You might also like
- Admission Requirements, Sy 2015-2016Document1 pageAdmission Requirements, Sy 2015-2016Monica DumalaogNo ratings yet
- 2018 2019 Admission RqmtsDocument1 page2018 2019 Admission RqmtsLucid LynxNo ratings yet
- William H. Quasha Memorial: A. Application For Admission Requirements Freshmen TransfereeDocument1 pageWilliam H. Quasha Memorial: A. Application For Admission Requirements Freshmen TransfereeJuan De FocaNo ratings yet
- Medschool ApplicationsDocument2 pagesMedschool ApplicationsNO ONENo ratings yet
- Uwindsor Meng ApplicationDocument2 pagesUwindsor Meng Applicationyunus_bashar1813No ratings yet
- Application FormsDocument6 pagesApplication FormsseptillionaireNo ratings yet
- EACCR Training Application FormDocument2 pagesEACCR Training Application FormPAGINo ratings yet
- Application For 2022 Fall International Exchange StudentDocument30 pagesApplication For 2022 Fall International Exchange StudentThùy DungNo ratings yet
- Admission Form 2021-22 MBBS & BDSDocument4 pagesAdmission Form 2021-22 MBBS & BDSAhmed AliNo ratings yet
- EduCare Grant Application Form 21 22Document5 pagesEduCare Grant Application Form 21 22Antonyio CurtisNo ratings yet
- GSFS Guide (Fall 2019)Document8 pagesGSFS Guide (Fall 2019)PutriPasaribuNo ratings yet
- Application Form JuniorDocument1 pageApplication Form JuniorPee Dee Hey EstiloNo ratings yet
- Uconn 003 Fact Sheet 011117 Web 1Document2 pagesUconn 003 Fact Sheet 011117 Web 1api-365015922No ratings yet
- Admission Form - PCoHAS - 2022-2023 v5Document3 pagesAdmission Form - PCoHAS - 2022-2023 v5Mussa AthanasNo ratings yet
- Ched Student Financial Assistance Programs (Stufaps) Application FormDocument3 pagesChed Student Financial Assistance Programs (Stufaps) Application Formmary roseNo ratings yet
- Convenios de Colaboracion1 PDFDocument114 pagesConvenios de Colaboracion1 PDFDavid CamposNo ratings yet
- Stanford University Common Data Set 2021 - 2022Document41 pagesStanford University Common Data Set 2021 - 2022SakshamNo ratings yet
- Graduate Legislative Fellowship ApplicationDocument2 pagesGraduate Legislative Fellowship ApplicationNew York SenateNo ratings yet
- MCM 2023Document4 pagesMCM 2023druno255No ratings yet
- Feu Entrance Examination Application FormDocument2 pagesFeu Entrance Examination Application FormJay Anthony50% (6)
- AO1 2021 Application Form For AdmissionDocument2 pagesAO1 2021 Application Form For AdmissionMa Cristina VelascoNo ratings yet
- Advertisement For Guest Faculty (Per Lecture Basis) 9248Document4 pagesAdvertisement For Guest Faculty (Per Lecture Basis) 9248RAHUL MATHURNo ratings yet
- Admission and Scholarship Requirements 2020-2021 - v02Document2 pagesAdmission and Scholarship Requirements 2020-2021 - v02IrishNo ratings yet
- VT International BrochureDocument20 pagesVT International BrochureAnnNo ratings yet
- MGM University BSc programsDocument2 pagesMGM University BSc programsCherry KushwahaNo ratings yet
- General Academic Information Undergraduate Admission Policies/Requirements New FreshmanDocument10 pagesGeneral Academic Information Undergraduate Admission Policies/Requirements New FreshmanKlaus AlmesNo ratings yet
- CSU2021Document4 pagesCSU2021Electrical EngineerNo ratings yet
- Ag EnglishDocument27 pagesAg Englishatifa ashrafNo ratings yet
- Gctcdo Fo.27 Cccapplication FormDocument2 pagesGctcdo Fo.27 Cccapplication FormJohn Carlo AlcantaraNo ratings yet
- Oss-Ched Scholarship FormDocument1 pageOss-Ched Scholarship Formramilsanchez@yahoo.com100% (4)
- Bachelor of Arts Application: New York Film AcademyDocument7 pagesBachelor of Arts Application: New York Film AcademyPedro SantiagoNo ratings yet
- SS Examapplication RPTDocument1 pageSS Examapplication RPTSouvik chatterjeeNo ratings yet
