You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- VT SgnsDocument3 pagesVT SgnsAndee SalegonNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Appendix A. Matric of ThemesDocument52 pagesAppendix A. Matric of ThemesAndee SalegonNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Medici Di Makati College 1061 Metropolitan Avenue, San Antonio Village, Makati City, Philippines 1200Document18 pagesMedici Di Makati College 1061 Metropolitan Avenue, San Antonio Village, Makati City, Philippines 1200Andee SalegonNo ratings yet
- IGNACIO, Andee - Anatomy of The Bone and Brain Function When in Pain - OrthoDocument2 pagesIGNACIO, Andee - Anatomy of The Bone and Brain Function When in Pain - OrthoAndee SalegonNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Medici Di Makati College: "Cita Astals Recounts Struggles With Mental Disorder" Reaction PaperDocument3 pagesMedici Di Makati College: "Cita Astals Recounts Struggles With Mental Disorder" Reaction PaperAndee SalegonNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Makati College student attendance sheetDocument1 pageMakati College student attendance sheetAndee SalegonNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- IGNACIO, Andee - Anatomy of The Bone and Brain Function When in Pain - OrthoDocument2 pagesIGNACIO, Andee - Anatomy of The Bone and Brain Function When in Pain - OrthoAndee SalegonNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- DRW IntrptnDocument1 pageDRW IntrptnAndee SalegonNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Drugs BadingDocument3 pagesDrugs BadingAndee SalegonNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
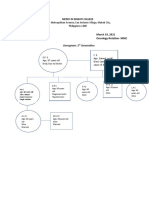
- Genogram of 3 GenerationsDocument1 pageGenogram of 3 GenerationsAndee SalegonNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Medici di Makati College Announces Blended Learning for AY 2020-2021Document2 pagesMedici di Makati College Announces Blended Learning for AY 2020-2021Andee SalegonNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Diabetes Care Plan GuideDocument5 pagesDiabetes Care Plan GuideAndee SalegonNo ratings yet
- Medici Di Makati College: Unparalleled Outbreak of COVID-19 Has Greatly Affected The Education System of Our School LikeDocument2 pagesMedici Di Makati College: Unparalleled Outbreak of COVID-19 Has Greatly Affected The Education System of Our School LikeAndee SalegonNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Community Health Nursing ProcessDocument5 pagesCommunity Health Nursing ProcessAndee SalegonNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Health Teaching Plan 1Document1 pageHealth Teaching Plan 1Andee SalegonNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Bal GenogramDocument1 pageBal GenogramAndee SalegonNo ratings yet
- Nursing Management Planning and OgranizationDocument2 pagesNursing Management Planning and OgranizationAndee SalegonNo ratings yet
- Scale For Ranking-DMDocument5 pagesScale For Ranking-DMAndee SalegonNo ratings yet
- Chapter IiDocument14 pagesChapter IiAndee SalegonNo ratings yet
- Bal FloorplanDocument2 pagesBal FloorplanAndee SalegonNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- FNCP DMDocument1 pageFNCP DMAndee SalegonNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Diabetes Care Plan GuideDocument5 pagesDiabetes Care Plan GuideAndee SalegonNo ratings yet
- 2nd LVL Faulty EatingDocument2 pages2nd LVL Faulty EatingAndee SalegonNo ratings yet
- 1st Level Assessment JAVIER FOR STA CRUZ CASEDocument4 pages1st Level Assessment JAVIER FOR STA CRUZ CASEAndee SalegonNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Market Analysis When Introducing Los Banos To Tourists, They Had To Explain That Los Banos Is From A Spanish WordDocument1 pageMarket Analysis When Introducing Los Banos To Tourists, They Had To Explain That Los Banos Is From A Spanish WordAndee SalegonNo ratings yet
