You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tissue Ablation and Gas Formation of Two Excimer Laser Systems - An in Vitro Evaluation On Porcine AortaDocument9 pagesTissue Ablation and Gas Formation of Two Excimer Laser Systems - An in Vitro Evaluation On Porcine AortaMarco Antonio Miranda RodriguezNo ratings yet
- Toyota Camry 2002 2006 Workshop ManualDocument20 pagesToyota Camry 2002 2006 Workshop Manualbelinda100% (47)
- The Bedrock Principles: DisciplineDocument9 pagesThe Bedrock Principles: Disciplinekriki_mNo ratings yet
- 24 MountainsDocument3 pages24 MountainsDaniela DanaNo ratings yet
- Ansari, Abid A. - Gill, Sarvajeet Singh - Naeem, M-Essential Plant Nutrients - Uptake, Use Efficiency, and Management-Springer International Publishing (2017) PDFDocument571 pagesAnsari, Abid A. - Gill, Sarvajeet Singh - Naeem, M-Essential Plant Nutrients - Uptake, Use Efficiency, and Management-Springer International Publishing (2017) PDFluisNo ratings yet
- Molar Uprighting / Orthodontic Courses by Indian Dental AcademyDocument142 pagesMolar Uprighting / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Creation Stories: in The BeginningDocument6 pagesCreation Stories: in The BeginningJackie LooNo ratings yet
- IT Companies in CoimbatoreDocument1 pageIT Companies in Coimbatoresureshkumarmask60% (5)
- Dyeing Defects and Their RemediesDocument5 pagesDyeing Defects and Their RemediesMuhammad ImranNo ratings yet
- Laser and Light Sources For Removal of Unwanted HairDocument11 pagesLaser and Light Sources For Removal of Unwanted HairSuhair F Diebes100% (1)
- Theories, Models and Approaches Applied To Midwifery PracticesDocument111 pagesTheories, Models and Approaches Applied To Midwifery Practicesdr.anu Rk90% (10)
- Numerical Modelling of Methane Gas Migration in Dry Coal SeamsDocument23 pagesNumerical Modelling of Methane Gas Migration in Dry Coal SeamsMarco Antonio Miranda RodriguezNo ratings yet
- Liquid and Gas Chromatographic Multi-Residue Pesticide Determination in Animal TissuesDocument9 pagesLiquid and Gas Chromatographic Multi-Residue Pesticide Determination in Animal TissuesMarco Antonio Miranda RodriguezNo ratings yet
- Application of Lattice Gas Techniques To The Study of Sediment Erosion and Transport Caused by Laminar SheetflowDocument9 pagesApplication of Lattice Gas Techniques To The Study of Sediment Erosion and Transport Caused by Laminar SheetflowMarco Antonio Miranda RodriguezNo ratings yet
- Stress-Strain Analysis in Productive Gas - Oil ReservoirsDocument25 pagesStress-Strain Analysis in Productive Gas - Oil ReservoirsMarco Antonio Miranda RodriguezNo ratings yet
- Bond Graph Modelling and Simulation PhotovoltaicDocument12 pagesBond Graph Modelling and Simulation PhotovoltaicMarco Antonio Miranda RodriguezNo ratings yet
- Transient Simulation of Conventional Hybrid PhotovoltaicDocument16 pagesTransient Simulation of Conventional Hybrid PhotovoltaicMarco Antonio Miranda RodriguezNo ratings yet
- Marine Battery Training Guide: How To Select, Install and Maintain A Marine BatteryDocument8 pagesMarine Battery Training Guide: How To Select, Install and Maintain A Marine BatteryMarco Antonio Miranda RodriguezNo ratings yet
- Electrical Characterization Testing of Sealed Nickel-Zinc BatteriesDocument6 pagesElectrical Characterization Testing of Sealed Nickel-Zinc BatteriesMarco Antonio Miranda RodriguezNo ratings yet
