You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Infinite CoinsDocument1 pageInfinite CoinsJames NorldNo ratings yet
- PricelistDocument14 pagesPricelistJames NorldNo ratings yet
- E4881 en USDocument9 pagesE4881 en USJames NorldNo ratings yet
- Lumit® Anti-Tag Protein Interaction Reagents - Tagged Protein InteractionsDocument6 pagesLumit® Anti-Tag Protein Interaction Reagents - Tagged Protein InteractionsJames NorldNo ratings yet
- Cases For Clinical Skills in USMLE 2 - 1Document84 pagesCases For Clinical Skills in USMLE 2 - 1James NorldNo ratings yet
- V6961 en USDocument38 pagesV6961 en USJames NorldNo ratings yet
- E4881 en USDocument9 pagesE4881 en USJames NorldNo ratings yet
- Unlabelled and Mislabelled SpecimensDocument2 pagesUnlabelled and Mislabelled SpecimensJames NorldNo ratings yet
- Blood Brochure International - 210528Document4 pagesBlood Brochure International - 210528James NorldNo ratings yet
- Krause - World Coins Catalog 1701-1800 IndexDocument16 pagesKrause - World Coins Catalog 1701-1800 IndexJames Norld0% (1)
- Uganda Banana Tissue CultureDocument2 pagesUganda Banana Tissue CultureJames NorldNo ratings yet
- Fainting: Signs and Symptoms of FaintingDocument1 pageFainting: Signs and Symptoms of FaintingJames NorldNo ratings yet
- My Research ArticleDocument7 pagesMy Research ArticleclimedNo ratings yet
- PCT For BodybuildersDocument12 pagesPCT For BodybuildersJon Mester100% (4)
- Innovation in Higher Education (Pak Amirullah)Document7 pagesInnovation in Higher Education (Pak Amirullah)Elsa AmeliaNo ratings yet
- Department of Education Schools Division of Toledo City Malubog Elementary SchoolDocument6 pagesDepartment of Education Schools Division of Toledo City Malubog Elementary SchoolTintin Cadorna FielNo ratings yet
- 5 Ways To Focus at Work, From An Executive Who's Struggled With ADHDDocument5 pages5 Ways To Focus at Work, From An Executive Who's Struggled With ADHDtinaNo ratings yet
- THERAP COMM QuizletDocument28 pagesTHERAP COMM QuizletMary Margareth GonzalesNo ratings yet
- Health - Fontanilla, LyndoDocument4 pagesHealth - Fontanilla, LyndoArvin R. VillanuevaNo ratings yet
- Contoh Review GarciniaDocument8 pagesContoh Review GarciniamarwahNo ratings yet
- MSDS Hydrol HLPD 22 32 46 68 2008 enDocument6 pagesMSDS Hydrol HLPD 22 32 46 68 2008 enDaniel DaiaNo ratings yet
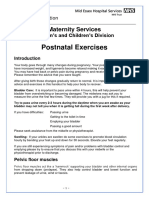
- MEHT130379 Postnatal Exercises 2.0Document7 pagesMEHT130379 Postnatal Exercises 2.0rachellycNo ratings yet
- 2021 Anthropometry Procedures Manual 508Document91 pages2021 Anthropometry Procedures Manual 508Diogo JuniorNo ratings yet
- Residential Fire Protection ProposalDocument24 pagesResidential Fire Protection ProposalAidan YepsonNo ratings yet
- Gerontologic Nursing 10Document10 pagesGerontologic Nursing 10Sherrylyne Anne De Francia - OrdanzaNo ratings yet
- UPSC Monthly Current Affairs Dec 2019 PDFDocument143 pagesUPSC Monthly Current Affairs Dec 2019 PDFBhargav KNo ratings yet
- Health Economics 1st Edition Bhattacharya Solutions ManualDocument24 pagesHealth Economics 1st Edition Bhattacharya Solutions ManualZacharyPrinceyasp100% (38)
- Neuromuscular DiseasesDocument205 pagesNeuromuscular DiseasesvivicouNo ratings yet
- Spirituality, Spiritual Well-Being, and Spiritual Coping in Advanced Heart FailureDocument18 pagesSpirituality, Spiritual Well-Being, and Spiritual Coping in Advanced Heart FailurezakiaNo ratings yet
- Body Temperature: Physiology DepartmentDocument17 pagesBody Temperature: Physiology DepartmentMaab AlrsheedNo ratings yet
- Cultural Humility in Psychotherapy SupervisionDocument19 pagesCultural Humility in Psychotherapy SupervisionMilo DueNo ratings yet
- Reviewer in P.E. 11Document25 pagesReviewer in P.E. 11Joel BrionesNo ratings yet
- The Analysis of Character Behaviors in "Yellow Wallpaper" by Charlotte Perkins Gilman and Its Relevance To The Current IssuesDocument6 pagesThe Analysis of Character Behaviors in "Yellow Wallpaper" by Charlotte Perkins Gilman and Its Relevance To The Current IssuesFadlilah RahmawatiNo ratings yet
- Course Syllabus - Hematology 2Document2 pagesCourse Syllabus - Hematology 2Fearless AngelNo ratings yet
- F 01 01 02 A FORM PENDAFTARAN Rev 28-20 TRAINING IKBAL IKBAL-M-YOSDocument2 pagesF 01 01 02 A FORM PENDAFTARAN Rev 28-20 TRAINING IKBAL IKBAL-M-YOSjerrysibaoadiNo ratings yet
- Community Health Planning, Implementation, and EvaluationDocument9 pagesCommunity Health Planning, Implementation, and EvaluationKarl Angelo MontanoNo ratings yet
- Formulating A Nursing Care Plan: S++aint Paul University PhilippinesDocument7 pagesFormulating A Nursing Care Plan: S++aint Paul University Philippinesninafatima allamNo ratings yet
- Fruit PP-1Document13 pagesFruit PP-1RedwanNo ratings yet
- TOACS OSCE Exam For IMM & Part IIDocument71 pagesTOACS OSCE Exam For IMM & Part IIFurqan MirzaNo ratings yet
- Mechaala 2021Document13 pagesMechaala 2021Evelin YanaNo ratings yet
- Mosquito Repellent Property of Ylang YlangDocument9 pagesMosquito Repellent Property of Ylang YlangR RenegadeNo ratings yet
- Practice Lw-03: Questions 1-5 Choose The Correct Letter, A, B or CDocument6 pagesPractice Lw-03: Questions 1-5 Choose The Correct Letter, A, B or CViet HoangNo ratings yet