You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gregory Lessing Garrett - Stand or Fall in The COVID 19 Chess GameDocument122 pagesGregory Lessing Garrett - Stand or Fall in The COVID 19 Chess Gamedjv1985100% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Rule 1070 Occupational Health and Environmental ControlDocument10 pagesRule 1070 Occupational Health and Environmental ControlJaime VillalunaNo ratings yet
- Pre-Test Psychiatric NursingDocument17 pagesPre-Test Psychiatric NursingDefensor Pison Gringgo100% (1)
- Psychiatrics McqsDocument20 pagesPsychiatrics McqsHirwaNo ratings yet
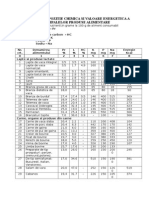
- Tabele de Compozitie Chimica Si Valoare Energetica A Principalelor Produse AlimentareDocument6 pagesTabele de Compozitie Chimica Si Valoare Energetica A Principalelor Produse AlimentareVlad Hadarean Munteanu0% (1)
- TriageDocument4 pagesTriageTenIs ForMeNo ratings yet
- (Tim Lang, Michael Heasman) Food Wars The GlobalDocument385 pages(Tim Lang, Michael Heasman) Food Wars The GlobalNitish Gautam100% (1)
- Indispensable Companion To Dr. Pagano's: Praise For Dr. John's Healing Psoriasis Cookbook "This Valuable Cookbook Is TheDocument12 pagesIndispensable Companion To Dr. Pagano's: Praise For Dr. John's Healing Psoriasis Cookbook "This Valuable Cookbook Is TheСергей ОлейникNo ratings yet
- Case Analysis: Republic of The Philippines Bicol UniversityDocument7 pagesCase Analysis: Republic of The Philippines Bicol UniversityTrixia AlmendralNo ratings yet
- MyBRD Bank Statement SummaryDocument4 pagesMyBRD Bank Statement SummaryDiana DiaconuNo ratings yet
- ArticolDocument9 pagesArticolDiana DiaconuNo ratings yet
- 10 1067@moe 2000 109780Document4 pages10 1067@moe 2000 109780Diana DiaconuNo ratings yet
- Romanian Journal Analyzes Oral Rehabilitation Methods for Kennedy I EdentulismDocument8 pagesRomanian Journal Analyzes Oral Rehabilitation Methods for Kennedy I EdentulismBuzoianu Mihaela-AndreeaNo ratings yet
- Presentation, Analysis, and Interpretation of Data: Springfield School of NovalichesDocument37 pagesPresentation, Analysis, and Interpretation of Data: Springfield School of Novalichestristan espinosaNo ratings yet
- Health Teaching Plan Mars and LainDocument7 pagesHealth Teaching Plan Mars and LainMarissa AsimNo ratings yet
- Askep Kanker ParuDocument39 pagesAskep Kanker ParuNanaRathnaNo ratings yet
- Establish and Maintain Whs Safety System1Document46 pagesEstablish and Maintain Whs Safety System1raj ramukNo ratings yet
- Wiki CataractDocument20 pagesWiki CataractUnggul YudhaNo ratings yet
- Prof DR Akram ICUDocument233 pagesProf DR Akram ICUramzi MohamedNo ratings yet
- PhysioEx Exercise 11 Activity 3Document3 pagesPhysioEx Exercise 11 Activity 3MEGAN NICOLE PERNILLA HERNANDEZNo ratings yet
- What Is Stomatitis DiseaseDocument4 pagesWhat Is Stomatitis DiseaseRoyster CabralNo ratings yet
- Bataan National High School Genre IdentificationDocument10 pagesBataan National High School Genre IdentificationMarc Andrei MirandaNo ratings yet
- Critical Reasoning Document Focuses on Health Issues in IndiaDocument12 pagesCritical Reasoning Document Focuses on Health Issues in Indiapushpendra kumar vashishthaNo ratings yet
- General Animal Surgery and Anaesthesiology (VetBooks - Ir)Document430 pagesGeneral Animal Surgery and Anaesthesiology (VetBooks - Ir)Giovana BragaNo ratings yet
- Pathognomonic Imaging Signs in Abdominal RadiologyDocument11 pagesPathognomonic Imaging Signs in Abdominal RadiologyifzarNo ratings yet
- Fauquert 2019@Document10 pagesFauquert 2019@Angel LimNo ratings yet
- ICD 10 Diagnosis Code ReferenceDocument4 pagesICD 10 Diagnosis Code Referenceady suciptoNo ratings yet
- VN8 Term 2 Calendar Updated June 2, 2021Document7 pagesVN8 Term 2 Calendar Updated June 2, 2021Janmarie BongcaronNo ratings yet
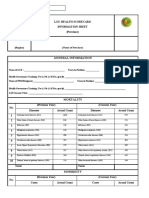
- LGU health scorecard info sheetDocument2 pagesLGU health scorecard info sheetToni Quitalig GamezNo ratings yet
- Peptic Ulcer Disease: by Aniedu, UgochukwuDocument32 pagesPeptic Ulcer Disease: by Aniedu, UgochukwuManish Sapkota100% (1)
- Definition and General Features 4.i 5.12.Document216 pagesDefinition and General Features 4.i 5.12.Elma RamakicNo ratings yet
- GR Up: Ultrasound of Maxillary SinusDocument14 pagesGR Up: Ultrasound of Maxillary SinusSatrya DitaNo ratings yet
- 3 Features of Public HealthDocument12 pages3 Features of Public HealthMoreiyamNo ratings yet
- Chapter 12 Section 3Document21 pagesChapter 12 Section 3api-240305777No ratings yet
- Using The ABCDE Approach For All Critically Unwell PatientsDocument6 pagesUsing The ABCDE Approach For All Critically Unwell PatientsYustitiNo ratings yet