- Scholarship Application FormDocument2 pagesScholarship Application FormJaxel LumaynoNo ratings yet
- CTCC-APPLICATION-FORMDocument7 pagesCTCC-APPLICATION-FORMmzfqyptytdNo ratings yet
- International Student Admission ProcedureDocument2 pagesInternational Student Admission ProcedureSiti SyafiqahNo ratings yet
- AOFF Scholarship Application FormDocument2 pagesAOFF Scholarship Application FormKrisha FernandezNo ratings yet
- MPH Admission Form Session Spring 2020 - 1Document3 pagesMPH Admission Form Session Spring 2020 - 1farooqNo ratings yet
- 2020 Information Brochure B.SC - AgriDocument9 pages2020 Information Brochure B.SC - Agrideva sekarNo ratings yet
- Inbound Exchange Student Nomination Form: Instructions For Exchange Program CoordinatorDocument1 pageInbound Exchange Student Nomination Form: Instructions For Exchange Program CoordinatorMario AndresNo ratings yet
- WelcomeGuide2022 UniversityDocument20 pagesWelcomeGuide2022 UniversitySylph MoonNo ratings yet
- Mcu Form International StudentDocument12 pagesMcu Form International StudentJason WongNo ratings yet
- BPEI Clinical Observership ApplicationDocument4 pagesBPEI Clinical Observership ApplicationDayana SalasNo ratings yet
- Advert Direct Entry 20242025Document3 pagesAdvert Direct Entry 20242025henrykiggundu11No ratings yet
- CPD Application Form for Lusaka Apex Medical UniversityDocument6 pagesCPD Application Form for Lusaka Apex Medical UniversityOrlando CostaNo ratings yet
- BS Pharm D Admission Form AustDocument3 pagesBS Pharm D Admission Form AustYasir MehmoodNo ratings yet
- School Contingency Plan For COVID-19 OutbreakDocument11 pagesSchool Contingency Plan For COVID-19 OutbreakJonathan BlasNo ratings yet
- Annual Report: Ucf Burnett Honors CollegeDocument14 pagesAnnual Report: Ucf Burnett Honors CollegeJonathan GabrielNo ratings yet
- About Strand PDFDocument2 pagesAbout Strand PDFErnesto CaguayNo ratings yet
- Application For Accreditation of CoursesDocument2 pagesApplication For Accreditation of CoursesClint Dwight F. PandoNo ratings yet
- PG Reg WeekendDocument4 pagesPG Reg WeekendAraarsaa Deesisaa GannatiiNo ratings yet
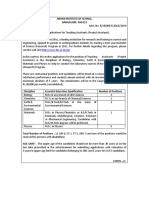
- Indian Institute of Science, BANGALORE-560 012Document4 pagesIndian Institute of Science, BANGALORE-560 012Ashwath KumaranNo ratings yet
- 2"x 2" Picture: Application Form University Admission TestDocument2 pages2"x 2" Picture: Application Form University Admission TestARCH3S PANAGSAGAN JR. BSCE3BNo ratings yet
- Salvar AgrDocument26 pagesSalvar AgrDoos TalissonNo ratings yet
- 2022 Confidential Academic Reference FormDocument2 pages2022 Confidential Academic Reference Formiputama99No ratings yet
- Mobility Program Inbound 2023 2024Document12 pagesMobility Program Inbound 2023 2024장민호No ratings yet
- UCC Graduation ApplicationDocument3 pagesUCC Graduation ApplicationSophia PerezNo ratings yet
- Missing the Mark: Why So Many School Exam Grades are Wrong – and How to Get Results We Can TrustFrom EverandMissing the Mark: Why So Many School Exam Grades are Wrong – and How to Get Results We Can TrustNo ratings yet
- RPHDocument3 pagesRPHErica Jazzanne LopezNo ratings yet
- Module 2Document29 pagesModule 2Erica Jazzanne LopezNo ratings yet
- Interview SheetDocument2 pagesInterview SheetChristian Irvin Harvey DavidNo ratings yet
- Med Reco Letter (Mam Mye - Feu)Document1 pageMed Reco Letter (Mam Mye - Feu)Erica Jazzanne LopezNo ratings yet
- Mod 2 Pharmacognosy PDFDocument11 pagesMod 2 Pharmacognosy PDFJoelly C. ValendezNo ratings yet
- Mod 2 Pharmacognosy PDFDocument11 pagesMod 2 Pharmacognosy PDFJoelly C. ValendezNo ratings yet
- 2015 Usnco Local ExamDocument8 pages2015 Usnco Local ExamLizAndrei Jaja MarquezNo ratings yet
- Pharmacology: General Anaesthetic AgentsDocument65 pagesPharmacology: General Anaesthetic AgentsSharifa DarayanNo ratings yet
