You might also like
- Scrotal SwellingDocument123 pagesScrotal SwellingLestari Amelia AdmNo ratings yet
- General Surgery: (Acute Abdomen)Document1 pageGeneral Surgery: (Acute Abdomen)MattNo ratings yet
- Physiology Magdy Sabry Autonomic, Nerve, MuscleDocument104 pagesPhysiology Magdy Sabry Autonomic, Nerve, Musclegmneur100% (4)
- Pediatric SmleDocument218 pagesPediatric SmleKholoud Kholoud100% (2)
- PathophysiologyDocument7 pagesPathophysiologyJerica Mae VenoyaNo ratings yet
- Emergency UrologyDocument56 pagesEmergency UrologyayususantinaNo ratings yet
- Module 6 - Benign Gynecologic TumorsDocument9 pagesModule 6 - Benign Gynecologic TumorsRenz Francis SasaNo ratings yet
- Urinary IncontinenceDocument1 pageUrinary IncontinenceZiyad100% (1)
- Chapter 1 Sepsis Practise QuestionsDocument6 pagesChapter 1 Sepsis Practise QuestionsAzra MuzafarNo ratings yet
- Benign Diseases of Vulva and VaginaDocument6 pagesBenign Diseases of Vulva and VaginaTj Kevin P-DoctorNo ratings yet
- Evaluation of The Painful EyeDocument9 pagesEvaluation of The Painful EyeMuthia Farah AshmaNo ratings yet
- Assignment GiDocument14 pagesAssignment GiVoid LessNo ratings yet
- Vascular Access For HemodialysisDocument6 pagesVascular Access For HemodialysisWira Dat100% (1)
- Infectious Keratitis Final PDFDocument99 pagesInfectious Keratitis Final PDFGetenet shumetNo ratings yet
- The Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesFrom EverandThe Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesNo ratings yet
- Acute Painful Scrotum: ALGORITHM-Suspicion For Testicular TorsionDocument13 pagesAcute Painful Scrotum: ALGORITHM-Suspicion For Testicular TorsionM. ANDRI PRASETYONo ratings yet
- UrolithiasisDocument9 pagesUrolithiasisJessa MaeNo ratings yet
- Acute Abdomen Practical Approach FransDocument29 pagesAcute Abdomen Practical Approach FransAbel MncaNo ratings yet
- Abdominal PDFDocument1 pageAbdominal PDFChakra BaktiNo ratings yet
- Torsio Testis 1Document3 pagesTorsio Testis 1Wialda Dwi rodyahNo ratings yet
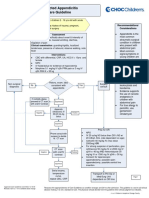
- Suspected Appendicitis Care GuidelineDocument3 pagesSuspected Appendicitis Care GuidelinetamiNo ratings yet
- php7EypFo U4v33rDocument16 pagesphp7EypFo U4v33rRiza Fadhila MuhammadNo ratings yet
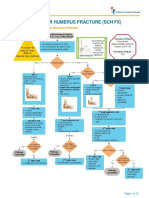
- Fracture Supracondylar HumerusDocument12 pagesFracture Supracondylar HumeruskemsNo ratings yet
- Algorith UTI 20121218 PDFDocument1 pageAlgorith UTI 20121218 PDFIin fermitaNo ratings yet
- Emergenze Addome RXDocument9 pagesEmergenze Addome RXBrovazzo PieroNo ratings yet
- Testicular Torsion: Basic Information DiagnosisDocument2 pagesTesticular Torsion: Basic Information DiagnosisFaisal Ridho SNo ratings yet
- Acute Scrotal PainDocument46 pagesAcute Scrotal PainAdi SetiawanNo ratings yet
- EndometriosisDocument14 pagesEndometriosis01OrietammNo ratings yet
- 4 Protocol For Snakebite Management 1.4Document1 page4 Protocol For Snakebite Management 1.4Aakash BalasubramanianNo ratings yet
- Syndromic Management of STIsDocument1 pageSyndromic Management of STIsJoyNo ratings yet
- WBS Kul - Trauma UroDocument19 pagesWBS Kul - Trauma UroRizal ArzaniNo ratings yet
- 27 Testicular PainDocument2 pages27 Testicular PainazizaaharisNo ratings yet
- EAU Pocket On Paediatric Urology 2023Document54 pagesEAU Pocket On Paediatric Urology 2023Andrea SzaszNo ratings yet
- Appendicitis: Anetha Jodhan Ravindra SinghDocument34 pagesAppendicitis: Anetha Jodhan Ravindra SinghMarlon GeorgeNo ratings yet
- Testicular Torsion, Peds Cases NotesDocument1 pageTesticular Torsion, Peds Cases NotesdzalhcNo ratings yet
- finalsURINARY ELIMINATION DIAGNOSTICSDocument11 pagesfinalsURINARY ELIMINATION DIAGNOSTICSFrances LiqueNo ratings yet
- PromDocument1 pagePromwedishaNo ratings yet
- 84 - UTI Ed and Uc Culture Results Decision TreeDocument1 page84 - UTI Ed and Uc Culture Results Decision TreeShimelis TadesseNo ratings yet
- Management of Abnormal Uterine Bleeding Peripheral Unit: Female Presenting To A With AUBDocument1 pageManagement of Abnormal Uterine Bleeding Peripheral Unit: Female Presenting To A With AUBwedishaNo ratings yet
- Testicular Torsion Fani FinalDocument31 pagesTesticular Torsion Fani Finalrockblaster80No ratings yet
- Acute Pelvic Pain: HistoryDocument4 pagesAcute Pelvic Pain: HistoryMohamed Al-zichrawyNo ratings yet
- Laparoscopic in TraumaDocument37 pagesLaparoscopic in TraumaronaldNo ratings yet
- EAU Pocket On Paediatric Urology 2022Document54 pagesEAU Pocket On Paediatric Urology 2022AlbalushiNo ratings yet
- Syndromic ManagemtDocument4 pagesSyndromic ManagemtKain ValkyrieNo ratings yet
- Vi. Nursing Care Plan Cues Analysis Nursing Diagnosis Goal / Plan Intervention Rationale EvaluationDocument2 pagesVi. Nursing Care Plan Cues Analysis Nursing Diagnosis Goal / Plan Intervention Rationale EvaluationRaisa Robelle QuichoNo ratings yet
- Mat 1Document5 pagesMat 1Shainnie IsmaelNo ratings yet
- (OB GRP 2) SGD - Ovarian Cyst in PregnancyDocument4 pages(OB GRP 2) SGD - Ovarian Cyst in PregnancyRicky Justin NgoNo ratings yet
- Urological RefferalDocument12 pagesUrological Refferalmichelle octavianiNo ratings yet
- Asynchronous 3 - FINALSDocument8 pagesAsynchronous 3 - FINALSWellanie Guillena TamalaNo ratings yet
- Ectopic PregnancyDocument13 pagesEctopic PregnancyJonielyn LagunaNo ratings yet
- Kuliah Trauma Urologi - DR WibisonoDocument34 pagesKuliah Trauma Urologi - DR WibisonoAgung Budi SuristioNo ratings yet
- Emergency Urology Non TraumaticDocument51 pagesEmergency Urology Non TraumaticJeremi SetiawanNo ratings yet
- Drug Dose Route Indicatio N Contraindication Action Sideffe CT Nursing ConsiderationDocument3 pagesDrug Dose Route Indicatio N Contraindication Action Sideffe CT Nursing ConsiderationAnaliza Vios YaoNo ratings yet
- Case: Renal and Genitourinary Block Week 3 General DataDocument19 pagesCase: Renal and Genitourinary Block Week 3 General DataEveryday FundayNo ratings yet
- Isolated Hematuria - Genitourinary Disorders - MSD Manual Professional EditionDocument3 pagesIsolated Hematuria - Genitourinary Disorders - MSD Manual Professional EditionleozdmNo ratings yet
- Rauma Epar: Soetamto Wibowo Bagian Bedah FK UNAIR / RSUD DR Soetomo SurabayaDocument37 pagesRauma Epar: Soetamto Wibowo Bagian Bedah FK UNAIR / RSUD DR Soetomo SurabayaMuhammad FirdausNo ratings yet
- 6 SURGERY II 6 - Pediatric UrologyDocument6 pages6 SURGERY II 6 - Pediatric UrologyDeann RoscomNo ratings yet
- CefuroximeDocument2 pagesCefuroximeAnreezahy GnoihcNo ratings yet
- Appendix Anatomy: SURGERY 2 - G.I. ModuleDocument2 pagesAppendix Anatomy: SURGERY 2 - G.I. ModuleFrances Isabella OlasimanNo ratings yet
- Differential Diagnosis of Placenta Praevia and AbruptioDocument1 pageDifferential Diagnosis of Placenta Praevia and Abruptiojalan_zNo ratings yet
