You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- NCLEX RNdemoDocument14 pagesNCLEX RNdemoricastmaryNo ratings yet
- Sec2chapter12 Aligninginformationsystemusingcsfmethod 130802110141 Phpapp02Document8 pagesSec2chapter12 Aligninginformationsystemusingcsfmethod 130802110141 Phpapp02padmaNo ratings yet
- Watershortage 170116135910Document6 pagesWatershortage 170116135910padmaNo ratings yet
- HAAD ReviewerDocument35 pagesHAAD ReviewerSydRey92% (24)
- Criticalpathmethodcpm 160629040025Document20 pagesCriticalpathmethodcpm 160629040025padmaNo ratings yet
- Kinds and Classifications of ResearchDocument11 pagesKinds and Classifications of Researcherwin rectoNo ratings yet
- 3000wordessaymakeupandbeauty 140522053111 Phpapp01Document5 pages3000wordessaymakeupandbeauty 140522053111 Phpapp01padmaNo ratings yet
- 4573Document2 pages4573padmaNo ratings yet
- Documentationtypes 100406074633 Phpapp02Document13 pagesDocumentationtypes 100406074633 Phpapp02padmaNo ratings yet
- Thesisresearchpaperexamplestopics 100924064922 Phpapp01 PDFDocument1 pageThesisresearchpaperexamplestopics 100924064922 Phpapp01 PDFpadmaNo ratings yet
- Hydatidcystofliver 091114233153 Phpapp02Document20 pagesHydatidcystofliver 091114233153 Phpapp02padmaNo ratings yet
- Creativeessaywritingtopics 100924064859 Phpapp01 PDFDocument1 pageCreativeessaywritingtopics 100924064859 Phpapp01 PDFpadmaNo ratings yet
- Argumentativeessayoutline 170116135030 PDFDocument1 pageArgumentativeessayoutline 170116135030 PDFpadmaNo ratings yet
- MSC Nursing - 2009 - 1 - Clinical Specialty I - Mental Health (Psychiatric) NursingDocument1 pageMSC Nursing - 2009 - 1 - Clinical Specialty I - Mental Health (Psychiatric) NursingpadmaNo ratings yet
- Biochemistryhighyield 120125063515 Phpapp02 PDFDocument18 pagesBiochemistryhighyield 120125063515 Phpapp02 PDFpadmaNo ratings yet
- Reaserchpaper 100107150523 Phpapp01Document5 pagesReaserchpaper 100107150523 Phpapp01padmaNo ratings yet
- Neuroanatomy 111129205351 Phpapp02Document5 pagesNeuroanatomy 111129205351 Phpapp02padmaNo ratings yet
- Tipstoremember 110410100836 Phpapp02Document13 pagesTipstoremember 110410100836 Phpapp02padmaNo ratings yet
- Hematologymnemonics 151002194222 Lva1 App6891Document8 pagesHematologymnemonics 151002194222 Lva1 App6891padmaNo ratings yet
- Inhdrug 150611074056 Lva1 App6891Document17 pagesInhdrug 150611074056 Lva1 App6891padmaNo ratings yet
- Hematology Mnemonics: Macrocytic Anemia CausesDocument8 pagesHematology Mnemonics: Macrocytic Anemia CausespadmaNo ratings yet
- Gisystemmnemonics 151002183330 Lva1 App6892Document7 pagesGisystemmnemonics 151002183330 Lva1 App6892padmaNo ratings yet
- Cardiologymnemonics 131127141317 Phpapp02Document4 pagesCardiologymnemonics 131127141317 Phpapp02padmaNo ratings yet
- Synapses 151229164516Document14 pagesSynapses 151229164516padmaNo ratings yet
- Propioceptiveneuromuscularfacilitation 151229171301Document16 pagesPropioceptiveneuromuscularfacilitation 151229171301padmaNo ratings yet
- Basicstructureofneuron 151204003458 Lva1 App6892Document2 pagesBasicstructureofneuron 151204003458 Lva1 App6892padmaNo ratings yet
- Endocrinesystemmnemonics 151002183222 Lva1 App6892Document3 pagesEndocrinesystemmnemonics 151002183222 Lva1 App6892padmaNo ratings yet
- Sodiumpotassiumpump 161120143926Document4 pagesSodiumpotassiumpump 161120143926padmaNo ratings yet
- Typesofneuron 120714094052 Phpapp01Document11 pagesTypesofneuron 120714094052 Phpapp01padmaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cell - Unit of Life Notes+ EXEDocument95 pagesCell - Unit of Life Notes+ EXEheena lakhwaniNo ratings yet