- Life-Cycle Analysis of Flow-Assisted Nickel Zinc-,manganeseDocument17 pagesLife-Cycle Analysis of Flow-Assisted Nickel Zinc-,manganeseMarco Antonio Miranda RodriguezNo ratings yet
- Nickel - Zinc BatteriesDocument8 pagesNickel - Zinc BatteriesMarco Antonio Miranda RodriguezNo ratings yet
- Nickel-Zinc Accordion-Fold Batteries With MicrofibrousDocument14 pagesNickel-Zinc Accordion-Fold Batteries With MicrofibrousMarco Antonio Miranda RodriguezNo ratings yet
- Zinc-Nickel Single Flow Batteries With Improved Cycling StabilityDocument7 pagesZinc-Nickel Single Flow Batteries With Improved Cycling StabilityMarco Antonio Miranda RodriguezNo ratings yet
- Characterization of Evertroll Nickel-Zinc BatteriesDocument7 pagesCharacterization of Evertroll Nickel-Zinc BatteriesMarco Antonio Miranda RodriguezNo ratings yet
- Zinc Morphology in Zinc-Nickel Flow BatteryDocument6 pagesZinc Morphology in Zinc-Nickel Flow BatteryMarco Antonio Miranda RodriguezNo ratings yet
- Lead Ion and Tetrabutylammonium Bromide As Inhibitors of The Growth of Spongy PDFDocument5 pagesLead Ion and Tetrabutylammonium Bromide As Inhibitors of The Growth of Spongy PDFMarco Antonio Miranda RodriguezNo ratings yet
- Water MetersDocument3 pagesWater MetersRashedNo ratings yet
- 2021 MSF2021 PM MG Precon3dDocument4 pages2021 MSF2021 PM MG Precon3dPavao MarovicNo ratings yet
- Double FertilizationDocument2 pagesDouble FertilizationDNeye1940No ratings yet
- Analog Circuits II Lab ManualDocument47 pagesAnalog Circuits II Lab ManualParesh SawantNo ratings yet
- Jenbacher: 1. General: - 1Document5 pagesJenbacher: 1. General: - 1ArîfNo ratings yet
- AESV Catalogue Final PDFDocument32 pagesAESV Catalogue Final PDFSuvek KumarNo ratings yet
- Grundig BL 6280 Bl6280 LeafletDocument1 pageGrundig BL 6280 Bl6280 Leafletmrsiiiiiiii xetNo ratings yet
- Geno CapitoniDocument18 pagesGeno CapitoniolguinrfNo ratings yet
- Delta Airlines and SummaryDocument39 pagesDelta Airlines and Summaryeissa alesayiNo ratings yet
- Tier1-Cvs, Cns and Respiratory Safety Pharmacology, Herg Assay Tier2-Gi, Renal and Other StudiesDocument30 pagesTier1-Cvs, Cns and Respiratory Safety Pharmacology, Herg Assay Tier2-Gi, Renal and Other StudiesCHETHAN K SNo ratings yet
- RTN 380 V100R002C00 Commissioning and Configuration Guide 03Document308 pagesRTN 380 V100R002C00 Commissioning and Configuration Guide 03Lubo PicturesMaker100% (5)
- RidgeBot - AI Driven Pen TestDocument1 pageRidgeBot - AI Driven Pen TestMuhammed Asif ShaikhNo ratings yet
- Chapter 3 Cassava Taro Group 2Document8 pagesChapter 3 Cassava Taro Group 2jadeshades12No ratings yet
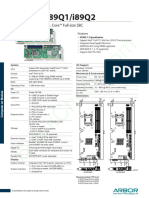
- Arbor Hicore I89q1 I89q2Document2 pagesArbor Hicore I89q1 I89q2Waleed MareeNo ratings yet
- CLE7 ThirdQuarter Module1Document10 pagesCLE7 ThirdQuarter Module1Roella Mae Tudias AlodNo ratings yet
- BMT300 User Manual 0J PP130409-Revised01MayECDocument41 pagesBMT300 User Manual 0J PP130409-Revised01MayECreza515heiNo ratings yet
- Vaccine: by DR Balaram SahuDocument27 pagesVaccine: by DR Balaram SahuPratap Chandra BeheraNo ratings yet
- CN PresentationDocument24 pagesCN PresentationMd AshikNo ratings yet
- Hindi NounsDocument1 pageHindi NounsvenkatsowmiNo ratings yet
- For Your Information Its MaggiDocument12 pagesFor Your Information Its MaggiSheetal SainiNo ratings yet