Professional Documents
Culture Documents
Kitagawa 2019
Uploaded by
saosaharaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Kitagawa 2019
Uploaded by
saosaharaCopyright:
Available Formats
Research
JAMA Neurology | Original Investigation
Effect of Standard vs Intensive Blood Pressure Control
on the Risk of Recurrent Stroke
A Randomized Clinical Trial and Meta-analysis
Kazuo Kitagawa, MD, PhD; Yasumasa Yamamoto, MD, PhD; Hisatomi Arima, MD, PhD; Toshiki Maeda, MD, PhD; Norio Sunami, MD, PhD;
Takao Kanzawa, MD, PhD; Kazuo Eguchi, MD, PhD; Kenji Kamiyama, MD, PhD; Kazuo Minematsu, MD, PhD; Shinichiro Ueda, MD, PhD;
Hiromi Rakugi, MD, PhD; Yusuke Ohya, MD, PhD; Takahide Kohro, MD, PhD; Koji Yonemoto, MD, PhD; Yasushi Okada, MD, PhD; Jitsuo Higaki, MD, PhD;
Norio Tanahashi, MD, PhD; Genjiro Kimura, MD, PhD; Satoshi Umemura, MD, PhD; Masayasu Matsumoto, MD, PhD; Kazuaki Shimamoto, MD, PhD;
Sadayoshi Ito, MD, PhD; Takao Saruta, MD, PhD; Kazuyuki Shimada, MD, PhD; for the Recurrent Stroke Prevention Clinical Outcome (RESPECT) Study Group
Editorial
IMPORTANCE The Systolic Blood Pressure Intervention Trial (SPRINT) demonstrated that a Supplemental content
systolic blood pressure (BP) target less than 120 mm Hg was superior to less than 140 mm Hg
for preventing vascular events. This trial excluded patients with prior stroke; therefore, the
ideal BP target for secondary stroke prevention remains unknown.
OBJECTIVE To assess whether intensive BP control would achieve fewer recurrent strokes vs
standard BP control.
DESIGN, SETTING, AND PARTICIPANTS Randomized clinical trial (RCT) of standard vs intensive
BP control in an intent-to-treat population of patients who had a history of stroke. Patients
were enrolled between October 20, 2010, and December 7, 2016. For an updated
meta-analysis, PubMed and the Cochrane Central Library database were searched through
September 30, 2018, using the Medical Subject Headings and relevant search terms for
cerebrovascular disease and for intensive BP lowering. This was a multicenter trial that
included 140 hospitals in Japan; 1514 patients who had a history of stroke within the previous
3 years were approached, but 234 refused to give informed consent.
INTERVENTIONS In total, 1280 patients were randomized 1:1 to BP control to less than 140/90
mm Hg (standard treatment) (n = 640) or to less than 120/80 mm Hg (intensive treatment)
(n = 640). However, 17 patients never received intervention; therefore, 1263 patients
assigned to standard treatment (n = 630) or intensive treatment (n = 633) were analyzed.
MAIN OUTCOMES AND MEASURES The primary outcome was stroke recurrence.
RESULTS The trial was stopped early. Among 1263 analyzed patients (mean [SD] age, 67.2
[8.8] years; 69.4% male), 1257 of 1263 (99.5%) completed a mean (SD) of 3.9 (1.5) years of
follow-up. The mean BP at baseline was 145.4/83.6 mm Hg. Throughout the overall follow-up
period, the mean BP was 133.2/77.7 (95% CI, 132.5-133.8/77.1-78.4) mm Hg in the standard
group and 126.7/77.4 (95% CI, 125.9-127.2/73.8-75.0) mm Hg in the intensive group.
Ninety-one first recurrent strokes occurred. Nonsignificant rate reductions were seen for
recurrent stroke in the intensive group compared with the standard group (hazard ratio [HR],
0.73; 95% CI, 0.49-1.11; P = .15). When this finding was pooled in 3 previous relevant RCTs in a
meta-analysis, the risk ratio favored intensive BP control (relative risk, 0.78; 95% CI,
0.64-0.96; P = .02; absolute risk difference, −1.5%; 95% CI, −2.6% to −0.4%; number needed Author Affiliations: Author
affiliations are listed at the end of this
to treat, 67; 95% CI, 39-250). article.
Group Information: The Recurrent
CONCLUSIONS AND RELEVANCE Intensive BP lowering tended to reduce stroke recurrence. Stroke Prevention Clinical Outcome
The updated meta-analysis supports a target BP less than 130/80 mm Hg in secondary stroke (RESPECT) Study Group members
appear at the end of the article.
prevention.
Corresponding Author: Kazuo
Kitagawa, MD, PhD, Department of
TRIAL REGISTRATION ClinicalTrials.gov identifier: NCT01198496 Neurology, Tokyo Women’s Medical
University, 8-1 Kawada-cho,
JAMA Neurol. doi:10.1001/jamaneurol.2019.2167 Shinjuku-ku, Tokyo 162-8666, Japan
Published online July 29, 2019. (kitagawa.kazuo@twmu.ac.jp).
(Reprinted) E1
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Research Original Investigation Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke
I
n 2010, the absolute number of people with a first stroke
in the world was 16.9 million, and the number with stroke- Key Points
related deaths was 5.9 million.1 Therefore, prevention of
Question What is the optimum blood pressure target in
primary and secondary stroke is a priority. Elevated blood pres- secondary stroke prevention?
sure (BP) is the most relevant and prevalent risk factor for
Findings In this randomized clinical trial that included 1263
stroke. Reduction in BP is the most effective intervention to
patients with a history of stroke, intensive blood pressure control
prevent both primary and secondary strokes.2-7 In clinical trials
to less than 120/80 mm Hg tended to reduce stroke recurrence
for primary prevention of cardiovascular events, including compared with standard blood pressure control (<140/90 mm
stroke, the lower the better seems acceptable for stroke pre- Hg). When this finding was pooled with the results of prior trials of
vention in hypertensive patients, with less than 115 mm Hg sug- intensive blood pressure control for secondary stroke prevention
gested as the optimum target level of systolic BP.8 After a stroke, in an updated meta-analysis, intensive blood pressure treatment
lowering BP in the chronic stage reduced the rates of recur- significantly reduced stroke recurrence by 22%.
rent stroke among both hypertensive and nonhypertensive pa- Meaning Intensive blood pressure control to less than 130/80
tients in the Perindopril Protection Against Recurrent Stroke mm Hg is recommended for secondary stroke prevention.
Study (PROGRESS).4 A post hoc analysis of the PROGRESS9 sug-
gested that the optimum target level of systolic BP for the pre-
vention of recurrent stroke is less than 120 mm Hg. In the Sec-
ondary Prevention of Small Subcortical Strokes (SPS3) dence of an acute disturbance of focal neurological func-
randomized trial,10 the BP target was first evaluated in pa- tions, with symptoms lasting more than 24 hours, and
tients with recent stroke. The trial randomly assigned those symptomatic ischemic stroke or intracerebral hemorrhage con-
with lacunar stroke to a systolic BP target of 130 to 149 mm Hg firmed by magnetic resonance imaging or computed tomog-
or less than 130 mm Hg, and the authors showed that the use raphy). Patients in whom stroke onset occurred 1 month or less
of a systolic BP target less than 130 mm Hg is likely to be ben- previously were excluded. Participation required written in-
eficial, especially for the prevention of hemorrhagic stroke. A formed consent, and approval was provided by all local eth-
recent meta-analysis demonstrated that strict and aggressive ics committees for human research. The trial protocol and sta-
control of BP with achieved mean systolic and diastolic BP lev- tistical analysis plan, including clinical sites and numbers
els less than 130 mm Hg and less than 85 mm Hg, respec- of participants, are available in Supplement 1. This study
tively, seemed to be beneficial for secondary prevention.7 In followed the Consolidated Standards of Reporting Trials
primary prevention, the Systolic Blood Pressure Intervention (CONSORT) reporting guidelines.
Trial (SPRINT)11 proved the benefit of aggressive BP control,
demonstrating that targeting a systolic BP less than 120 mm Randomization
Hg resulted in lower rates of major cardiovascular events com- In total, 1280 patients were randomized 1:1 to 2 BP control
pared with less than 140 mm Hg. Although a pooled analysis groups with targets of either less than 140/90 mm Hg (the stan-
of 3 studies12-14 (3632 participants) comparing different sys- dard treatment group [n = 640]) or less than 120/80 mm Hg
tolic BP targets suggested that intensive BP lowering reduced (the intensive treatment group [n = 640]) according to a par-
the rate of recurrent stroke, no clinical trials to date have tested allel design. However, 17 patients never received interven-
the effect of such aggressive BP lowering for secondary stroke tion; therefore, 1263 patients assigned to standard treatment
prevention. In the Recurrent Stroke Prevention Clinical Out- (n = 630) or intensive treatment (n = 633) were analyzed. Ran-
come (RESPECT) Study, we herein tested the hypothesis that domization was conducted through a password-protected, in-
targeting intensive BP lowering of systolic and diastolic blood ternet-based system according to a computer-generated ran-
BP less than 120 mm Hg and less than 80 mm Hg, respec- dom sequence, with patients stratified by age (<70 vs ≥70
tively, reduces the rate of stroke recurrence compared with a years), presence of diabetes, chronic kidney disease,
standard BP-lowering regimen. history of myocardial infarction (MI), and history of atrial
fibrillation.
Intervention
Methods The intensive treatment group received stepwise multidrug
Study Design and Participants therapy with a BP target less than 120/80 mm Hg, and the stan-
The RESPECT Study was a prospective, multicenter, open, dard treatment group received the same stepwise therapy with
masked–end point, randomized clinical trial (RCT) that in- BP targets less than 140/90 mm Hg or less than 130/80 mm Hg
cluded 140 hospitals in Japan between October 20, 2010, and for patients who have diabetes, chronic kidney disease, or a
December 7, 2016. In total, 1514 patients who had a history of history of MI. The study used a combination drug of losartan
stroke within the previous 3 years were approached, but 234 potassium or other angiotensin II receptor blockers and hy-
refused to give informed consent. Eligible participants had the drochlorothiazide, amlodipine besylate, and spironolactone
following characteristics: age 50 to 85 years, independent am- to control BP. To achieve the target BP, patients received
bulation, systolic BP of 130 to 180 mm Hg or diastolic BP of 80 stepwise treatments orally every 4 weeks for 24 weeks
to 110 mm Hg on a regimen of 0 to 3 antihypertensive medi- at maximum during the titration period (trial protocol in
cations, and a history of stroke within the previous 3 years (evi- Supplement 1).