- Anesthesia, Surgery Terms, and Perioperative TrendsDocument2 pagesAnesthesia, Surgery Terms, and Perioperative TrendsAndee SalegonNo ratings yet
- Ampicillin Sulbactam - Drug StudyDocument2 pagesAmpicillin Sulbactam - Drug StudyAndee Salegon100% (5)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Diazepam Drug StudyDocument1 pageDiazepam Drug StudyAndee Salegon100% (3)
- Drug Study VaccinesDocument3 pagesDrug Study VaccinesAndee SalegonNo ratings yet
- Basic HematologyDocument89 pagesBasic Hematologydrafq2000No ratings yet
- Jurnal Reading OsteomyelitisDocument11 pagesJurnal Reading Osteomyelitisfidela_ffNo ratings yet
- Plasma ProteinsDocument28 pagesPlasma ProteinsAyesha AzamNo ratings yet
- ESR3000 - Operator Manual Ver 1 1Document20 pagesESR3000 - Operator Manual Ver 1 1Michael OkekeNo ratings yet
- Lesson 08Document9 pagesLesson 08asyafujisaki100% (2)
- Symptoms: Rheumatoid ArthritisDocument17 pagesSymptoms: Rheumatoid Arthritismehrasa nikandishNo ratings yet
- Interpreting Laboratory Values in Older AdultsDocument11 pagesInterpreting Laboratory Values in Older AdultsmaeNo ratings yet
- Sonu ReportDocument8 pagesSonu ReportVeeraj SinghNo ratings yet
- Growing Pains - UpToDateDocument11 pagesGrowing Pains - UpToDateEver Ivan Restrepo RuizNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- XIJU5502Document3 pagesXIJU5502Praveen ReddyNo ratings yet
- 09 ICSH Review of The Measurement of The ESR PDFDocument8 pages09 ICSH Review of The Measurement of The ESR PDFMuslim Majlis UojNo ratings yet
- Hematology 1 Lab Activities ManualDocument35 pagesHematology 1 Lab Activities ManualAchmad Xenon KongNo ratings yet
- SAPHO Syndrome Current Clinical, Diagnostic and Treatment ApproachesDocument13 pagesSAPHO Syndrome Current Clinical, Diagnostic and Treatment Approachesdarkangelmx1No ratings yet
- XC-A30 ESR Analyzer User's Manual: Caretium Medical Instruments Co., LTDDocument25 pagesXC-A30 ESR Analyzer User's Manual: Caretium Medical Instruments Co., LTDAlexeyNo ratings yet
- Comprehensive Hematology and Biochemistry Report for Mr. Srinivas VDocument28 pagesComprehensive Hematology and Biochemistry Report for Mr. Srinivas VVijaya SheelamNo ratings yet
- Erythrocyte Sedimentation Rate (ESR)Document7 pagesErythrocyte Sedimentation Rate (ESR)Mrym DestinyNo ratings yet
- DynaMed Plus Rheumatoid ArthritisDocument20 pagesDynaMed Plus Rheumatoid ArthritisHeather Marie MathisNo ratings yet
- NURSING PRACTICE I SET A 2007Document17 pagesNURSING PRACTICE I SET A 2007TyronNo ratings yet
- Acute Rheumatic Fever and Rheumatic Heart DiseaseDocument10 pagesAcute Rheumatic Fever and Rheumatic Heart DiseaseBenazir SalsabillahNo ratings yet
- Episodic Focused SOAP NoteDocument7 pagesEpisodic Focused SOAP NoteSam Odoo100% (1)
- Erythrocyte Sedimentation Rate: Westergren MethodDocument20 pagesErythrocyte Sedimentation Rate: Westergren MethodDenise April June CadizNo ratings yet
- Problem Based Learning in Clinical HematologyDocument14 pagesProblem Based Learning in Clinical HematologyThabang ThaboNo ratings yet
- Lab ReportDocument5 pagesLab ReportTAMKEEN MUSTAFANo ratings yet
- Erythrocyte Sedimentation RateDocument57 pagesErythrocyte Sedimentation Ratehirendra patelNo ratings yet
- Erythrocyte Sedimentation Rate: Definition DeterminationDocument3 pagesErythrocyte Sedimentation Rate: Definition DeterminationAnusuya SNo ratings yet
- NLE Compilation 1Document67 pagesNLE Compilation 1blazegomez91% (34)
- Hematological ProceduresDocument14 pagesHematological ProceduresWynlor AbarcaNo ratings yet
- Supplementary AppendixDocument52 pagesSupplementary AppendixZey RamosNo ratings yet
- Pyrexia of Unknown OriginDocument81 pagesPyrexia of Unknown OriginJithin Bhagavati Kalam100% (1)
- OCCUPATIONAL DISEASES Clinical cases 2015 англ 2Document28 pagesOCCUPATIONAL DISEASES Clinical cases 2015 англ 2kjk100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet