You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 60 Item Medical Surgical Nursing Musculoskeletal Examination AnswersDocument11 pages60 Item Medical Surgical Nursing Musculoskeletal Examination AnswersLj Ferolino94% (48)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tetanus and Rabies FinalDocument23 pagesTetanus and Rabies FinalnavenNo ratings yet
- Muscular FitnessDocument44 pagesMuscular FitnessJack Messaros100% (1)
- Concussion To Consequence - Managing Sport-Related Concussion On & Off The FieldDocument63 pagesConcussion To Consequence - Managing Sport-Related Concussion On & Off The FieldSNo ratings yet
- ACL and PCL ReconstructionDocument25 pagesACL and PCL ReconstructionAli Aufar Hutasuhut100% (1)
- CASE STUDY PATHFIT Gregorio Prianes Sandhu CabayacruzDocument45 pagesCASE STUDY PATHFIT Gregorio Prianes Sandhu CabayacruzNoldan King FranciscoNo ratings yet
- ETT IntubationDocument10 pagesETT IntubationPoova RagavanNo ratings yet
- Learner'S Packet No. 5 Quarter 1: Identify Hazards and RisksDocument5 pagesLearner'S Packet No. 5 Quarter 1: Identify Hazards and Risksanna balmesNo ratings yet
- 11 (B) - Neurological AssessmentDocument63 pages11 (B) - Neurological AssessmentNabil KhanNo ratings yet
- CCCABI ChecklistDocument2 pagesCCCABI ChecklistLucy WhiteheadNo ratings yet
- Changes in Musculoskeletal System During AgingDocument19 pagesChanges in Musculoskeletal System During Agingsonali tushamerNo ratings yet
- Neuroanatomy L2 (ANS)Document11 pagesNeuroanatomy L2 (ANS)Charlize MarthaNo ratings yet
- Trusted Medical Answers-In Seconds.: Chest PainDocument22 pagesTrusted Medical Answers-In Seconds.: Chest PainntnquynhproNo ratings yet
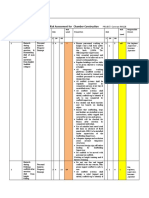
- Risk Assesment For Chamber ConstructionDocument5 pagesRisk Assesment For Chamber ConstructionSasi KumarNo ratings yet
- Back SafetyDocument27 pagesBack SafetyJoel TendoNo ratings yet
- Final Project 2020-21Document50 pagesFinal Project 2020-21Rs 31 Pavan PawarNo ratings yet
- TOTAPSDocument14 pagesTOTAPSHANIFF FAIZAL BIN CHEK ANI CHEK ANI IPG KDANo ratings yet
- 2 Female Pelvis and Foetal SkullDocument17 pages2 Female Pelvis and Foetal SkullMalak Ahmed 2295No ratings yet
- Japanese Silk Love RopeDocument9 pagesJapanese Silk Love RopePedro AraujoNo ratings yet
- Forensic PathologyDocument83 pagesForensic PathologyElisa RoyNo ratings yet
- Shoe and Foot OrthosisDocument9 pagesShoe and Foot Orthosis楊畯凱No ratings yet
- Criminal Law Ii Notes: Non-Fatal Offences Affecting Human BodyDocument43 pagesCriminal Law Ii Notes: Non-Fatal Offences Affecting Human BodyWai LingNo ratings yet
- Guideline and Treatment Algorithm For Burn InjuriesDocument12 pagesGuideline and Treatment Algorithm For Burn InjuriesGrnitrv 22No ratings yet
- Abaqus BioRID-II Crash Dummy ModelDocument7 pagesAbaqus BioRID-II Crash Dummy ModelAlex CarhatNo ratings yet
- Return Demo Level 4Document16 pagesReturn Demo Level 4Denese JocsonNo ratings yet
- Lesson Exemplar Health 4thDocument4 pagesLesson Exemplar Health 4thelmalynNo ratings yet
- Emergency Radiology The Requisites Second Edition Edition Lucey Full ChapterDocument67 pagesEmergency Radiology The Requisites Second Edition Edition Lucey Full Chaptergina.larson159100% (8)
- Clinical GoalsDocument13 pagesClinical GoalsHycient PaulNo ratings yet
- Clinical Staging and Management of Pressure-Induced Skin and Soft Tissue Injury - UpToDateDocument31 pagesClinical Staging and Management of Pressure-Induced Skin and Soft Tissue Injury - UpToDatePriscillaNo ratings yet
- Triple Artrodesis TobilloDocument17 pagesTriple Artrodesis TobilloIsrael CucsNo ratings yet