E2 JAMA Neurology Published online July 29, 2019 (Reprinted) jamaneurology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke Original Investigation Research
Outcome Measures Meta-analysis
The primary end point was recurrent stroke, including ische- We searched PubMed and the Cochrane Central Library data-
mic stroke and intracerebral hemorrhage. Recurrent stroke was base for RCTs that compared the effects of BP treatment using
clinically defined as a focal neurological deficit persisting for lon- 2 different targets in patients with prior cerebrovascular dis-
ger than 24 hours, as confirmed by magnetic resonance imaging ease through September 30, 2018. We used the Medical Sub-
or computed tomography. Stroke was deemed fatal if death oc- ject Headings (MeSH) and relevant search terms for cerebro-
curred within 30 days. Secondary end points included the fol- vascular disease (cerebrovascular disorders [MeSH] and all
lowing: reductions in ischemic stroke, subtype of ischemic stroke spellings of stroke, cerebral infarction, brain infarction, ische-
(including atherothrombotic infarction, cardioembolic infarc- mic stroke, intracranial hemorrhage, intracerebral hemor-
tion, lacunar infarction, or infarction due to other and un- rhage, cerebral hemorrhage, brain hemorrhage, hemorrhagic
known etiology), intracerebral hemorrhage, subarachnoid hem- stroke, transient ischemic attack, and cerebral ischemia) and
orrhage, transient ischemic attack, acute MI defined by standard the MeSH and relevant search terms for intensive BP lowering
criteria (compatible clinical history with changes on electrocar- (antihypertensive agents [MeSH] and all spellings of target BP,
diogram or in cardiac enzyme concentration), composite car- intensive BP, strict BP, and tight BP). The search was limited
diovascular events (cardiovascular death, nonfatal stroke, and to RCTs. The literature search, data extraction, and quality as-
nonfatal MI), all-cause death, and the composite of all-cause sessment were conducted independently by 2 authors (H.A.
death, nonfatal stroke, and nonfatal MI. Cardiovascular death and T.M.) using a standardized approach. All completed RCTs
was defined as sudden death, fatal stroke, fatal MI, fatal con- that compared more vs less intensive BP targets with pharma-
gestive heart failure, or death attributed to other cardiovascu- cological BP-lowering agents among patients with prior cere-
lar disease. All reported efficacy outcomes were confirmed by a brovascular disease were eligible for inclusion. Published re-
central adjudication committee that was masked to treatment ports were obtained for each trial, and standard information
assignment. Serious adverse events were defined as those that was extracted into a spreadsheet. The outcome for the meta-
were fatal or life threatening, that resulted in clinically signifi- analysis was recurrent stroke, including ischemic stroke and
cant or persistent disability, that required hospitalization, or that intracerebral hemorrhage. For each trial, we calculated the rela-
were judged as a significant hazard or harm that required medi- tive risk and its variance according to the principle of intent
cal or surgical interventions. to treat. Summary estimates of the effects and 95% CIs were
calculated using a random-effects model with inverse-
Statistical Analysis variance weighting. The percentage of variability across stud-
Our original plan was to recruit 5000 patients. In 2014, chal- ies attributable to heterogeneity beyond chance was esti-
lenges in achieving recruitment targets prompted us to re- mated using the I2 statistic. Meta-analysis was performed using
view the accumulated masked study data. In consideration of a software program (Stata, version 15; StataCorp LP).
interim masked trial data showing an annual stroke recur-
rence rate of 4.6%, we revised our sample size to 2000 pa-
tients; we estimated that this sample size would provide 80%
power (at α = .05) to detect a minimum relative reduction of
Results
30% in the intensive treatment group, on the assumption that Enrollment and Baseline Characteristics
the cumulative recurrence rate of stroke would be 15.6% in the The independent data and safety monitoring committee rec-
standard group during approximately 3.5 years of follow-up ommended continuation of research at the first interim analy-
and a dropout rate of 10%. sis on August 14, 2016; however, the steering committee
In accordance with the intent-to-treat principle, all pa- stopped enrollment on December 31, 2016, before reaching the
tients except for those who immediately withdrew their con- planned sample size of 2000 because of slow recruitment and
sent and those without any information after randomization funding cessation. In total, 1280 patients were randomized, and
were included in the analysis. Cumulative incidence was es- 17 (1.3%) were excluded from the randomized population ow-
timated using the Kaplan-Meier method and compared using ing to protocol violation, unmet inclusion criteria, or imme-
a log-rank test between randomized groups. Incidences of out- diate withdrawal of consent (Figure 1); the remaining 1263 pa-
comes were also estimated using a person-year approach. The tients (mean [SD] age, 67.2 [8.8] years; 69.4% male) were
effects of strict BP control on outcomes were calculated using enrolled in the intent-to-treat analysis. A total of 1263 partici-
univariable Cox proportional hazards models and are re- pants were enrolled, including 1074 with ischemic stroke and
ported as hazard ratios (HRs) and 95% CIs. If multiple events 189 with intracerebral hemorrhage as the qualifying event, and
of the same type occurred, the time to event was calculated 1257 of 1273 (99.5%) were followed up for a mean (SD) of 3.9
as the time to first events. The effects of randomized treat- (1.5) years (range, 0-5.5 years) (Table 1). The mean BP at base-
ment on BP during the overall follow-up period were esti- line was 145.4/83.6 mm Hg. Baseline characteristics did not dif-
mated using linear mixed models. All analyses were based on fer substantially between the treatment groups. The median
the intent-to-treat principle and were performed with SAS (ver- time from qualifying stroke to randomization was 4.6 months
sion 9.4; SAS Institute Inc) or R (version 3.4.1; The R Founda- (interquartile range, 1.7-13.0 months). The frequency of per-
tion for Statistical Computing). The study was registered with manent discontinuation of BP-lowering therapy was similar be-
ClinicalTrials.gov (NCT01198496). The threshold of statisti- tween the randomized groups (15 of 630 [2.4%] in the stan-
cal significance was set at 2-sided P < .05. dard treatment group vs 12 of 633 [1.9%] in the intensive
jamaneurology.com (Reprinted) JAMA Neurology Published online July 29, 2019 E3
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Research Original Investigation Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke
Figure 1. Flow of Participants Included in the RESPECT Study Table 1. Patient Characteristics by Randomized Groups
Standard Intensive
1514 Assessment of eligibility Treatment Treatment
Characteristic (n = 630) (n = 633)
234 Did not give consent Age, mean (SD), y 67.3 (8.8) 67.2 (8.8)
Male, No. (%) 428 (67.9) 449 (70.9)
1280 Randomization Blood pressure at entry, mean (SD),
mm Hg
Systolic 145.7 (12.9) 145.1 (12.4)
640 Standard treatment 640 Intensive treatment Diastolic 83.7 (10.4) 83.6 (10.7)
BMI, mean (SD) 23.9 (3.3) 23.7 (3.2)
2 Had protocol violation 1 Had protocol violation History of hypertension, No. (%) 630 (100) 633 (100)
1 Did not meet inclusion 3 Did not meet inclusion
criteria criteria Diabetes, No. (%) 154 (24.4) 142 (22.4)
7 Withdrew consent 3 Withdrew consent
Dyslipidemia, No. (%) 234 (37.1) 224 (35.4)
Coronary heart disease, No. (%) 17 (2.7) 15 (2.4)
630 Received standard treatment 633 Received intensive treatment
Chronic kidney disease, No. (%)a 27 (4.3) 36 (5.7)
Atrial fibrillation, No. (%) 53 (8.4) 53 (8.4)
41 Withdrew consent 46 Withdrew consent
15 Discontinued intervention 12 Discontinued intervention Stroke/TIA before qualifying event, 99 (15.7) 94 (14.8)
4 Lost to follow-up 2 Lost to follow-up No. (%)
Qualifying event, No. (%)
630 Included in the analysis 633 Included in the analysis Ischemic stroke 542 (86.0) 532 (84.0)
Intracerebral hemorrhage 88 (14.0) 101 (16.0)
RESPECT indicates Recurrent Stroke Prevention Clinical Outcome. Time since qualifying event, 4.6 (1.7-12.7) 4.7 (1.8-13.2)
median (IQR), mo
Serum creatinine, mean (SD), mg/dL 0.81 (0.21) 0.83 (0.22)
treatment group). Among 1263 patients in the cohort, 6 pa-
Cholesterol, mean (SD), mg/dL
tients (0.5%) were lost to follow-up, and an additional 87 of
LDL 112.0 (34.5) 111.8 (32.2)
1257 patients (6.9%) withdrew their consent and ended their
HDL 54.1 (14.9) 54.4 (15.5)
follow-up early.
Plasma glucose, mean (SD), mg/dL 127.6 (52.8) 125.4 (41.6)
Glycated hemoglobin, % 5.7 (0.8) 5.7 (0.9)
BP Control
Antihypertensive drugs at entry
Two treatments resulted in a rapid and sustained between-
No. of medications, mean 1.4 1.5
group difference in systolic and diastolic BP (eFigure 1 in
ARB/ACE inhibitor, No. (%) 428 (67.9) 421 (66.5)
Supplement 2). At 1 year of follow-up, the achieved BP was
132.0/77.5 (95% CI, 130.9-133.0/76.6-78.3) mm Hg in the stan- Thiazide, No. (%) 80 (12.7) 88 (13.9)
dard target group and 123.7/72.8 (95% CI, 122.6-124.8/72.0- Calcium channel blocker, No. (%) 239 (37.9) 257 (40.6)
73.7) mm Hg in the intensive target group, for a mean differ- Other, No. (%) 56 (8.9) 43 (6.8)
ence of 8.3 mm Hg in systolic BP. Target BP levels were achieved Concomitant drugs at entry, No. (%)
by 61.7% (374 of 606) in the standard group and 32.0% (197 of Statin 225 (35.7) 210 (33.2)
615) in the intensive group. Throughout the overall follow-up Antiplatelet drug 455 (72.2) 442 (69.8)
period, the mean BP was 133.2/77.7 (95% CI, 132.5-133.8/77.1- Anticoagulant drug 68 (10.8) 68 (10.7)
78.4) mm Hg in the standard group and 126.7/74.4 (95% CI, Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin II
125.9-127.2/73.8-75.0) mm Hg in the intensive group, for a mean receptor blocker; BMI, body mass index (calculated as weight in kilograms
difference of 6.5/3.3 (95% CI, 5.7-7.5/2.5-4.2) mm Hg. The mean divided by height in meters squared); HDL, high-density lipoprotein; IQR,
interquartile range; LDL, low-density lipoprotein; TIA, transient ischemic attack.
number of antihypertensive drugs was 1.4 at baseline. At 1 year,
SI conversion factors: To convert cholesterol levels (HDL and LDL) to millimoles
patients in the intensive treatment group had received more
per liter, multiply by 0.0259; creatinine level to micromoles per liter, multiply by
antihypertensive drugs than those in the standard treatment 88.4; glucose level to millimoles per liter, multiply by 0.0555; and glycated
group, and the mean numbers of antihypertensive drugs were hemoglobin level to proportion of total hemoglobin, multiply by 0.01.
a
1.6 and 2.8 during the overall follow-up period in the stan- Defined as estimated glomerular filtration rate less than 60 mL/min/1.73 m2 of
dard and intensive groups, respectively. The relative distribu- body surface area.
tion of antihypertensive classes used was almost similar in the
2 groups, although the use of diuretics was greater in the in- in the standard treatment group was 2.26% compared with
tensive treatment group. 1.65% in the intensive treatment group (Table 2), with an HR
of 0.73; 95% CI, 0.49-1.11 (P = .15). Although the cumulative
Primary Outcome incidence of recurrent stroke seemed to separate over time be-
The primary outcome was stroke recurrence. During the fol- tween the randomized groups, the difference was not statis-
low-up period, 91 first recurrent strokes occurred. Of these, 79 tically significant (Figure 2). There was no heterogeneity in
(86.8%) were ischemic strokes, and 12 (13.2%) were intrace- treatment effect on the primary outcome in any of the clini-
rebral hemorrhages. The annualized rate of recurrent stroke cal subgroups (eFigure 2 in Supplement 2).
E4 JAMA Neurology Published online July 29, 2019 (Reprinted) jamaneurology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke Original Investigation Research
Table 2. Effects of Intensive Blood Pressure Treatment on Primary and Secondary Outcomes
No. of Events (Annual Rate)
Standard Treatment Intensive Treatment
Outcome (n = 630) (n = 633) Hazard Ratio (95% CI) P Value
Primary Outcome
Strokea 52 (2.26) 39 (1.65) 0.73 (0.49-1.11) .15
Secondary Outcomes
Ischemic stroke 41 (1.76) 38 (1.60) 0.91 (0.59-1.42) .69
Lacunar infarction 12 (0.50) 14 (0.58) 1.16 (0.54-2.52) .70
Atherothrombotic infarction 9 (0.37) 4 (0.16) 0.44 (0.14-1.42) .17 a
Ischemic stroke and intracerebral
Cardiogenic embolism 5 (0.21) 4 (0.16) 0.79 (0.21-2.96) .73 hemorrhage.
Other 16 (0.67) 19 (0.78) 1.17 (0.60-2.27) .65 b
When the bootstrap percentile
Intracerebral hemorrhage 11 (0.46) 1 (0.04) 0.09 (0.01-0.70)b .02b method was used for intracerebral
Subarachnoid hemorrhage 0 (0) 1 (0.04) Not calculable hemorrhage, the 95% CI was 0.00
to 0.29, and the P value was less
Transient ischemic attack 3 (0.12) 8 (0.33) 2.66 (0.71-10.02) .15 than .001.
