20 pagesPreventive Obstetrics: Presented By-Itismita Biswal M, Sc. Nursing (1) Yr Obstetrics & Gynaecological NursingPabhat Kumar89% (9)
- On Epidemological Aspects of Maternal and Child HealthDocument30 pagesOn Epidemological Aspects of Maternal and Child HealthBisma Maqbool67% (3)
- SNCDocument9 pagesSNCValarmathi100% (1)
- Preventive Obstetrics SeminarDocument25 pagesPreventive Obstetrics SeminarAnju MargaretNo ratings yet
- EDUCATIONAL PREPARATIO ShitalDocument28 pagesEDUCATIONAL PREPARATIO ShitalKinjal Vasava100% (2)
- Seminar On National Health and Family Welfare Programmes Related To Maternal and ChildhealthDocument21 pagesSeminar On National Health and Family Welfare Programmes Related To Maternal and ChildhealthKondapavuluru Jyothi81% (36)
- 5174health Promotion Models in Midwifery - Raheega 3Document54 pages5174health Promotion Models in Midwifery - Raheega 3Jyoti Prem Uttam100% (3)
- Nursing Autonomy and AccountabilityDocument6 pagesNursing Autonomy and AccountabilityRabu75% (4)
- Role of Professional Association and UnionsDocument11 pagesRole of Professional Association and UnionsDivya Thomas80% (5)
- Master of Philosophy Programme in NursingDocument17 pagesMaster of Philosophy Programme in NursingSanjay Kumar SanjuNo ratings yet
- Evaluation of Educational Programs in Nursing Course and Program V1Document13 pagesEvaluation of Educational Programs in Nursing Course and Program V1Stephina ImmaculateNo ratings yet
- Abortion Legislation inDocument57 pagesAbortion Legislation inValarmathi Thangadurai100% (1)
- Critical Analysis of M.sc. Program of Teacher Education in IndiaDocument13 pagesCritical Analysis of M.sc. Program of Teacher Education in Indiakiran mahal76% (17)
- Public Relations Nursing EducationDocument77 pagesPublic Relations Nursing EducationKalla Daniel SharonNo ratings yet
- Maintaining Good Faculty-Staff RelationshipsDocument2 pagesMaintaining Good Faculty-Staff RelationshipsShaells Joshi90% (10)
- Role of Professional Associations and Unions GauriDocument18 pagesRole of Professional Associations and Unions GauriBisakha DeyNo ratings yet
- Independent Nurse PractitionerDocument14 pagesIndependent Nurse PractitionerKarishma Shroff100% (1)
- MiesDocument40 pagesMiessanthiyasandyNo ratings yet
- Recent Advancement in Contraceptive TechnologyDocument3 pagesRecent Advancement in Contraceptive Technologyjeelani saima83% (6)
- Theories Applied To MidwiferyDocument25 pagesTheories Applied To Midwiferybhawna82% (22)
- Standing Orders, Life Saving Drugs for Obstetric EmergenciesDocument16 pagesStanding Orders, Life Saving Drugs for Obstetric Emergenciesvarshasharma0589% (19)
- Coordination and Organization of Guidance and CounselingDocument82 pagesCoordination and Organization of Guidance and CounselingAiswarya R P Ammu80% (5)
- Epidemiological Aspects of Maternal and Child Health and Its Issues Word ContentDocument40 pagesEpidemiological Aspects of Maternal and Child Health and Its Issues Word ContentNimi Simon100% (2)
- Contemprory Issues in ObstetricsDocument6 pagesContemprory Issues in ObstetricsDelphy Varghese100% (1)
- Epidermological Aspects of Meternal and Child Health Unit 1Document24 pagesEpidermological Aspects of Meternal and Child Health Unit 1Pruthvi100% (4)
- Collaboration Issues and Models - Within and Outside Nursing)Document14 pagesCollaboration Issues and Models - Within and Outside Nursing)madhurima kundu44% (9)
- Independent nurse midwifery practitioner issuesDocument8 pagesIndependent nurse midwifery practitioner issuesKrishnaveni Murugesh100% (3)
- First Year PBBSC Master Rotation Plan by DelphyDocument3 pagesFirst Year PBBSC Master Rotation Plan by DelphyDelphy VargheseNo ratings yet
- Practice Standards For Obstetric and Gynaecological UnitDocument27 pagesPractice Standards For Obstetric and Gynaecological UnitRDi J100% (1)
- Epidemiological Aspects of Maternal and Child HealthDocument30 pagesEpidemiological Aspects of Maternal and Child HealthNitin Sharma100% (1)
- Preparation of Professional Teacher Organizing Professional Aspects of Teacher Preparation ProgramsDocument27 pagesPreparation of Professional Teacher Organizing Professional Aspects of Teacher Preparation ProgramsGaoudam Natarajan50% (4)
- Development and Maintenance of Standards and Accreditation ofDocument38 pagesDevelopment and Maintenance of Standards and Accreditation ofsrimalathi100% (1)
- History of Development of Nursing Profession J CharacteristicsDocument28 pagesHistory of Development of Nursing Profession J CharacteristicsSushma SwathiNo ratings yet
- Nursing Seminar on Health Problems and Data CollectionDocument11 pagesNursing Seminar on Health Problems and Data CollectionLekshmi ManuNo ratings yet
- Concept of Faculty Supervisor (Dual) Position: SupervisionDocument6 pagesConcept of Faculty Supervisor (Dual) Position: SupervisionAru Verma100% (2)
- Educational Aims and Objectives-2Document22 pagesEducational Aims and Objectives-2Shruthi Pingula100% (2)
- Educational Aims and ObjectivesDocument49 pagesEducational Aims and Objectivessona100% (2)
- Prespective of NSG Edu Global N NationalDocument10 pagesPrespective of NSG Edu Global N NationalAru VermaNo ratings yet
- Independent Nurse Practice ANPDocument14 pagesIndependent Nurse Practice ANPSamjhana NeupaneNo ratings yet
- Independent Nurse PractitionerDocument23 pagesIndependent Nurse PractitionerNarjina Begam100% (2)
- Independent Nurse Practice ANPDocument12 pagesIndependent Nurse Practice ANPSavita HanamsagarNo ratings yet
- Nurse Practitioner. (Final)Document14 pagesNurse Practitioner. (Final)SamNo ratings yet
- Independent Nurse Practice ANPDocument12 pagesIndependent Nurse Practice ANPSamjhana Neupane50% (2)
- OSCE & OSPE Final PresentationDocument49 pagesOSCE & OSPE Final PresentationKrini TandelNo ratings yet
- Clinical Teaching ProgrammeDocument11 pagesClinical Teaching ProgrammeKrini TandelNo ratings yet
- Clinical Teaching ProgrammeDocument11 pagesClinical Teaching ProgrammeKrini TandelNo ratings yet
- Factors Influencing Health: Heredity, Environment, Behavior and Access To CareDocument11 pagesFactors Influencing Health: Heredity, Environment, Behavior and Access To Carejitesh royNo ratings yet
- Identification of High Risk PregnanciesDocument15 pagesIdentification of High Risk PregnanciesVidya Ganesh100% (12)
- Developing Nursing Standard Protocals in Labour RoomDocument32 pagesDeveloping Nursing Standard Protocals in Labour RoomKrini TandelNo ratings yet
- Obg AssingmentDocument10 pagesObg AssingmentKrini TandelNo ratings yet
- Need of New Born and Parenting ProcessDocument13 pagesNeed of New Born and Parenting ProcessKrini Tandel100% (3)
- Final Unit Test AssignmentDocument9 pagesFinal Unit Test AssignmentKrini TandelNo ratings yet
- INTERNAL ASSESSMENT AssingnmentDocument5 pagesINTERNAL ASSESSMENT AssingnmentKrini Tandel100% (1)
- Heamodialysis LPDocument32 pagesHeamodialysis LPKrini TandelNo ratings yet
- Demonstration of Comfort and Use of Comfort DevicesDocument9 pagesDemonstration of Comfort and Use of Comfort DevicesKrini Tandel100% (1)
- Cirrhosis of Liver New Lesson PlaneDocument17 pagesCirrhosis of Liver New Lesson PlaneKrini Tandel100% (6)
- Seminar On Standing Orders and Labour ProtocalsDocument18 pagesSeminar On Standing Orders and Labour ProtocalsKrini TandelNo ratings yet
- Pemenant Family PlanningDocument6 pagesPemenant Family PlanningKrini TandelNo ratings yet
- Preventive ObstetricDocument12 pagesPreventive ObstetricRicha KohliNo ratings yet
- Health Pramotion IssueDocument12 pagesHealth Pramotion IssueKrini TandelNo ratings yet
- Final Unit Test AssignmentDocument9 pagesFinal Unit Test AssignmentKrini TandelNo ratings yet
- Fluid RequiermentDocument14 pagesFluid RequiermentKrini TandelNo ratings yet
- New Born CareDocument23 pagesNew Born CareKrini TandelNo ratings yet
- Fluid RequiermentDocument14 pagesFluid RequiermentKrini TandelNo ratings yet
- Need of New Born and Parenting ProcessDocument13 pagesNeed of New Born and Parenting ProcessKrini TandelNo ratings yet
- Common-Procedures-2014 NeonatalDocument34 pagesCommon-Procedures-2014 NeonatalKrini TandelNo ratings yet
- Evidence Based PracticeDocument14 pagesEvidence Based PracticeKrini Tandel100% (2)
- Evidence Based PracticeDocument14 pagesEvidence Based PracticeKrini Tandel100% (2)
- Genital Tract Infection 2Document22 pagesGenital Tract Infection 2Krini TandelNo ratings yet
- Cirrhosis of LiverDocument22 pagesCirrhosis of LiverKrini Tandel50% (2)
- Advanced Neonatal ResuscitationDocument14 pagesAdvanced Neonatal ResuscitationKrini TandelNo ratings yet
- Neurological Assessment AssignmentDocument13 pagesNeurological Assessment AssignmentKrini TandelNo ratings yet
- Division Memorandum No. 100, S. 2017Document6 pagesDivision Memorandum No. 100, S. 2017Dee HeiNo ratings yet
- Sample 2Document30 pagesSample 2marianaNo ratings yet
- The Risk Based AuditDocument6 pagesThe Risk Based AuditHana AlmiraNo ratings yet
- BSBLDR523 - Assessment Task 2Document39 pagesBSBLDR523 - Assessment Task 2dsharlie94No ratings yet
- Education and Out of The Box Thinking - Linearization of Graham's Scan Algorithm Complexity As Fruit of Education PolicyDocument9 pagesEducation and Out of The Box Thinking - Linearization of Graham's Scan Algorithm Complexity As Fruit of Education PolicyUbiquitous Computing and Communication JournalNo ratings yet
- Nguyen Thanh Huong. Safe Vegetable. ISBMBUS1.2010Document68 pagesNguyen Thanh Huong. Safe Vegetable. ISBMBUS1.2010Ku HieuNo ratings yet
- Initial Professional Development - Professional Skills (Revised)Document13 pagesInitial Professional Development - Professional Skills (Revised)Zoraida RamirezNo ratings yet
- Limitless LightDocument3 pagesLimitless Lightidlehans100% (1)
- 2022 John A. Perez Resume CVDocument3 pages2022 John A. Perez Resume CVCalifornia Stem Cell ReportNo ratings yet
- Values Education Website by Nonette MarteDocument12 pagesValues Education Website by Nonette MarteJoviner Yabres LactamNo ratings yet
- Work ImmersionDocument26 pagesWork ImmersionMarc John Lonaery EstilNo ratings yet
- Final Project - BaluDocument94 pagesFinal Project - BalubalunriitNo ratings yet
- Task Sheet 1.1-5 RevisedDocument3 pagesTask Sheet 1.1-5 RevisedEL FuentesNo ratings yet
- Field Experience Assignment #2Document2 pagesField Experience Assignment #2Natali OrtizNo ratings yet
- Makerere 70th Graduation Lists Day 3Document28 pagesMakerere 70th Graduation Lists Day 3The Independent MagazineNo ratings yet
- The Role of Vocational and Technical Education - I. OlaitariDocument22 pagesThe Role of Vocational and Technical Education - I. OlaitarioedhieNo ratings yet
- Contoh Soalan Public PerceptionDocument27 pagesContoh Soalan Public Perception12035safyaabdulmalikNo ratings yet
- Karina Castillo: I Am A 30 Year Old Woman Looking To Further Expand My Career As A Session Singer in The Music IndustryDocument7 pagesKarina Castillo: I Am A 30 Year Old Woman Looking To Further Expand My Career As A Session Singer in The Music IndustryKarina PorterNo ratings yet
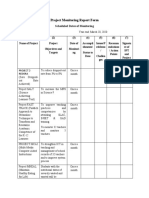
- Project Monitoring Report FormDocument3 pagesProject Monitoring Report FormAireen SiagaNo ratings yet
- Types and Conditions of Social Adaptation ExplainedDocument8 pagesTypes and Conditions of Social Adaptation ExplainedAlbina ScutaruNo ratings yet
- Tinyvers AssignmentDocument3 pagesTinyvers AssignmentRachana Reddy SunkiNo ratings yet
- Ensayo Sobre Las Etapas Básicas Del Proceso de Una Empresa y Las Personas en Un Equipo de Trabajo Ga5-240202501-Aa1-Ev02Document7 pagesEnsayo Sobre Las Etapas Básicas Del Proceso de Una Empresa y Las Personas en Un Equipo de Trabajo Ga5-240202501-Aa1-Ev02Jonathan OrtizNo ratings yet
- Case Study Grid NUR 403 Theories and Models of Nursing PracticeDocument3 pagesCase Study Grid NUR 403 Theories and Models of Nursing Practicenurse911kimNo ratings yet
- QA/QC Engineer-Inspector ResumeDocument2 pagesQA/QC Engineer-Inspector Resumejulius j. madularaNo ratings yet
- Thesis Preschool EducationDocument6 pagesThesis Preschool Educationfc5wsq30100% (1)
- Manisha SinghDocument2 pagesManisha SinghkamleshyadavmoneyNo ratings yet
- Professional Education Child & Adolescent Development 1Document4 pagesProfessional Education Child & Adolescent Development 1Hanna Grace Honrade100% (13)
- Improving Students' Reading Comprehension through Action ResearchDocument91 pagesImproving Students' Reading Comprehension through Action ResearchClaire CabactulanNo ratings yet
- Firm Growth TheoryDocument3 pagesFirm Growth TheoryChakraKhadka100% (2)
- UNMAC - Mine ActionDocument284 pagesUNMAC - Mine ActionFrancesco100% (1)