- Elaj Al SalikinDocument80 pagesElaj Al SalikinMohammed Abdul Hafeez, B.Com., Hyderabad, India100% (1)
- CHM 131 Case StudyDocument13 pagesCHM 131 Case StudyNabila IgorNo ratings yet
- Tarell Swain - Journal 1 - My Purpose For Pursuing CollegeDocument3 pagesTarell Swain - Journal 1 - My Purpose For Pursuing CollegeAlexis BodieNo ratings yet
- EUCAST V - 9.0 - Breakpoint - Tables PDFDocument100 pagesEUCAST V - 9.0 - Breakpoint - Tables PDFRicardo Ariel GianeciniNo ratings yet
- Chemical Fact SheetDocument2 pagesChemical Fact SheetAnonymous dp5b3X1NANo ratings yet
- Subconjunctival HaemorrhageDocument7 pagesSubconjunctival HaemorrhageTry Ahmad MirzaNo ratings yet
- Recat Medical BoardDocument5 pagesRecat Medical BoardNavara Naveen kumarNo ratings yet
- Urology Basics What You Should Know Fact SheetDocument2 pagesUrology Basics What You Should Know Fact SheetWaseem MoukhtarNo ratings yet
- LILLE FRANCE Trip Report-MajaliwaDocument4 pagesLILLE FRANCE Trip Report-MajaliwaMajaliwa TungarazaNo ratings yet
- DRUG AbuseDocument77 pagesDRUG AbuseJmart84No ratings yet
- THE ANTIFUNGAL PROPERTY OF RADISH EXTRACT (RaphanusDocument35 pagesTHE ANTIFUNGAL PROPERTY OF RADISH EXTRACT (RaphanusJaroq Aljon HipolitoNo ratings yet
- 2018-09-01 Men's Fitness UK PDFDocument116 pages2018-09-01 Men's Fitness UK PDFsalik salmanNo ratings yet
- Lesson Plan Q4 Week1 Support Agronomic Crop WorkDocument6 pagesLesson Plan Q4 Week1 Support Agronomic Crop WorkTeodi Alden TegioNo ratings yet
- CoronarografieDocument72 pagesCoronarografieLaurentiu AndreiNo ratings yet
- ASPEN Consensus Recommendations For RefeedingDocument18 pagesASPEN Consensus Recommendations For RefeedingCLAUDIA PATRICIA AGUADO QUINTERONo ratings yet
- Anxiety Disorders: Powerpoint Lecture Notes PresentationDocument43 pagesAnxiety Disorders: Powerpoint Lecture Notes PresentationErsido SamuelNo ratings yet
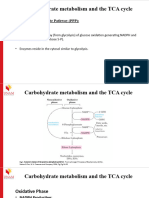
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelNo ratings yet
- Graduate School Application Essay ExamplesDocument8 pagesGraduate School Application Essay Examplesafabeaida100% (2)
- Uterin InversionDocument8 pagesUterin InversionZahra AlSaif100% (1)
- ACEM PostersDocument2 pagesACEM PostersDr.KHAJA SHAFIUDDINNo ratings yet
- Typhoid Fever Epidemics in the Philippines: Contaminated Wells as Risk FactorDocument5 pagesTyphoid Fever Epidemics in the Philippines: Contaminated Wells as Risk Factorjessica_nava_8No ratings yet
- Group 8Document14 pagesGroup 8HrishavNo ratings yet
- Research Article: Ihsan Otriami, Devin Mahendika, Dio JainataDocument19 pagesResearch Article: Ihsan Otriami, Devin Mahendika, Dio JainataRollyRiksantoNo ratings yet
- Patient Counselling - CPDocument8 pagesPatient Counselling - CPmrcopy xeroxNo ratings yet
- Cardiac Self-Efficacy and Quality of Life in Patients With Coronary Heart Disease: A Cross-Sectional Study From PalestineDocument13 pagesCardiac Self-Efficacy and Quality of Life in Patients With Coronary Heart Disease: A Cross-Sectional Study From Palestineشبلي غرايبهNo ratings yet
- Avhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Document6 pagesAvhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Phuong ThaoNo ratings yet
- Anatomy and Physiology of Adrenal GlandDocument26 pagesAnatomy and Physiology of Adrenal GlandYAMINIPRIYANNo ratings yet
- The Importance of NutritionDocument16 pagesThe Importance of NutritionRonna DipasupilNo ratings yet
- Α Α Α Α-Amylase-Eps: Biosystems S.ADocument1 pageΑ Α Α Α-Amylase-Eps: Biosystems S.ARisqon Anjahiranda AdiputraNo ratings yet