Myocardial infarction 4 (0.17) 5 (0.20) 1.23 (0.33-4.59) .75 c
Cardiovascular death, nonfatal
Major vascular eventc 59 (2.57) 46 (1.95) 0.76 (0.52-1.12) .17 stroke, and nonfatal myocardial
infarction.
All-cause death 37 (1.52) 30 (1.22) 0.80 (0.49-1.29) .36
d
All-cause death, nonfatal stroke,
Composite outcomed 86 (3.75) 68 (2.88) 0.77 (0.56-1.06) .11
and nonfatal myocardial infarction.
Secondary Outcomes Figure 2. Cumulative Incidence of Stroke by Randomized Groups
With regard to secondary end points, the rate of intracerebral
hemorrhage (0.04% per patient-year) was reduced in the in- 20
P = .14
Standard
by log-rank
treatment
test
tensive treatment group compared with that in the standard
Cumulative Incidence, %
group (0.46% per patient-year) (HR, 0.09; 95% CI, 0.01-0.70; 15
P = .02). However, the rates of ischemic stroke (1.60% per pa-
tient-year in the intensive group vs 1.76% per patient-year in 10 Standard treatment
the standard group), subtypes of ischemic stroke, and mortal-
ity were similar (Table 2). 5 Intensive treatment
Adverse Events
0
Serious adverse events were similar between the 2 groups 0 1 2 3 4 5
(eTable in Supplement 2). Adverse events related to hypoten- Time Since Randomization, y
No. at risk
sion, such as syncope and dizziness, were also infrequent and Standard treatment 630 578 495 419 308 170
similar between the groups. The most frequent serious ad- Intensive treatment 633 591 523 442 318 165
verse event was malignant neoplasm in both groups (5.08%
Stroke is a composite of ischemic stroke and intracerebral hemorrhage.
in the standard treatment group and 3.63% in the intensive
treatment group).
(I2 = 0%) (Figure 3). When the absolute risk difference was
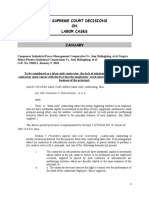
Updated Meta-analysis pooled for all 4 trials, the estimated risk difference was −1.5%
Three RCTs (the SPS3 trial,10 the Prevention After Stroke– (95% CI, −2.6% to −0.4%), and the estimated number needed
Blood Pressure [PAST-BP] trial,13 and the Prevention of De- to treat to avoid 1 recurrent stroke was 67 (95% CI, 39-250). In
cline in Cognition After Stroke Trial [PODCAST]14) investi- a meta-analysis performed for ischemic and hemorrhagic stroke
gated the effects of intensive BP lowering on recurrent stroke separately, the pooled risk ratio favored intensive BP control
(cerebral infarction and intracerebral hemorrhage for the SPS3 only for hemorrhagic stroke (relative risk, 0.25; 95% CI, 0.07-
trial10 and any stroke for the others) among patients with prior 0.90) and not for ischemic stroke (relative risk, 0.88; 95% CI,
cerebrovascular disease (target systolic BP <125 mm Hg or <130 0.71-1.08) (eFigure 3 in Supplement 2).
mm Hg). A meta-analysis of the 3 prior trials showed that no
statistically significant reduction in recurrent stroke was seen
in intensive BP lowering than in control treatment (relative risk,
0.80; 95% CI, 0.63-1.00; P = .05) (Figure 3). When an up-
Discussion
dated meta-analysis was conducted for the present trial with Among adults with a history of stroke, the RESPECT Study
the 3 prior trials of intensive BP treatment for secondary pre- showed that lowering BP to a target goal less than 120/80 mm
vention of stroke, the pooled risk ratio of this study and that Hg compared with the standard goal of less than 140/90 mm
of the 3 prior trials of intensive BP lowering for secondary stroke Hg resulted in nonsignificant reductions in all strokes. These
prevention favored intensive BP control (relative risk, 0.78; 95% effects were consistent across major subgroups, including pa-
CI, 0.64-0.96; P = .02), with no evidence of heterogeneity tients 70 years or older and patients with diabetes. When com-
jamaneurology.com (Reprinted) JAMA Neurology Published online July 29, 2019 E5
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Research Original Investigation Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke
Figure 3. Effects of Intensive Blood Pressure Lowering on Recurrent Stroke in a Meta-analysis
of Randomized Clinical Trials
No. of Events/No. of Patients Boxes and horizontal lines represent
Favors Favors
Intensive Standard Relative Risk Intensive Standard
relative risks and 95% CIs for each
Source Treatment Treatment (95% CI) Treatment Treatment trial. The size of boxes is proportional
Prior trials to the inverse variance. Diamonds
show the 95% CIs for pooled
SPS3,10 2013 118/1501 147/1519 0.81 (0.64-1.02)
estimates of effect and are centered
PAST-BP,13 2016 0/266 3/263 0.14 (0.01-2.72)
on the pooled relative risk.
PODCAST,14 2017 1/41 3/42 0.34 (0.04-3.15) PAST-BP indicates Prevention
Subtotal effect: I 2 = 0%, P = .05 119/1808 153/1824 0.80 (0.63-1.00) After Stroke–Blood Pressure13;
RESPECT 39/633 52/630 0.75 (0.50-1.11) PODCAST, Prevention of Decline in
Overall effect: I 2 = 0%, P = .02 158/2441 205/2454 0.78 (0.64-0.96) Cognition After Stroke Trial14;
RESPECT, Recurrent Stroke
0.1 1 10 Prevention Clinical Outcome; and
Relative Risk (95% CI) SPS3, Secondary Prevention of Small
Subcortical Strokes.10
bined in a meta-analysis of 3 other intensive BP treatment trials, 0.04% per patient-year in patients with achieved a systolic
there was a significant reduction in stroke recurrence in pa- BP of less than 120 mm Hg, which is consistent with the rate
tients randomized to intensive BP treatment. in the intensive treatment group of the present study
Blood pressure lowering has been strongly recom- (0.04% per patient-year). In the standard treatment group
mended for secondary prevention of chronic management af- of the RESPECT Study and the group with achieved BP of
ter stroke since the results of the PROGRESS 4 were pub- 130 to 139 mm Hg in the PROGRESS,9 the rate of intracere-
lished, but the optimum BP level and significance of intensive bral hemorrhage was also similar (0.10% vs 0.10% per
BP lowering needed to be examined. The SPS3 trial10 is the only patient-year). In contrast, the benefit of intensive BP lower-
large-scale study to date that has examined the effect of in- ing for the prevention of recurrent cerebral infarction is
tensive BP lowering in stroke survivors. In patients with lacu- unclear compared with standard treatment. In the post hoc
nar infarction, the researchers showed that within 180 days analysis of the PROGRESS,9 the risk of cerebral infarction
(median, 62 days) intensive BP lowering to a target less than was similar between the achieved BP levels of 130 to 139
130 mm Hg (mean, 127 mm Hg) resulted in a nonsignificant re- mm Hg and less than 130 mm Hg. In the SPS3 trial,10 the rate
duction in all strokes (HR, 0.81; 95% CI, 0.64-1.03) and a sig- of ischemic stroke was similar between the standard and
nificant reduction in intracerebral hemorrhages (HR, 0.37; 95% intensive treatment groups (HR, 0.84; 95% CI, 0.66-1.09).
CI, 0.15-0.95) compared with standard BP lowering to a target Our results also showed that the rate of cerebral infarction
of 130 to 149 mm Hg. Although the target goal of BP in the was similar between the standard and intensive treatment
RESPECT Study was 120 mm Hg, the results are in line with groups (HR, 0.91; 95% CI, 0.59-1.42). These results sug-
those of the SPS3 trial,10 and our meta-analysis showed that gested that intensive BP lowering did not show clear benefit
intensive BP lowering is more beneficial for the prevention of in preventing recurrent ischemic stroke, but this point
recurrent stroke, especially intracerebral hemorrhage. Fur- needs further investigation.
thermore, risk reduction and BP difference may be consistent
across trials: risk reduction and systolic BP difference, respec- Limitations
tively, were 0.72 and 9.0 mm Hg in the PROGRESS,4 0.81 and The RESPECT Study had several limitations. First, the trial did
11.0 mm Hg in the SPS3 trial,10 0.90 and 4.0 mm Hg in the Pre- not have sufficient power to draw statistical significance for
vention Regimen for Effectively Avoiding Second Strokes all strokes, which was the primary end point. However, our
(PRoFESS) trial,15 0.73 and 6.5 mm Hg in the RESPECT Study, meta-analysis that combined the results of 3 other trials found
and 0.73 and 7.0 mm Hg in a systematic review of all BP- a significant benefit of intensive BP lowering compared with
lowering trials.16 Another RCT testing the effect of 3 different standard treatment for stroke recurrence. Second, the assign-
BP targets (135 to <145, 125 to <135, and <125 mm Hg) on stroke ment of either treatment group herein was not masked, which
recurrence is ongoing.17 potentially introduced bias. However, the end points and ad-
The post hoc analysis of the PROGRESS9 showed that verse events were confirmed by an adjudication committee
lower BP is better and demonstrated that the target systolic who were unaware of the allocation, as in previous larger hy-
BP level should be less than 120 mm Hg. Our RESPECT pertension trials.10,11 Third, we excluded patients older than
Study supported that the proposed target level of BP in the 85 years because Japanese guidelines19 recommended a tar-
PROGRESS post hoc analysis is valid for stroke prevention. get BP less than 150/90 mm Hg in elderly hypertensive pa-
However, the consequences of BP lowering were more tients when the RESPECT Study started enrollment. It re-
evident for intracerebral hemorrhage than for cerebral mains unclear whether intensive BP lowering is beneficial for
infarction. Asian epidemiological data18 also have shown very elderly patients with a history of stroke. Fourth, none of
that the association between BP and hemorrhagic stroke the individual studies had significant results for secondary
is greater than that between BP and ischemic stroke. In stroke prevention, although the meta-analysis showed clear
the PROGRESS,9 the rate of intracerebral hemorrhage was benefit.
E6 JAMA Neurology Published online July 29, 2019 (Reprinted) jamaneurology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke Original Investigation Research
significant in this study. However, a meta-analysis of
Conclusions our results together w ith those of 3 prev ious trials
support that the use of a BP target less than 130/80 mm Hg
Rate reductions seen for recurrent stroke in the intensive is likely to be beneficial in patients with a history of
group compared w ith the standard group were not stroke.
ARTICLE INFORMATION Acquisition, analysis, or interpretation of data: Otsuka Pharmaceutical Co Ltd, Astellas Pharma Inc,
Accepted for Publication: April 25, 2019. Kitagawa, Yamamoto, Arima, Maeda, Kanzawa, AstraZeneca KK, Mochida Pharmaceutical Co, Ltd,
Eguchi, Kamiyama, Minematsu, Ueda, Ohya, Kohro, Sumitomo Dainippon Pharma Co Ltd, Amgen
Published Online: July 29, 2019. Yonemoto, Tanahashi, Umemura, Matsumoto. Astellas BioPharma KK, Esai Co, Ltd, and Pfizer
doi:10.1001/jamaneurol.2019.2167 Drafting of the manuscript: Kitagawa, Arima, Japan Inc. Dr Shimamoto reported receiving
Author Affiliations: Department of Neurology, Maeda, Sunami, Ueda, Rakugi, Ohya, Yonemoto, personal fees from Takeda, Sumitomo Dainippon
Tokyo Women’s Medical University, Shinjuku, Higaki, Kimura, Umemura, Matsumoto, Shimamoto, Pharma Co Ltd, MSD, Astellas Pharma, Boehringer
Tokyo, Japan (Kitagawa); Department of Neurology, Saruta. Ingelheim, and Bayer Yakuhin. Dr Ito reported
Kyoto Katsura Hospital, Nishikyo, Kyoto, Japan Critical revision of the manuscript for important receiving grants and/or personal fees from MSD,
(Yamamoto); Department of Preventive Medicine intellectual content: Kitagawa, Yamamoto, Daiichi Sankyo, Takeda, Astellas, and Boehringer
and Public Health, Fukuoka University Faculty of Kanzawa, Eguchi, Kamiyama, Minematsu, Ueda, Ingelheim. Dr Shimada reported receiving personal
Medicine, Jyonan, Fukuoka, Japan (Arima, Maeda); Ohya, Kohro, Yonemoto, Okada, Tanahashi, fees from Dainippon Sumitomo Ltd, and Daiichi
Department of Neurosurgery, Fukuzumi Hospital, Umemura, Matsumoto, Shimamoto, Ito, Saruta, Sankyo. No other disclosures were reported.