- Revised NCPDocument6 pagesRevised NCPTiffany AdriasNo ratings yet
- Women's HealthDocument8 pagesWomen's HealthkellyjackykjNo ratings yet
- Button Battery Ingestion Birmingham Childrens Hospital 2013Document1 pageButton Battery Ingestion Birmingham Childrens Hospital 2013rashidNo ratings yet
- Gynecological Assessment: DateDocument4 pagesGynecological Assessment: Dateanne laureNo ratings yet
- Kuliah Traumatologi Abdomen DewasaDocument19 pagesKuliah Traumatologi Abdomen DewasaIndra GunawanNo ratings yet
- (Surgery) Midterms PediatricsDocument5 pages(Surgery) Midterms Pediatricsalmira.s.mercadoNo ratings yet
- Sacral Dimple Org PathwayDocument10 pagesSacral Dimple Org PathwayViolaNo ratings yet
- Transcription and Translation Power PointDocument21 pagesTranscription and Translation Power Pointapi-176402481No ratings yet
- 0127「小兒遺傳及代謝」講師陳燕彰醫師Document114 pages0127「小兒遺傳及代謝」講師陳燕彰醫師許懷朔No ratings yet
- Headache ReviewDocument8 pagesHeadache Reviewoscar nieblesNo ratings yet
- OBGYN Manual - Preceptorial Module 2019-2020 Final Export PDFDocument14 pagesOBGYN Manual - Preceptorial Module 2019-2020 Final Export PDFJerwin EstacioNo ratings yet
- Reactii Adverse Dupa Administrare de IodineDocument8 pagesReactii Adverse Dupa Administrare de IodineahmadNo ratings yet
- Shonihari Hari Boston 04082019Document18 pagesShonihari Hari Boston 04082019William TellNo ratings yet
- Chirurgia TiroideiDocument15 pagesChirurgia TiroideiAna CotomanNo ratings yet
- Lic Health Plus FormDocument27 pagesLic Health Plus FormKuldeep Chakerwarti100% (1)
- Nur Intan Saidaah - NUR INTAN SAIDAAH MOHAMED YUSOFDocument2 pagesNur Intan Saidaah - NUR INTAN SAIDAAH MOHAMED YUSOFNhan NguyenNo ratings yet
- Clinical Manifestations and Diagnosis of Raynaud Phenomenon - UpToDateDocument29 pagesClinical Manifestations and Diagnosis of Raynaud Phenomenon - UpToDateMarcos Torchia EstebanNo ratings yet
- LipoproteinsDocument30 pagesLipoproteinsApurba PradhanNo ratings yet
- Medical Surgical NotesDocument18 pagesMedical Surgical NotesshalomNo ratings yet
- Alzheimer'sDocument18 pagesAlzheimer'sUltimate ChallengeNo ratings yet
- Revised Nematodes Specimens With Labels 2NMT Moving PracticalsDocument45 pagesRevised Nematodes Specimens With Labels 2NMT Moving PracticalsRudolph MendozaNo ratings yet
- Clinical Concept MapDocument5 pagesClinical Concept MapMj FernandezNo ratings yet
- Antipyretic-Analgesic and Anti-Inflammatory Drugs (Nsaids)Document43 pagesAntipyretic-Analgesic and Anti-Inflammatory Drugs (Nsaids)Ritu ShewaniNo ratings yet
- Dialysis ReviewerDocument16 pagesDialysis ReviewerlarraNo ratings yet
- Cardio Nursing - Course Audit 2Document320 pagesCardio Nursing - Course Audit 2Ciella Dela CruzNo ratings yet
- College of Nursing: Pharmacological ManagementDocument3 pagesCollege of Nursing: Pharmacological ManagementNathanielle Keith PENASONo ratings yet
- Examination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaDocument29 pagesExamination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaForeighn97No ratings yet
- Dizziness HXDocument4 pagesDizziness HXbadmanNo ratings yet
- Acute Necrotizing Sinusitis Caused by Staphylococcus Lugdunensis 2011Document3 pagesAcute Necrotizing Sinusitis Caused by Staphylococcus Lugdunensis 2011J Sebastian PeinadoNo ratings yet
- Histo NervousDocument20 pagesHisto NervousALESSANDRA CELINo ratings yet