You might also like
- Vatachart Back BW FinalDocument1 pageVatachart Back BW FinalAnand YadavNo ratings yet
- Ayurveda and Psychiatry: Everything That Exists Is A Mirage of The MindDocument44 pagesAyurveda and Psychiatry: Everything That Exists Is A Mirage of The MindAnand YadavNo ratings yet
- Ayurved Vyaspeeth Dainandini 2022 List of Coordinators For Maharashtra Division List To The Coordinator of Devagiri DivisionDocument3 pagesAyurved Vyaspeeth Dainandini 2022 List of Coordinators For Maharashtra Division List To The Coordinator of Devagiri DivisionAnand YadavNo ratings yet
- Chikitsa ChatushpadaDocument4 pagesChikitsa ChatushpadaAnand YadavNo ratings yet
- Chikitsa ChatuspadDocument2 pagesChikitsa ChatuspadAnand YadavNo ratings yet
- Cow Product ListDocument2 pagesCow Product ListAnand YadavNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- From Earth To Hair Reviewing Herbal Shampoo BarDocument8 pagesFrom Earth To Hair Reviewing Herbal Shampoo BarDarshana BafnaNo ratings yet
- Suranjan PmsDocument10 pagesSuranjan PmsFSTPS Switch-YardNo ratings yet
- A Quality Improvement Initiative To Engage Older Adults in The DiDocument128 pagesA Quality Improvement Initiative To Engage Older Adults in The Disara mohamedNo ratings yet
- Update Stok & Harga 25 Januari 2022Document17 pagesUpdate Stok & Harga 25 Januari 2022Feny RafnasariNo ratings yet
- 2022 6280 ACG Oxygen Generators Status 30 Junio 2022 FinalesDocument2 pages2022 6280 ACG Oxygen Generators Status 30 Junio 2022 FinalesDeisy BonillaNo ratings yet
- Ebn in Critical Care NursingDocument9 pagesEbn in Critical Care Nursingprima satriadelinNo ratings yet
- Research Paper Topics On CubaDocument5 pagesResearch Paper Topics On Cubaggteukwhf100% (1)
- Stok Opnmae FixDocument6 pagesStok Opnmae FixRossa patria NandaNo ratings yet
- Medical Reimbursement Dipika Vasava 2019-20Document2 pagesMedical Reimbursement Dipika Vasava 2019-20praful2604No ratings yet
- 0301omar Yusef Kudsi - Robotic Hernia Surgery - A Comprehensive Illustrated Guide-Springer International Publishing - Springer (2020)Document25 pages0301omar Yusef Kudsi - Robotic Hernia Surgery - A Comprehensive Illustrated Guide-Springer International Publishing - Springer (2020)ravikanth100% (1)
- Importer ListDocument26 pagesImporter ListRiyaz Rangrez100% (1)
- Eko Fransiska - Pelayanan Dispensing Sediaan Steril Berdasarkan Standar UspDocument49 pagesEko Fransiska - Pelayanan Dispensing Sediaan Steril Berdasarkan Standar Uspmulla ali qoriNo ratings yet
- Underweight Assessment Parameters Final-1Document3 pagesUnderweight Assessment Parameters Final-1Yuvraj GargNo ratings yet
- Grade 11 - ABM - Araling Panlipunan - Applied Economics - Week 1Document11 pagesGrade 11 - ABM - Araling Panlipunan - Applied Economics - Week 1Christian LapidNo ratings yet
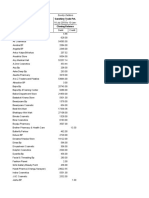
- Particulars Closing Balance Sunshine Trade Pvt. LTD.: Sundry DebtorsDocument5 pagesParticulars Closing Balance Sunshine Trade Pvt. LTD.: Sundry DebtorsRajiv NeupaneNo ratings yet
- Public Employment Service Office: Republic of The Philippines Province of Surigao Del Sur - OooDocument4 pagesPublic Employment Service Office: Republic of The Philippines Province of Surigao Del Sur - OooLUMACTOD , Jemie RoseNo ratings yet
- RestrainingDocument45 pagesRestrainingRizwanNo ratings yet
- Communication, Collegiality and Collaboration..Document4 pagesCommunication, Collegiality and Collaboration..Maina PeterNo ratings yet
- Rhetorical Analysis Finaldraft 043022 BartlingDocument4 pagesRhetorical Analysis Finaldraft 043022 Bartlingapi-310408707No ratings yet
- Progressive OverloadDocument10 pagesProgressive OverloadDerrick AngNo ratings yet
- Kepuasan Pasien Terhadap Kualitas Pelayanan Pasien Rawat Jalan Rumah Sakit Di 7 Provinsi Di IndonesiaDocument12 pagesKepuasan Pasien Terhadap Kualitas Pelayanan Pasien Rawat Jalan Rumah Sakit Di 7 Provinsi Di IndonesiaTHOHAROHNo ratings yet
- First Aid Box ChecklistDocument1 pageFirst Aid Box ChecklistNaveenNo ratings yet
- Hoja Médica IWW Art16Document7 pagesHoja Médica IWW Art16pedroNo ratings yet
- Topic 5 DQ 2.Document3 pagesTopic 5 DQ 2.Emmanuel OpiyoNo ratings yet
- 6 Sept 23 LKDocument178 pages6 Sept 23 LKDurrah Zati YumnaNo ratings yet
- Tivigra LM CRT LabelDocument2 pagesTivigra LM CRT Labelshishi chikkuNo ratings yet
- Antimicrobial Susceptibility TestingDocument5 pagesAntimicrobial Susceptibility TestingChristine BuenNo ratings yet
- Village and Town Directory: Part Xii - ADocument468 pagesVillage and Town Directory: Part Xii - Aabhishek5810No ratings yet
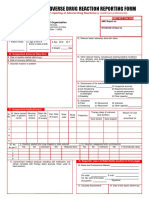
- Adr Form Pvpi PDFDocument2 pagesAdr Form Pvpi PDFAndris SundaeNo ratings yet
- Quackwatch Rebuttal 2Document17 pagesQuackwatch Rebuttal 2mathoni100% (1)