Matsuyama, Ehime, Japan (Sunami); Department of Shimada. Funding/Support: The Recurrent Stroke
Stroke Medicine, Institute of Brain and Blood Statistical analysis: Arima, Maeda, Kamiyama, Prevention Clinical Outcome (RESPECT) Study was
Vessel, Mihara Memorial Hospital, Isesaki, Gunnma, Kohro, Yonemoto, Matsumoto. funded by Merck and Co Inc, Bristol-Myers Squibb,
Japan (Kanzawa); Department of Internal Medicine, Obtained funding: Ueda, Ohya, Matsumoto, Ito, Towa Pharmaceutical Co, Ltd, and Omron
Hanyu General Hospital, Hanyu, Saitama, Japan Shimada. Corporation.
(Eguchi); Department of Neurosurgery, Nakamura Administrative, technical, or material support:
Memorial Hospital, Sapporo, Hokkaido, Japan Kitagawa, Kanzawa, Eguchi, Minematsu, Rakugi, Role of the Funder/Sponsor: The funding sources
(Kamiyama); General of the Hospital, National Ohya, Higaki, Umemura, Matsumoto, Shimamoto. had no role in the design and conduct of the study;
Cerebral and Cardiovascular Center, Suita, Osaka, Supervision: Kitagawa, Yamamoto, Kanzawa, collection, management, analysis, and
Japan (Minematsu); Department of Clinical Minematsu, Higaki, Tanahashi, Matsumoto, interpretation of the data; preparation, review, or
Pharmacology and Therapeutics, University of the Shimamoto, Ito, Saruta, Shimada. approval of the manuscript; and decision to submit
Ryukyus School of Medicine, Nakagamigunn, the manuscript for publication.
Conflict of Interest Disclosures: Dr Kitagawa
Okinawa, Japan (Ueda); Department of Geriatric reported receiving grants and personal fees from Group Information: The members of the Recurrent
and General Medicine, Osaka University Graduate Daiichi Sankyo, Bayer Inc, Takeda Pharmaceutical, Stroke Prevention Clinical Outcome (RESPECT)
School of Medicine, Suita, Osaka, Japan (Rakugi); Nippon Boehringer Ingelheim, Kyowa Hakko Kirin, Study Group are listed below.
Department of Cardiovascular Medicine, Sumitomo Dainippon Pharma, Astellas Pharma, and Chief Investigator: Kazuyuki Shimada, MD,
Nephrology and Neurology, University of the Sanofi. Dr Arima reported receiving personal fees Shin-Oyama City Hospital, Oyama, Tochigi, Japan.
Ryukyus School of Medicine, Nakagamigunn, from Bayer, Daiichi Sankyo, Fukuda Denshi, Kyowa
Okinawa, Japan (Ohya); Department of Writing Committee: Kazuyuki Shimada (chair), MD,
Kirin, and Takeda. Dr Minematsu reported receiving Shin-Oyama City Hospital, Oyama, Tochigi, Japan;
Cerebrovascular Medicine, Jichi Medical School, personal fees from Bayer Yakuhin, Otsuka
Shimotsuke, Tochigi, Japan (Kohro); Department of Kazuo Kitagawa, MD, Tokyo Women’s Medical
Pharmaceutical, Boehringer Ingelheim, University, Shinjuku, Tokyo, Japan; Yasumasa
Environmental Health, University of the Ryukyus AstraZeneca, Pfizer, Mitsubishi Tanabe Pharma
School of Medicine, Nakagamigunn, Okinawa, Yamamoto, MD, Kyoto Katsura Hospital, Nishikyo,
Cooperation, Japan Stryker, Kowa, Nihon Kyoto, Japan; Hisatomi Arima, MD, Fukuoka
Japan (Yonemoto); Department of Cerebrovascular Medi-Physics Co, BMS, Sawai Pharmaceutical Co,
Medicine and Neurology, National Hospital University Faculty of Medicine, Jyonan, Fukuoka,
Sumitomo Dainippon Pharma Co Ltd, Daiichi Japan; Shinichiro Ueda, MD, University of the
Organization Kyushu Medical Center Clinical Sankyo, Asteras Pharma, and Nippon Chemiphar
Research Institute, Chuo, Fukuoka, Japan (Okada); Ryukyus School of Medicine, Nakagamigun,
and reported receiving other financial support from Okinawa, Japan; Takahide Kohro, MD, Jichi Medical
Minami-Matsuyama Hospital, Matsuyama, Ehime, AstraZeneca, CSL Behring, Medico’s Hirata, and
Japan (Higaki); Department of Neurology, Saitama School, Shimotsuke, Tochigi, Japan; Koji Yonemoto,
Bayer Yakuhin. Dr Ueda reported receiving grants PhD, University of the Ryukyus Faculty of Medicine,
Medical University International Medical Center, from Kowa Soyaku, Bayer, Bristol-Myers Squibb,
Hidaka, Saitama, Japan (Tanahashi); Cardio-renal Nakagamigun, Okinawa, Japan.
Pfizer, Daiichi Sankyo, and Takeda Yakuhin and
and Health Research Institute, Nagoya, Aichi, Japan reported receiving personal fees from Ezai, Steering Committee: Kazuyuki Shimada (chair),
(Kimura); Yokohama Rosai Hospital, Yokohama, Novartis, MSD, and Boelinger Ingelheim. Dr Rakugi MD, Shin-Oyama City Hospital, Oyama, Tochigi,
Kanagawa, Japan (Umemura); Sakai City Medical reported receiving grants and/or personal fees from Japan; Satoshi Umemura, MD, Yokohama Rosai
Center, Sakai, Osaka, Japan (Matsumoto); Japan MSD, Astellas Pharma, Daiichi Sankyo, Dainippon Hospital, Yokohama, Kanagawa, Japan; Yasushi
Health Care College, Sapporo, Hokkaido, Japan Sumitomo Pharma, Bayer Yakuhin, Kyowa Hakko Okada, MD, National Hospital Organization Kyushu
(Shimamoto); Department of Nephrology Kirin, Mochida Pharmaceutical, Nippon Boehringer Medical Center, Chuo, Fukuoka, Japan; Genjiro
Endocrinology and Vascular Medicine, Tohoku Ingelheim, Takeda Pharmaceutical, Mitsubishi Kimura, MD, Cardio-renal and Health Research
University School of Medicine, Sendai, Miyagi, Tanabe Pharma, Novartis Pharma, Otsuka Institute, Nagoya, Aichi, Japan; Kazuaki Shimamoto,
Japan (Ito); Department of Internal Medicine, Keio Pharmaceutical, Pfizer Japan, Shionogi & Co, and MD, Japan Health Care College, Sapporo, Hokkaido,
University School of Medicine, Tokyo, Japan Teijin Pharma. Dr Ohya reported receiving grants Japan; Norio Tanahashi, MD, Saitama Medical
(Saruta); Shin-Oyama City Hospital, Oyama, Tochigi, and/or personal fees from Takeda Pharma, Daiichi University International Medical Center, Hidaka,
Japan (Shimada). Sankyo, Novartis Pharma, Asterasu, Dainippon Saitama, Japan; Jitsuo Higaki, MD,
Author Contributions: Dr Shimada had full access Sumitomo, MSD, Bayer, Pfizer, and Boehringer Minami-Matsuyama Hospital, Matsuyama, Ehime,
to all of the data in the study and takes Ingelheim. Dr Umemura reported receiving grants Japan; Masayasu Matsumoto, MD, Sakai City
responsibility for the integrity of the data and the from Dainippon Sumitomo, Asteras, Pfizer, Nippon Medical Center, Sakai, Osaka, Japan.
accuracy of the data analysis. Dr Shimada was the Boehringer Ingelheim, Daiichi Sankyo, and Takeda Protocol Committee: Masayasu Matsumoto (chair),
principal investigator. and reported receiving personal fees from Nippon MD, Sakai City Medical Center, Sakai, Osaka, Japan;
Concept and design: Kitagawa, Yamamoto, Sunami, Boehringer Ingelheim and Takeda. Dr Matsumoto Sadayoshi Ito, MD, Tohoku University School of
Ueda, Rakugi, Ohya, Okada, Higaki, Tanahashi, reported receiving personal fees from Kowa Medicine, Sendai, Miyagi, Japan; Shinichiro Ueda, MD,
Kimura, Umemura, Matsumoto, Shimamoto, Ito, Pharmaceutical Co Ltd, Takeda Pharmaceutical Co University of the Ryukyus School of Medicine,
Saruta, Shimada. Ltd, Bayer Yakuhin, Ltd, Sanofi KK, Daiichi Sankyo, Nakagamigun, Okinawa, Japan; Yusuke Ohya, MD,
jamaneurology.com (Reprinted) JAMA Neurology Published online July 29, 2019 E7
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Research Original Investigation Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke
University of the Ryukyus Graduate School of Ebetsu City Hospital, Ebetsu, Hokkaido, Japan; Yoshihiro Tanaka, MD, Dokkyo Medical University
Medicine, Nakagamigun, Okinawa, Japan; Kazuo Kiyomi Kuroshima, MD, Katsumi Takizawa, MD, and Saitama Medical Center, Koshigaya, Saitama, Japan;
Kitagawa, MD, Tokyo Women’s Medical University, Kazuto Yoshida, MD, Japanese Red Cross Asahikawa Shigehisa Inokuma, MD, Inokuma Clinic, Kawagoe,
Shinjuku, Tokyo, Japan; Yasumasa Yamamoto, MD, Hospital, Asahikawa, Hokkaido, Japan; Hideo Saitama, Japan; Yuji Kato, MD, and Norio Tanahashi,
Kyoto Katsura Hospital, Nishikyo, Kyoto, Japan; Morimoto, MD, Fukagawa Municipal Hospital, MD, Saitama Medical University International
Hiromi Rakugi, MD, Osaka University Graduate Fukagawa, Hokkaido, Japan; Naoyuki Hasebe, MD, Medical Center, Hidaka, Saitama, Japan.
School of Medicine, Suita, Osaka, Japan. Asahikawa Medical University, Asahikawa, Chiba Prefecture: Naoki Ishige, MD, National
End Point Committee: Kazuo Minematsu (chair), Hokkaido, Japan; Satoshi Koyama, MD, and Junichi Hospital Organization Chiba Medical Center, Chiba,
MD, General of the Hospital, National Cerebral and Maruyama, MD, Asahikawa Rehabilitation Hospital, Japan; Kazuhiro Muramatsu, MD, Shigeru Nogawa,
Cardiovascular Center, Suita, Osaka, Japan; Asahikawa, Hokkaido, Japan; Shinsuke Irie, MD, MD, and Takahito Yoshizaki, MD, Tokyo Dental
Kazuomi Kario, MD, Jichi Medical School, Kushiro Neurosurgical Clinic, Kushiro, Hokkaido, College Ichikawa General Hospital, Ichikawa, Chiba,
Shimotsuke, Tochigi, Japan; Yoshihiko Saito, MD, Japan. Japan; Takashi Ohashi, MD, Tokyo Women’s Medical
Nara Medical University, Kashihara, Nara, Japan; Aomori Prefecture: Takahiro Nakano, MD, Yukari University Yachiyo Medical Center, Yachiyo, Chiba,
Yasuo Terayama, MD, Iwate Medical University, Ogasawara, MD, and Hiroki Ohkuma, MD, Hirosaki Japan; Sumio Suda, MD, Kimitsu Chuo Hospital,
Morioka, Iwate, Japan; Kazunori Toyoda, MD, University Graduate School of Medicine, Hirosaki, Kisarazu, Chiba, Japan.