- ChemistryDocument7 pagesChemistryPaul Anthony LontokNo ratings yet
- Social Sciences Part 2: Sociology, Enculturation, ProverbsDocument7 pagesSocial Sciences Part 2: Sociology, Enculturation, ProverbsChoy Savilla100% (1)
- ChemistryDocument7 pagesChemistryPaul Anthony LontokNo ratings yet
- Madiha Riasat: ObjectiveDocument3 pagesMadiha Riasat: Objectivecallraza19No ratings yet
- Ch1. Considering Materiality and RiskDocument47 pagesCh1. Considering Materiality and RiskAli AlbaqshiNo ratings yet
- American Political Parties: Republicans vs. DemocratsDocument60 pagesAmerican Political Parties: Republicans vs. DemocratsSchmetterling TraurigNo ratings yet
- Vedanta KesariDocument56 pagesVedanta Kesarigeo_unoNo ratings yet
- Financial Shenanigans 3rd EditionDocument6 pagesFinancial Shenanigans 3rd Editionpwsicher100% (1)
- Tan Vs ZanduetaDocument2 pagesTan Vs ZanduetaPearl Deinne Ponce de LeonNo ratings yet
- Au L 1637113412 Poem Analysis of Matilda by Hilaire Belloc - Ver - 2Document5 pagesAu L 1637113412 Poem Analysis of Matilda by Hilaire Belloc - Ver - 2Manha abdellahNo ratings yet
- NEw IC 38 SummaryDocument80 pagesNEw IC 38 SummaryMadhup tarsolia100% (2)
- PIL For Generic Drugs by DR Sanjay KulshresthaDocument23 pagesPIL For Generic Drugs by DR Sanjay KulshresthaSanjay KulshresthaNo ratings yet
- Leadership in The Remote, Freelance, and Virtual Workforce EraDocument6 pagesLeadership in The Remote, Freelance, and Virtual Workforce EraRenata JapurNo ratings yet
- Chapter Five - Globalization of Irish Step DanceDocument38 pagesChapter Five - Globalization of Irish Step DanceElizabeth Venable0% (1)
- Unit 1 MCQDocument7 pagesUnit 1 MCQHan Nwe OoNo ratings yet
- Big BazarDocument62 pagesBig BazarVenki GajaNo ratings yet
- UGmacro2022 ps1Document2 pagesUGmacro2022 ps1Chunming TangNo ratings yet
- Entering and Developing A Service Network: Sheena Leek and Louise CanningDocument10 pagesEntering and Developing A Service Network: Sheena Leek and Louise CanningTanisha KrunalNo ratings yet
- E-Commerce and Consumer Goods A Strategy For Omnichannel SuccessDocument16 pagesE-Commerce and Consumer Goods A Strategy For Omnichannel SuccessAnthony Le Jr.100% (1)
- UntitledDocument22 pagesUntitledArjun kumar ShresthaNo ratings yet
- Financial Performance and Position HighlightsDocument100 pagesFinancial Performance and Position HighlightsSHAMSUL ARIF ZULFIKAR HUSNINo ratings yet
- CSS - 2 2 2023 CSS - 2Document1 pageCSS - 2 2 2023 CSS - 2Nirmal GeorgeNo ratings yet
- EAD 513 Kirk Summers Cultural Functions in PracticeDocument6 pagesEAD 513 Kirk Summers Cultural Functions in PracticeKirk Summers100% (1)
- IMI ScriptDocument130 pagesIMI ScriptDiego JacobsNo ratings yet
- 05 Cold CallingDocument106 pages05 Cold CallingSpil_vv_IJmuidenNo ratings yet
- The Influence of The English Language On The Russian Youth SlangDocument10 pagesThe Influence of The English Language On The Russian Youth SlangВасилий БоровцовNo ratings yet
- Achieving Balance Through SincerityDocument15 pagesAchieving Balance Through Sinceritychocoholic_soph91No ratings yet
- ACCOUNTS RECEIVABLES 7-8 - Sheet1-2Document3 pagesACCOUNTS RECEIVABLES 7-8 - Sheet1-2Astrid AboitizNo ratings yet
- Giovanna Ferrer - Language III - PW # 8 Use of EnglishDocument2 pagesGiovanna Ferrer - Language III - PW # 8 Use of EnglishGiovanna FerrerNo ratings yet
- Imo Modu Code 2001Document151 pagesImo Modu Code 2001Anonymous dQzWfU3y9100% (2)
- Integration of Islamic Education in Public SchoolsDocument7 pagesIntegration of Islamic Education in Public SchoolstimespergerakanNo ratings yet
- Sara's CAS Proposal FormDocument3 pagesSara's CAS Proposal FormsaraNo ratings yet
- Mumbai to Goa Flight Ticket BookingDocument3 pagesMumbai to Goa Flight Ticket BookingDarshNo ratings yet