General of the Hospital, National Cerebral and Aomori, Japan; Kazuo Shibanai, MD, Hachinohe JRC Tokyo: Yasuyuki Iguchi, MD, and Hidetaka
Cardiovascular Center, Suita, Osaka, Japan; Hospital, Hachinohe, Aomori, Japan. Mitsumura, MD, The Jikei University School of
Takafumi Okura, MD, Ehime University Graduate Akita Prefecture: Kentaro Hikichi, MD, Shinya Medicine, Minato, Tokyo, Japan; Tomohide Adachi,
School of Medicine, Toon, Ehime, Japan; Haruhiko Kobayashi, MD, Junta Moroi, MD, Taizen Nakase, MD, Haruhiko Hoshino, MD, Fumie Konoeda, MD,
Hoshino, MD, Tokyo Saiseikai Central Hospital, MD, Takeshi Okada, MD, Daiki Takano, MD, and Koichi Oki, MD, Tokyo Saiseikai Central Hospital,
Minato, Tokyo, Japan; Hirofumi Makino, MD, Shunsuke Takenaka, MD, and Shotaro Yoshioka, Minato, Tokyo, Japan; Ryota Tanaka, MD, Takao
Okayama University Graduate School of Medicine, MD, Research Institute for Brain and Blood Vessels– Urabe, MD, and Kazuo Yamashiro, MD, Juntendo
Okayama, Japan; Kazuo Eguchi, MD, Hanyu General Akita, Akita, Japan; Toshiharu Yanagisawa, MD, University Hospital, Bunkyo, Tokyo, Japan; Akihiro
Hospital, Hanyu, Saitama, Japan; Haruhito Uchida, Akita University Graduate School of Medicine, Akita, Ito, MD, Hirofumi Nakatomi, MD, and Masaaki
MD, Okayama University Graduate School of Japan; Yutaka Hirata, MD, Kita-Akita Municipal Shojima, MD, The University of Tokyo, Bunkyo,
Medicine, Okayama, Japan. Hospital, Kita-Akita, Akita, Japan. Tokyo, Japan; Kuniaki Otsuka, MD, and Koichi
Statistical Analysis Team: Hisatomi Arima (chair), Iwate Prefecture: Shu Konno, MD, Matuzono Shibata, MD, Tokyo Women’s Medical University
MD, Fukuoka University Faculty of Medicine, Jyonan, Second Hospital, Morioka, Iwate, Japan; Tomohiko Medical Center East, Arakawa, Tokyo, Japan; Takato
Fukuoka, Japan; Takahide Khoro, MD, Jichi Medical Sato, MD, National Hospital Organization, Iwate Abe, MD, Yoshiaki Itoh, MD, Koichi Oki, MD, and
School, Shimotsuke, Tochigi, Japan; Koji Yonemoto, Hospital, Ichinoseki, Iwate, Japan. Norihiro Suzuki, MD, Keio University School of
PhD, University of the Ryukyus Faculty of Medicine, Medicine, Shinjuku, Tokyo, Japan; Kazuo Kitagawa,
Nakagamigun, Okinawa, Japan. Yamagata Prefecture: Miiko Ito, MD, Rei Kondo, MD, and Sono Toi, MD, Tokyo Women’s Medical
MD, Wataru Mori, MD, and Shinjiro Saito, MD, University, Shinjuku, Tokyo, Japan; Tamio Teramoto,
Independent Data and Safety Monitoring Yamagata City Hospital SAISEIKAN, Yamagata,
Committee: Shinichiro Uchiyama (chair), MD, MD, Teikyo University, Itabashi, Tokyo, Japan;
Japan; Yasuaki Kokubo, MD, Yamagata University Atsushi Fukunaga, MD, Yuki Kujuro, MD, Kouichi
International University of Health and Welfare, Faculty of Medicine, Yamagata, Japan.
Minato, Tokyo, Japan; Hideki Etani, MD, OBP Clinic, Ohta, MD, Takashi Osada, MD, and Katuyoshi
Chuou, Osaka, Japan; Tatsuo Kohriyama, MD, Brain Miyagi Prefecture: Hideaki Kato, MD, and Hideki Shimizu, MD, Tachikawa Hospital, Tachikawa,
Attack Center, Ota Memorial Hospital, Fukuyama, Oyama, MD, Senseki Hospital, Higashi-Matsushima, Tokyo, Japan; Yasuhisa Kitagawa, MD, and Kentaro
Hiroshima, Japan; Hidekazu Tomimoto, MD, Mie Miyagi, Japan; Kaneyuki Matsuo, MD, Matsuo Kenko Tokuoka, MD, Tokai University Hachioji Hospital,
University Graduate School of Medicine, Tsu, Mie, Clinic, Sendai, Miyagi, Japan; Masahiro Matsumoto, Hachioji, Tokyo, Japan.
Japan; Taku Yoshio, MD, Jichi Medical University MD, and Mari Nakamura, MD, Tohoku Rosai Kanagawa Prefecture: Masao Omura, MD,
Hospital, Shimotsuke, Tochigi, Japan; Takao Saruta, Hospital, Sendai, Miyagi, Japan. Yokohama Rosai Hospital, Yokohama, Kanagawa,
MD, Keio University School of Medicine, Shinjuku, Fukushima Prefecture: Takayuki Koizumi, MD, and Japan; Hideyuki Kikyo, MD, Yokohama Public
Tokyo, Japan; Shotai Kobayashi, MD, Shimane Hiroyuki Sato, MD, Takeda General Hospital, Medical Center for Stroke and Neurology, Yokohama,
University, Izumo, Shimane, Japan. Aizuwakamatsu, Fukushima, Japan. Kanagawa, Japan; Tomoya Kamide, MD, Yoshihisa
Data Management Center: Hiroko Usami, PhD, Ibaraki Prefecture: Yasushi Shibata, MD, Mito Kitamura, MD, Katsuyoshi Miyashita, MD, Kentaro
Nonprofit Organization RESPECT Study Group, Kyodo General Hospital, Mito, Ibaraki, Japan. Mori, MD, Hiroshi Shima, MD, and Akira Tamase,
Hachioji, Tokyo, Japan. MD, Yokohama Sakae Kyosai Hospital, Yokohama,
Tochigi Prefecture: Kazuo Eguchi, MD, and Kanagawa, Japan; Tsugio Akutsu, MD, and
RESPECT Study Investigators: The investigators Kazuomi Kario, MD, Jichi Medical University, Kazutoshi Nishiyama, MD, Kitasato University
are listed below by location in Japan and by Shimotsuke, Tochigi, Japan; Masaaki Hashimoto, School of Medicine, Sagamihara, Kanagawa, Japan;
institution. MD, Kazuo Eguchi, MD, Hideharu Kurita, MD, and Shunya Takizawa, MD, and Tsuyoshi Uesugi, MD,
Hokkaido: Satoshi Iihoshi, MD, Takeshi Mikami, Eiji Matsumoto, MD, IUHW Hospital, Shiobara, Tokai University School of Medicine, Isehara,
MD, Nobuhiro Mikuni, MD, Kei Miyata, MD, and Tochigi, Japan. Kanagawa, Japan.
Tomohiro Murakami, MD, Sapporo Medical Gunma Prefecture: Koji Ishiguro, MD, Takasaki Nagano Prefecture: Uichi Ikeda, MD, Megumi
University, Sapporo, Hokkaido, Japan; Hideki Endo, General Medical Center, Takasaki, Gunma, Japan; Koshikawa, MD, and Saeko Yamasaki, MD, Shinshu
MD, Takahito Fukui, MD, Kentaro Fumoto, MD, Keiji Ken Asakura, MD, Hiroya Fujimaki, MD, and Kazuki University Graduate School of Medicine, Matsumoto,
Hara, MD, Kaori Honjo, MD, Kenji Kamiyama, MD, Wakabayashi, MD, Maebashi Red Cross Hospital, Nagano, Japan; Atsushi Inoue, MD, Nagano
Yusuke Kinoshita, MD, Masana Maeda, MD, Masaaki Maebashi, Gunma, Japan; Kazunori Akaji, MD, Tomo Prefectural Kiso Hospital, Kisofukushima, Nagano,
Mikamoto, MD, Daisuke Mori, MD, Takeo Horikoshi, MD, Tadashige Kano, MD, Takao Japan.
Murahashi, MD, Ryota Nomura, MD, Shusaku Noro, Kanzawa, MD, Takehiro Katano, MD, Hiroaki
MD, Tatsuya Ogino, MD, Masahiro Okuma, MD, Kimura, MD, Ban Mihara, MD, Kentaro Suzuki, MD, Ishikawa Prefecture: Yasuko Matsumoto, MD, and
Yasuhumi Otake, MD, Koichiro Shindo, MD, Hironori and Yohei Takayama, MD, Institute of Brain and Kazuyoshi Yamaguchi, MD, Ishikawa Prefectural
Sugio, MD, Hidekazu Takada, MD, Kazuki Takahira, Blood Vessel Mihara Memorial Hospital, Isesaki, Central Hospital, Kanazawa, Ishikawa, Japan;
MD, Akiko Takeuchi, MD, Toshiichi Watanabe, MD, Gunma, Japan. Genjirou Hirose, MD, and Satoshi Kontani, MD,
and Yohei Yamaguchi, MD, Nakamura Memorial Asanogawa General Hospital, Kanazawa, Ishikawa,
Saitama Prefecture: Akira Ishii, MD, Sin-ichi Japan; Kazuya Takasawa, MD, Public Central
Hospital, Sapporo, Hokkaido, Japan; Takeo Momomura, MD, Hitoshi Sugawara, MD, and
Abumiya, MD, and Kiyohiro Houkin, MD, Hokkaido Hospital of Matto Ishikawa, Hakusan, Ishikawa,
Takeshi Yamashita, MD, Saitama Medical Center, Japan.
University, Sapporo, Hokkaido, Japan; Shigeki Jichi Medical University, Saitama, Japan; Uichi
Matsumura, MD, and Tomohiro Murakami, MD, Kaneko, MD, and Toshie Takahashi, MD, Saitama Niigata Prefecture: Katsumi Hirahara, MD,
Sapporo Miyanosawa Neurosurgical Hospital, Red Cross Hospital, Saitama, Japan; Toshinari Arai, Hirahara Naika Clinic, Jouetsu, Niigata, Japan;
Sapporo, Hokkaido, Japan; Rikiya Shinohe, MD, MD, Soka Municipal Hospital, Soka, Saitama, Japan; Makoto Kodama, MD, and Nobue Yagihara, MD,
E8 JAMA Neurology Published online July 29, 2019 (Reprinted) jamaneurology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke Original Investigation Research
Niigata University School of Medicine, Niigata, Osaka, Japan; Shoji Arihiro, MD, Ryosuke Doijiri, University Graduate School of Medicine, Hiroshima,
Japan. MD, Kyoko Higashida, MD, Katsufumi Kajimoto, MD, Japan; Hayato Araki, MD, and Ryo Ogami, MD,
Shizuoka Prefecture: Takashi Hata, MD, and Kotaro Miyashita, MD, Kazuyuki Nagatsuka, MD, Mazda Hospital, Akigun, Hiroshima, Japan; Tsuyoshi
Makoto Hori, MD, Shizuoka City Shimizu Hospital, Kozue Saito, MD, Yuri Sugiura, MD, Hotake Torii, MD, National Hospital Organization Kure
Shimizu, Shizuoka, Japan. Takizawa, MD, Takako Torii, MD, Kazunori Toyoda, Medical Center and Chugoku Cancer Center, Kure,
MD, and Chiaki Yokota, MD, General of the Hospital, Hiroshima, Japan; Noboru Yokoyama, MD, and
Aichi Prefecture: Rokuhei Oda, MD, Nishio National Cerebral and Cardiovascular Center, Suita, Takakazu Yokoyama, MD, Yokoyama Hospital, Kure,
Municipal Hospital, Nishio, Aichi, Japan; Ayuka Osaka, Japan; Yoshinaga Kajimoto, MD, and Hiroshima, Japan; Satoshi Kataoka, MD, and Takeshi
Kubo, MD, and Satoshi Okuda, MD, National Toshihiko Kuroiwa, MD, Osaka Medical College, Kitamura, MD, Chugoku Rosai Hospital, Kure,
Hospital Organization Nagoya Medical Center, Takatsuki, Osaka, Japan; Ryuzo Fukunaga, MD, and Hiroshima, Japan.
Nagoya, Aichi, Japan; Kentaro Yamada, MD, Nagoya Tsutomu Takahashi, MD, JCHO Hoshigaoka Medical
City East Medical Center, Nagoya, Aichi, Japan; Yamaguchi Prefecture: Takashi Kanda, MD,
Center, Hirakata, Osaka, Japan; Kazutami Nakao, Toshihiko Maeda, MD, and Fumitaka Shimizu, MD,
Hiroki Takeuchi, MD, Higashi Nagoya National MD, Kawachi General Hospital, Higashiosaka,
Hospital, Nagoya, Aichi, Japan; Yoshio Araki, MD, Yamaguchi University Graduate School of Medicine,
Osaka, Japan; Yuta Kajiyama, MD, Yasuyoshi Ube, Yamaguchi, Japan; Kozaburo Seki, MD,
Mizuki Ito, MD, Joe Senda, MD, and Toshihiko Kimura, MD, Takashi Naka, MD, Hironori Otomune,
Wakabayashi, MD, Nagoya University Graduate Yamaguchi Rosai Hospital, Sanyoonoda, Yamaguchi,
MD, Takao Tanahashi, MD, and Takuya Uehara, MD, Japan.
School of Medicine, Nagoya, Aichi, Japan; Shinji Ito, Higashiosaka City Medical Center, Higashiosaka,
MD, and Tatsuro Mutoh, MD, Fujita Health Osaka, Japan; Hiroyuki Hashimoto, MD, and Kagawa Prefecture: Yuko Bando, MD, and Masaki
University School of Medicine, Toyoake, Aichi, Japan. Toshihiko Uematsu, MD, Osaka Rosai Hospital, Ohara, MD, Ayagawa National Health Insurance SUE
Gifu Prefecture: Yukinori Kawase, MD, Hashimoto Sakai, Osaka, Japan. Hospital, Ayautagun, Kagawa, Japan.
Clinic, Gifu, Japan; Fumio Ando, MD, Ando Clinic, Nara Prefecture: Kazuo Kataoka, MD, Kinki Kochi Prefecture: Masahiro Yamasaki, MD,
Kani, Gifu, Japan. University Nara Hospital, Ikoma, Nara, Japan; Chikamori Hospital, Okawasuji, Kochi, Japan;
Mie Prefecture: Shinya Okamoto, MD, Iwasaki Satoshi Okayama, MD, and Satoshi Somekawa, MD, Noritaka Masahira, MD, Tetsuya Ueba, MD, and
Hospital, Tsu, Mie, Japan; Takuya Shimada, MD, and Nara Medical University, Kashihara, Nara, Japan; Yusuke Ueba, MD, Kochi Medical School, Nankoku,
Akihiro Shindo, MD, Sakakibara Onsen Hospital, Shuichi Yamada, MD, Oyodo Town Hospital, Ikoma, Kochi, Japan.
Tsu, Mie, Japan; Masakatsu Nishikawa, MD, Atsushi Nara, Japan; Rie Sasaki, MD, and Shigeru Yamano, Ehime Prefecture: Norio Sunami, MD, Matsuyama
Niwa, MD, Ryogen Sasaki, MD, Akihiro Shindo, MD, MD, Nara Prefecture General Rehabilitation Center, Shimin Hospital, Matsuyama, Ehime, Japan; Yuichi
and Hidekazu Tomimoto, MD, Mie University Shikigun, Nara, Japan. Fujimoto, MD, Keiko Haro, MD, Hidenori Ogata, MD,
Graduate School of Medicine, Tsu, Mie, Japan; Wakayama Prefecture: Naoyuki Nakao, MD, and and Norihiko Shida, MD, Matsuyama Red Cross
Hiroto Murata, MD, Saiseikai Matsusaka General Shinji Obayashi, MD, Wakayama Medical University, Hospital, Matsuyama, Ehime, Japan; Takeshi
Hospital, Matsusaka, Mie, Japan; Kenichiro Yata, Kimiidera, Wakayama, Japan. Matsumoto, MD, and Kensho Okamoto, MD, Ehime
MD, Suzuka Kaisei Hospital, Suzuka, Mie, Japan. Prefectural Central Hospital, Matsuyama, Ehime,
Hyogo Prefecture: Hirotoshi Hamaguchi, MD, Japan; Jitsuo Higaki, MD, and Takafumi Okura, MD,
Shiga Prefecture: Koushun Matsuo, MD, Tatsushi Toda, MD, and Kazuo Washida, MD, Kobe
Omihachiman Community Medical Center, Ehime University Graduate School of Medicine, Toon,
University Graduate School of Medicine, Kobe, Ehime, Japan; Ryuichi Kawamoto, MD, Seiyo
Omihachiman, Shiga, Japan. Hyogo, Japan; Taku Hoshi, MD, Tomoyuki Kono, Municipal Nomura Hospital, Seiyo, Ehime, Japan.
Kyoto: Hideo Yagi, MD, Koseikai Takeda Hospital, MD, Hiroaki Sekiya, MD, Norifumi Sugo, MD, Kenichi
Shimogyo, Kyoto, Japan; Toshiyuki Shiogai, MD, Todo, MD, Masaya Togo, MD, Hiroshi Yamagami, Fukuoka Prefecture: Shuji Arakawa, MD, and Shoji
Kyoto Takeda Hospital, Shimogyo, Kyoto, Japan; MD, and Shiro Yamamoto, MD, Kobe City Medical Arihiro, MD, Kyushu Rosai Hospital, Kitakyushu,
Yoshinari Nagakane, MD, and Yasumasa Yamamoto, Center General Hospital, Kobe, Hyogo, Japan; Fukuoka, Japan; Hirofumi Shii, MD, and Hidetoshi
MD, Kyoto Second Red Cross Hospital, Kamigyo, Yoshihiko Shiro, MD, and Norifumi Sugo, MD, Kobe Kanai, MD, Kokura Kinen Hospital, Kitakyushu,
Kyoto, Japan; Jun Fujinami, MD, Masanori City Medical Center West Hospital, Kobe, Hyogo, Fukuoka, Japan; Shigeru Fujimoto, MD, Juro
Nakagawa, MD, Ryo Ohara, MD, and Yasuhiro Tomii, Japan; Hirotoshi Hamaguchi, MD, Kita-Harima Jinnouchi, MD, Takayuki Matsuki, MD, and Masato
MD, Kyoto Prefectural University of Medicine, Medical Center, Ono, Hyogo, Japan; Toshio Takaoka, Osaki, MD, Steel Memorial Yawata Hospital,
Kamigyo, Kyoto, Japan; Yoshiki Arakawa, MD, MD, Hyogo College of Medicine, Nishinomiya, Kitakyushu, Fukuoka, Japan; Kimika Arakawa, MD,
Takeshi Funaki, MD, Masafumi Ihara, MD, Akihiro Hyogo, Japan. Ai Ibaraki, MD, Kanako Kiyohara, MD, Yuko Ohta,
Kitamura, MD, Takakuni Maki, MD, Susumu MD, Hideyuki Oniki, MD, Minako Sakaki, MD,
Shimane Prefecture: Satoshi Abe, MD, Chizuko Mitsuhiro Tominaga, MD, and Takuya Tsuchihashi,
Miyamoto, MD, Yoshifumi Nakaya, MD, Ryosuke Hamada, MD, Masaki Ishihara, MD, Katuhiko
Takahashi, MD, Yohei Takenobu, MD, and Kazumichi MD, National Hospital Organization Kyushu Medical
Kadota, MD, Tomonori Nakagawa, MD, Hiroaki Center, Chuo, Fukuoka, Japan; Saho Higashi, MD,
Yoshida, MD, Kyoto University Graduate School of Oguro, MD, Hiroyuki Takayoshi, MD, Takuya
Medicine, Sakyo, Kyoto, Japan; Tadashi Ino, MD, Hiromi Ishikawa, MD, Koji Ishitsuka, MD, Jiro
Yamaguchi, MD, and Shuuhei Yamaguchi, MD, Kitayama, MD, and Hiroshi Nakane, MD, National
Rakuwakai Otowa Hospital, Yamashina, Kyoto, Shimane University Faculty of Medicine, Izumo,
Japan; Nagako Murase, MD, and Ryo Ohotani, MD, Hospital Organization Fukuoka Higashi Medical
Shimane, Japan; Ryo Mizuhara, MD, Kazunori Center, Koga, Fukuoka, Japan; Takeo Yoshimura,
National Hospital Organization Kyoto Medical Okada, MD, and Shingo Yamagata, MD, Ohda
Center, Fushimi, Kyoto, Japan; Yasuhiro Tomii, MD, MD, Fukuoka City Hospital, Hakata, Fukuoka, Japan;
Municipal Hospital, Ohda, Shimane, Japan; Kazunori Shunsuke Kakino, MD, and Yoshirou Kaneko, MD,
and Yasumasa Yamamoto, MD, Kyoto Katsura Okada, MD, Ohda Silver Clinic, Ohda, Shimane,
Hospital, Nishikyo, Kyoto, Japan; Atsushi Fukuoka Tokushukai Medical Center, Kasuga,
Japan; Akira Sasaki, MD, JCHO Tamatsukuri Fukuoka, Japan.
Kawashima, MD, and Akiko Watanabe, MD, Hospital, Matsue, Shimane, Japan.
Fukuchiyama City Hospital, Fukuchiyama, Kyoto, Kumamoto Prefecture: Junnosuke Inoue, MD,
Japan; Yuko Hayashi, MD, Takuma Ohmichi, MD, Rei Okayama Prefecture: Koji Abe, MD, Kentaro Kumamoto Jikei Hospital, Kumamoto, Japan.
Yasuda, MD, Akira Yoshioka, MD, and Natsuko Yuki, Deguchi, MD, Shoko Deguchi, MD, and Yumiko
Nakano, MD, Okayama University Graduate School Kagoshima Prefecture: Yoshikazu Maruyama, MD,
MD, National Hospital Organization Maizuru Medical Imakiire General Hospital, Shimotatuo, Kagoshima,
Center, Maizuru, Kyoto, Japan; Masahiro Makino, of Medicine, Okayama, Japan; Satoshi Hirai, MD,
Masaaki Uno, MD, and Kimihiko Yokosuka, MD, Japan.
MD, Yasuhiro Tomii, MD, and Tatsuyuki Yamaguchi,
MD, Kyoto Chubu Medical Center, Nantan, Kyoto, Kawasaki Medical School, Kurashiki, Okayama, Okinawa Prefecture: Katsunori Isa, MD, Yusuke
Japan. Japan; Yasuhiro Manabe, MD, National Hospital Ohya, MD, and Hirokuni Sakima, MD, University of
Organization Okayama Medical Center, Kita, the Ryukyus Graduate School of Medicine,
Osaka: Jyo Matsuzaki, MD, Hitoshi Niki, MD, Okayama, Japan. Nakagamigun, Okinawa, Japan; Seigo Nakada, MD,
Shoichi Shiraishi, MD, and Takehiko Yanagihara, MD, Chibana Clinic, Chibana, Okinawa, Japan.
Tane General Hospital, Nishi, Osaka, Japan; Keiichi Hiroshima Prefecture: Hijiri Ito, MD, Vihara
Yamada, MD, Kansai Electric Power Hospital, Hananosato Hospital, Miyoshi, Hiroshima, Japan; Data Sharing Statement: See Supplement 3.
Fukushima, Osaka, Japan; Jun Hatate, MD, Kaori Shiro Aoki, MD, Naohisa Hosomi, MD, Yasuki Kihara, Additional Contributions: Hiroko Usami, PhD,
Miwa, MD, and Shuhei Okazaki, MD, Osaka MD, Tomohiko Kisaka, MD, Hirofumi Maruyama, chief secretary of the Recurrent Stroke Prevention
University Graduate School of Medicine, Suita, MD, and Masayasu Matsumoto, MD, Hiroshima Clinical Outcome (RESPECT) Study Group,
jamaneurology.com (Reprinted) JAMA Neurology Published online July 29, 2019 E9
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
Research Original Investigation Effect of Standard vs Intensive Blood Pressure Control on the Risk of Recurrent Stroke
performed data management and protocol and other vascular events: a systematic review. Stroke. PAST-BP (Prevention After Stroke–Blood Pressure)
manuscript preparation. Yasuko Ohtsuki, BA, 2003;34(11):2741-2748. doi:10.1161/01.STR. randomised controlled trial. BMJ. 2016;352:i708.
clinical research coordinator, International 0000092488.40085.15 doi:10.1136/bmj.i708
University of Health and Welfare Hospital, 7. Katsanos AH, Filippatou A, Manios E, et al. Blood 14. Bath PM, Scutt P, Blackburn DJ, et al; PODCAST
contributed to patient recruitment and acquisition pressure reduction and secondary stroke Trial Investigators. Intensive versus guideline blood
of informed consent. They were not compensated prevention: a systematic review and pressure and lipid lowering in patients with
for their contributions. We appreciate the metaregression analysis of randomized clinical previous stroke: main results from the pilot
contributions of all the investigators and other trials. Hypertension. 2017;69(1):171-179. doi:10.1161/ “Prevention of Decline in Cognition After Stroke
clinical and research staff involved in the trial. HYPERTENSIONAHA.116.08485 Trial” (PODCAST) randomised controlled trial. PLoS
8. Lewington S, Clarke R, Qizilbash N, Peto R, One. 2017;12(1):e0164608. doi:10.1371/journal.
REFERENCES pone.0164608
Collins R; Prospective Studies Collaboration.
1. Feigin VL, Forouzanfar MH, Krishnamurthi R, Age-specific relevance of usual blood pressure to 15. Yusuf S, Diener HC, Sacco RL, et al; PRoFESS
et al; Global Burden of Diseases, Injuries, and Risk vascular mortality: a meta-analysis of individual Study Group. Telmisartan to prevent recurrent
Factors Study 2010 (GBD 2010) and the GBD data for one million adults in 61 prospective studies. stroke and cardiovascular events. N Engl J Med.
Stroke Experts Group. Global and regional burden Lancet. 2002;360(9349):1903-1913. doi:10.1016/ 2008;359(12):1225-1237. doi:10.1056/
of stroke during 1990-2010: findings from the S0140-6736(02)11911-8 NEJMoa0804593
Global Burden of Disease Study 2010 [published
correction appears in Lancet. 2014;383(9913):218.]. 9. Arima H, Chalmers J, Woodward M, et al; 16. Salam A, Atkins E, Sundström J, et al; Blood
Lancet. 2014;383(9913):245-254. doi:10.1016/S0140- PROGRESS Collaborative Group. Lower target Pressure Lowering Treatment Trialists’
6736(13)61953-4 blood pressures are safe and effective for the Collaboration. Effects of blood pressure lowering
prevention of recurrent stroke: the PROGRESS trial. on cardiovascular events, in the context of
2. Staessen JA, Wang JG, Thijs L. Cardiovascular J Hypertens. 2006;24(6):1201-1208. doi:10.1097/01. regression to the mean: a systematic review of
protection and blood pressure reduction: hjh.0000226212.34055.86 randomized trials. J Hypertens. 2019;37(1):16-23.
a meta-analysis. Lancet. 2001;358(9290):1305-1315. doi:10.1097/HJH.0000000000001994
doi:10.1016/S0140-6736(01)06411-X 10. Benavente OR, Coffey CS, Conwit R, et al; SPS3
Study Group. Blood-pressure targets in patients 17. Zanchetti A, Liu L, Mancia G, et al. Blood
3. Gueyffier F, Boissel JP, Boutitie F, et al; INDANA with recent lacunar stroke: the SPS3 randomised pressure and LDL-cholesterol targets for prevention
(Individual Data Analysis of Antihypertensive trial. Lancet. 2013;382(9891):507-515. doi:10.1016/ of recurrent strokes and cognitive decline in the
Intervention Trials) Project Collaborators. Effect of S0140-6736(13)60852-1 hypertensive patient: design of the European
antihypertensive treatment in patients having Society of Hypertension–Chinese Hypertension
already suffered from stroke: gathering the 11. Wright JT Jr, Williamson JD, Whelton PK, et al;
SPRINT Research Group. A randomized trial of League Stroke in Hypertension Optimal Treatment
evidence. Stroke. 1997;28(12):2557-2562. doi:10. randomized trial. J Hypertens. 2014;32(9):1888-1897.
1161/01.STR.28.12.2557 intensive versus standard blood-pressure control
[published correction appears at N Engl J Med. doi:10.1097/HJH.0000000000000254
4. PROGRESS Collaborative Group. Randomised 2017;377(25):2506]. N Engl J Med. 2015;373(22): 18. Lawes CM, Rodgers A, Bennett DA, et al; Asia
trial of a perindopril-based blood-pressure– 2103-2116. Pacific Cohort Studies Collaboration. Blood
lowering regimen among 6,105 individuals with pressure and cardiovascular disease in the Asia
previous stroke or transient ischaemic attack. Lancet. 12. Zonneveld TP, Richard E, Vergouwen MD, et al.
Blood pressure–lowering treatment for preventing Pacific region. J Hypertens. 2003;21(4):707-716.
2001;358(9287):1033-1041. doi:10.1016/S0140-6736 doi:10.1097/00004872-200304000-00013
(01)06178-5 recurrent stroke, major vascular events, and
dementia in patients with a history of stroke or 19. Shimamoto K, Ando K, Fujita T, et al; Japanese
5. Liu L, Wang Z, Gong L, et al. Blood pressure transient ischaemic attack. Cochrane Database Syst Society of Hypertension Committee for Guidelines
reduction for the secondary prevention of stroke: Rev. 2018;7:CD007858. doi:10.1002/14651858. for the Management of Hypertension. The
a Chinese trial and a systematic review of the CD007858.pub2 Japanese Society of Hypertension guidelines for
literature. Hypertens Res. 2009;32(11):1032-1040. the management of hypertension (JSH 2014).
doi:10.1038/hr.2009.139 13. Mant J, McManus RJ, Roalfe A, et al. Different
systolic blood pressure targets for people with Hypertens Res. 2014;37(4):253-390. doi:10.1038/
6. Rashid P, Leonardi-Bee J, Bath P. Blood pressure history of stroke or transient ischaemic attack: hr.2014.20
reduction and secondary prevention of stroke and
E10 JAMA Neurology Published online July 29, 2019 (Reprinted) jamaneurology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Dalhousie University User on 08/03/2019
You might also like
- Nuirsing Care Plan For HypertensionDocument8 pagesNuirsing Care Plan For HypertensionJowzef92% (24)
- Acute Stroke Management in the Era of ThrombectomyFrom EverandAcute Stroke Management in the Era of ThrombectomyEdgar A. SamaniegoNo ratings yet
- TASK 3 LEC CU9 (ZOMIL, Geralyn Kae M.)Document3 pagesTASK 3 LEC CU9 (ZOMIL, Geralyn Kae M.)Geralyn Kae100% (1)
- WHO Midwife Training ManualDocument139 pagesWHO Midwife Training ManualGleepeep Goobledegook100% (2)
- Kitagawa 2019Document10 pagesKitagawa 2019chriz murtNo ratings yet
- Aspirin Plus Clopidogrel As Secondary Prevention After Stroke or Transient Ischemic Attack: A Systematic Review and Meta-AnalysisDocument13 pagesAspirin Plus Clopidogrel As Secondary Prevention After Stroke or Transient Ischemic Attack: A Systematic Review and Meta-Analysisnandy surya kusumaNo ratings yet
- Case Meta AnalysisDocument10 pagesCase Meta AnalysisTutik RahayuNo ratings yet
- Aspirin Plus Clopidogrel As Secondary Prevention After Stroke or Transient Ischemic Attack: A Systematic Review and Meta-AnalysisDocument13 pagesAspirin Plus Clopidogrel As Secondary Prevention After Stroke or Transient Ischemic Attack: A Systematic Review and Meta-AnalysisshevmyrNo ratings yet
- Jurnal 1Document8 pagesJurnal 1sweetcloversNo ratings yet
- Aha 4Document11 pagesAha 4Yunika KhairinaNo ratings yet
- cilostazol timingDocument11 pagescilostazol timingesdras pramuditaNo ratings yet
- Packer 2019Document14 pagesPacker 2019Renata D GNo ratings yet
- Su 2015Document7 pagesSu 2015carolin enjelin rumaikewiNo ratings yet
- Document PDFDocument12 pagesDocument PDFnikenauliaputriNo ratings yet
- 397 671 1 SMDocument7 pages397 671 1 SMbobirfansyahputraNo ratings yet
- Benefit and Risks of Clopidogrel Vs Aspirin Monotherapy After Recent Ischemic StrokDocument13 pagesBenefit and Risks of Clopidogrel Vs Aspirin Monotherapy After Recent Ischemic StrokRichardNo ratings yet
- Fphar 11 00729Document8 pagesFphar 11 00729AmalNo ratings yet
- Johnston 2018Document23 pagesJohnston 2018cru1s3rNo ratings yet
- CABANADocument14 pagesCABANAIsmael Rivera DiazNo ratings yet
- Gouya 2013Document21 pagesGouya 2013Luthfi DziyaNo ratings yet
- STR 0000000000000377Document12 pagesSTR 0000000000000377MikeNo ratings yet
- Aspirin and Aspilet Compared PDFDocument18 pagesAspirin and Aspilet Compared PDFEfrianti Viorenta HutapeaNo ratings yet
- Jamainternal Brunstrm 2017 Oi 170103Document9 pagesJamainternal Brunstrm 2017 Oi 170103frandi wirajayaNo ratings yet
- Afire Articulo OriginalDocument11 pagesAfire Articulo OriginalElvira AnitaNo ratings yet
- Jurnal Aspirin Vs Klopidogrel Meta AnalysisDocument12 pagesJurnal Aspirin Vs Klopidogrel Meta AnalysisBantuinAku KakNo ratings yet
- Myocard InfarctionDocument10 pagesMyocard InfarctionFelicia HoseaNo ratings yet
- Association Between Magnitude of Differential Blood Pressure Reduction and Secondary Stroke Prevention A Meta-Analysis and Meta-RegressionDocument10 pagesAssociation Between Magnitude of Differential Blood Pressure Reduction and Secondary Stroke Prevention A Meta-Analysis and Meta-RegressionNeurología SinuanosNo ratings yet
- 4 PDFDocument9 pages4 PDFKhairinnisaNo ratings yet
- Dual Antiplatelet Therapy Using Cilostazol For SecondaryDocument10 pagesDual Antiplatelet Therapy Using Cilostazol For SecondarySyed Shabbir HaiderNo ratings yet
- Brain-X - 2023 - Li - Heart Brain Team Approach of Acute Myocardial Infarction Complicating Acute Stroke Evidencing TheDocument2 pagesBrain-X - 2023 - Li - Heart Brain Team Approach of Acute Myocardial Infarction Complicating Acute Stroke Evidencing TheBlackswannnNo ratings yet
- Effectiveness of Combined Regional General Anesth 2016 Brazilian Journal ofDocument11 pagesEffectiveness of Combined Regional General Anesth 2016 Brazilian Journal ofNguyễn Thị Mai XuânNo ratings yet
- Race Ii 2010 NejmDocument11 pagesRace Ii 2010 NejmAxel Hiram Hernandez PinedaNo ratings yet
- FKTR FixDocument3 pagesFKTR FixvinaNo ratings yet
- Control of Blood Pressure and Risk of Mortality in Older AdultsDocument8 pagesControl of Blood Pressure and Risk of Mortality in Older AdultsYakelin VillanuevaNo ratings yet
- Safety and Efficacy of Intensive Vs Guideline Antiplatelet Thera 2015Document7 pagesSafety and Efficacy of Intensive Vs Guideline Antiplatelet Thera 2015AnDreARNo ratings yet
- Ziff 2018Document9 pagesZiff 2018gabbynengNo ratings yet
- Strokeaha 120 033033Document7 pagesStrokeaha 120 033033MarisolCamposNo ratings yet
- Effects of Intensive Systolic Blood Pressure Control On Kidney and Cardiovascular Outcomes in Persons Without Kidney DiseaseDocument20 pagesEffects of Intensive Systolic Blood Pressure Control On Kidney and Cardiovascular Outcomes in Persons Without Kidney DiseaseRoberto López MataNo ratings yet
- Journal 4 - Management of Traumatic Brain Injury A Narrative Review of Current EvidenceDocument11 pagesJournal 4 - Management of Traumatic Brain Injury A Narrative Review of Current EvidenceNatalindah Jokiem Woecandra T. D.No ratings yet
- MatcH 2004Document7 pagesMatcH 2004Pedro Garcia CervantesNo ratings yet
- High Dose Vs Low Dose Statin in MaceDocument9 pagesHigh Dose Vs Low Dose Statin in MaceErvan ZuhriNo ratings yet
- Joa3 12534Document7 pagesJoa3 12534chasia chaselNo ratings yet
- 1 s2.0 S0914508719301765 MainDocument8 pages1 s2.0 S0914508719301765 MainAdriani HartantoNo ratings yet
- Restart Collaboration - Effects of Antiplatelet Therapy After Stroke Due To Intracerebral Haemorrhage (RESTART) - OriginalDocument11 pagesRestart Collaboration - Effects of Antiplatelet Therapy After Stroke Due To Intracerebral Haemorrhage (RESTART) - OriginalPhaimNo ratings yet
- Standardized Team-Based Care For Cardiogenic Shock: BackgroundDocument11 pagesStandardized Team-Based Care For Cardiogenic Shock: BackgroundLucas MatheusNo ratings yet
- Standard Blood-Pressure ControlDocument14 pagesStandard Blood-Pressure ControljaimeNo ratings yet
- Ticagrelor Versus Aspirin in Acute Stroke or Transient Ischemic AttackDocument9 pagesTicagrelor Versus Aspirin in Acute Stroke or Transient Ischemic AttackTara WandhitaNo ratings yet
- Effect of Lowering VT On Mortality in Acute Respiratory DistressDocument8 pagesEffect of Lowering VT On Mortality in Acute Respiratory DistressFabio RepettoNo ratings yet
- 1 Running Head: Preventing Recurrent Myocardial InfarctionsDocument10 pages1 Running Head: Preventing Recurrent Myocardial InfarctionsIsaacNo ratings yet
- Antihypertensive Use For Stroke in United States Emergency DepartmentsDocument5 pagesAntihypertensive Use For Stroke in United States Emergency DepartmentsIsrael Velástegui VillaNo ratings yet
- Strokeaha 120 033033Document7 pagesStrokeaha 120 033033AudryaNo ratings yet
- (19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeDocument7 pages(19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeRandy Reina RiveroNo ratings yet
- Xu 2006Document5 pagesXu 2006Elvan WiyartaNo ratings yet
- Joi 130108Document11 pagesJoi 130108Ami PuspitasariNo ratings yet
- New England Journal Medicine: The ofDocument14 pagesNew England Journal Medicine: The ofAndrew NdewNo ratings yet
- 10 1001@jama 2020 0930Document12 pages10 1001@jama 2020 0930Dobson Flores AparicioNo ratings yet
- EBioMedicine 2015 p1071Document8 pagesEBioMedicine 2015 p1071Chintya Anugrah SuhendraNo ratings yet
- 3.6 Meta-Analysis - Anticoagulant Prophylaxis To Prevent Symptomatic Venous Thromboembolism in Hospitalized Medical PatientsDocument13 pages3.6 Meta-Analysis - Anticoagulant Prophylaxis To Prevent Symptomatic Venous Thromboembolism in Hospitalized Medical PatientsMikeyNo ratings yet
- ehae151Document11 pagesehae151lakshminivas PingaliNo ratings yet
- NephrologyDocument10 pagesNephrologyDesi HutapeaNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofAlina PirtacNo ratings yet
- Charisma TrialDocument10 pagesCharisma TrialYahya AlmalkiNo ratings yet
- Jurnal KMB Diva - 015Document10 pagesJurnal KMB Diva - 015Setiaty PandiaNo ratings yet
- Arborizing Vessels On Dermoscopy in Various Skin Diseases Other Than Basal Cell CarcinomaDocument7 pagesArborizing Vessels On Dermoscopy in Various Skin Diseases Other Than Basal Cell CarcinomasaosaharaNo ratings yet
- 12482-Article Text-44305-1-10-20150624Document5 pages12482-Article Text-44305-1-10-20150624saosaharaNo ratings yet
- Jurding 2Document6 pagesJurding 2saosaharaNo ratings yet
- Jurding 3Document8 pagesJurding 3saosaharaNo ratings yet
- Jurnal KustaDocument11 pagesJurnal KustasaosaharaNo ratings yet
- Vancouver Referencing Style GuideDocument12 pagesVancouver Referencing Style GuideAndre PrayogoNo ratings yet
- Jurnaal PDFDocument4 pagesJurnaal PDFsaosaharaNo ratings yet
- Journal of Advanced Research Review of the Complex Relationship Between Vitamin D and the SkinDocument12 pagesJournal of Advanced Research Review of the Complex Relationship Between Vitamin D and the SkindayangNo ratings yet
- STD Treatment 2015Document140 pagesSTD Treatment 2015Supalerk KowinthanaphatNo ratings yet
- Nummular eczema of the breast after cancer surgeryDocument4 pagesNummular eczema of the breast after cancer surgerysaosaharaNo ratings yet
- IndianJDermatopatholDiagnDermatol4241-3A502823 094348Document11 pagesIndianJDermatopatholDiagnDermatol4241-3A502823 094348saosaharaNo ratings yet
- Jurnal KustaDocument11 pagesJurnal KustasaosaharaNo ratings yet
- Nummular eczema of the breast after cancer surgeryDocument4 pagesNummular eczema of the breast after cancer surgerysaosaharaNo ratings yet
- Arborizing Vessels On Dermoscopy in Various Skin Diseases Other Than Basal Cell CarcinomaDocument7 pagesArborizing Vessels On Dermoscopy in Various Skin Diseases Other Than Basal Cell CarcinomasaosaharaNo ratings yet
- 17Document4 pages17cut nondaNo ratings yet
- Assessment and Initial ManagemDocument14 pagesAssessment and Initial ManagemsaosaharaNo ratings yet
- Assessment and Initial ManagemDocument14 pagesAssessment and Initial ManagemsaosaharaNo ratings yet
- Assessment and Initial ManagemDocument14 pagesAssessment and Initial ManagemsaosaharaNo ratings yet
- Amlodipine ReadingDocument12 pagesAmlodipine Readingines pachecoNo ratings yet
- 2003 World Health Organization (WHO) /international Society of Hypertension (ISH) Statement On Management of HypertensionDocument10 pages2003 World Health Organization (WHO) /international Society of Hypertension (ISH) Statement On Management of HypertensionGhina NisrinaNo ratings yet
- Jelita Woman PKMDocument6 pagesJelita Woman PKMIrma Qirani MuhsenNo ratings yet
- Management of Preeclampsia, Severe Preeclampsia, and Eclampsia at Primary Care Facilities in BangladeshDocument12 pagesManagement of Preeclampsia, Severe Preeclampsia, and Eclampsia at Primary Care Facilities in BangladeshUmi Nur JannahNo ratings yet
- G.R. No. 187950 CRISTINA BARSOLO, Petitioner, Social Security System, Respondent. Decision Leonen, J.Document25 pagesG.R. No. 187950 CRISTINA BARSOLO, Petitioner, Social Security System, Respondent. Decision Leonen, J.Moachi SianenNo ratings yet
- Omron M6Document26 pagesOmron M6paninaro2011No ratings yet
- ATI Heart PPT - Chapter - 20Document40 pagesATI Heart PPT - Chapter - 20sutopianoNo ratings yet
- PBL 2 - StrokeDocument14 pagesPBL 2 - StrokeKong Pei IngNo ratings yet
- 2022 Labor Jurisprudence - LLR ClassDocument97 pages2022 Labor Jurisprudence - LLR Classzonix lomboyNo ratings yet
- 24-Hour BP Control with Triple Therapy"The title "TITLE 24-Hour BP Control with Triple TherapyDocument10 pages24-Hour BP Control with Triple Therapy"The title "TITLE 24-Hour BP Control with Triple TherapyAnggun Nurul FitriaNo ratings yet
- DNB CET REVIEW 3RD EDITION ERRATA REPORTDocument30 pagesDNB CET REVIEW 3RD EDITION ERRATA REPORTAjayModgil100% (1)
- Hypertension Infographic 005 WebDocument2 pagesHypertension Infographic 005 WebNailahRahmahNo ratings yet
- Ajay Bhalla, Jonathan Birns (Eds.) - Management of Post-Stroke Complications-Springer International Publishing (2015) PDFDocument393 pagesAjay Bhalla, Jonathan Birns (Eds.) - Management of Post-Stroke Complications-Springer International Publishing (2015) PDFAchmad FachryNo ratings yet
- Hipertensi: Winny Mutia FranciskaDocument4 pagesHipertensi: Winny Mutia FranciskaFranciska MuthiaNo ratings yet
- MCN Exam Gestational ConditionsDocument9 pagesMCN Exam Gestational ConditionsEdith Cabrera Cabigas - SabalboroNo ratings yet
- Review of Literature: (Bharucha and Kuruvilla, 2003)Document11 pagesReview of Literature: (Bharucha and Kuruvilla, 2003)jainslotusNo ratings yet
- Vox Sanguin Feb 16Document102 pagesVox Sanguin Feb 16rsdarsono labNo ratings yet
- Jurnal Observasional AnalitikDocument9 pagesJurnal Observasional AnalitikJethro BudimanNo ratings yet
- Clinical Case 1 - PGI MendezDocument2 pagesClinical Case 1 - PGI MendezJoher MendezNo ratings yet
- ClinicosocialcaseHypertensionDr DeepanshiDocument85 pagesClinicosocialcaseHypertensionDr DeepanshiAmit BondNo ratings yet
- Common Cardiac MedicationsDocument1 pageCommon Cardiac MedicationsPaige HardekopfNo ratings yet
- PIH Renal Doppler Pregnancy - CutDocument4 pagesPIH Renal Doppler Pregnancy - CutAnonymous 9QxPDpNo ratings yet
- Bescos (2020), Effects of Chlorhexidine Mouthwash On The Oral MicrobiomeDocument8 pagesBescos (2020), Effects of Chlorhexidine Mouthwash On The Oral MicrobiomePhuong ThaoNo ratings yet
- And Its: Dr. V.PushkarDocument92 pagesAnd Its: Dr. V.PushkarMudit MisraNo ratings yet
- CVD Risk Factors ExplainedDocument18 pagesCVD Risk Factors ExplainedShin QuinnNo ratings yet
- Gestational HypertensionDocument2 pagesGestational HypertensionReyniel Pablo ElumbaNo ratings yet
- Drugs Used For Treatment of Hypertension: 4/6/2023 DBU, Pharmacology 1Document113 pagesDrugs Used For Treatment of Hypertension: 4/6/2023 DBU, Pharmacology 1BeimnetNo ratings yet