You might also like
- NCP. Deficient Fluid Volume by Eben D.C.Document1 pageNCP. Deficient Fluid Volume by Eben D.C.dominoredwing2024100% (1)
- Ncp.-Fluid Volume DeficitDocument1 pageNcp.-Fluid Volume DeficitAdia Cavrinni De JesusNo ratings yet
- Nursing Care Plan: IndependentDocument2 pagesNursing Care Plan: IndependentAdhaNo ratings yet
- Betty Impaired Skin IntegrityDocument2 pagesBetty Impaired Skin IntegrityBenjie DimayacyacNo ratings yet
- NCP RiskDocument3 pagesNCP RiskMaricar Azolae MascualNo ratings yet
- Assessing and Treating Acute Gastroenteritis and DehydrationDocument2 pagesAssessing and Treating Acute Gastroenteritis and DehydrationvicenteturasNo ratings yet
- NCPDocument1 pageNCPJ. ishtelleNo ratings yet
- NCP Delayed Wound RecoveryDocument5 pagesNCP Delayed Wound RecoveryDarkCeades100% (2)
- Activity IntoleranceDocument2 pagesActivity IntolerancedohbleNo ratings yet
- Nursing Care Plan For RabiesDocument1 pageNursing Care Plan For RabiesAngel VillamorNo ratings yet
- NCP StressDocument2 pagesNCP StressWaqas Javed100% (7)
- Gouty Arthritis-NcpDocument2 pagesGouty Arthritis-NcpJohn D100% (2)
- Fluid Volume DeficitDocument1 pageFluid Volume DeficitventimiglionNo ratings yet
- NCP Acute PainDocument5 pagesNCP Acute PainMicah Jonah Elicaño0% (1)
- NCP Acute Pain R/T Injuring AgentsDocument4 pagesNCP Acute Pain R/T Injuring AgentsKevin Sam AguirreNo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation GoalDocument2 pagesAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation GoalI Am SmilingNo ratings yet
- PEDIA NCP Risk For BleedingDocument2 pagesPEDIA NCP Risk For BleedingTricia DogilloNo ratings yet
- NCP 2Document2 pagesNCP 2Neil Abraham Mendoza Lalap100% (2)
- NCPDocument2 pagesNCPDidith AbanNo ratings yet
- NCP HemothoraxDocument3 pagesNCP HemothoraxMichael John F. NatividadNo ratings yet
- Nursing Care Plan for Enhanced NutritionDocument2 pagesNursing Care Plan for Enhanced NutritionHippocrates Impressionist CostalesNo ratings yet
- NCP Surgery WardDocument6 pagesNCP Surgery WardZNEROL100% (2)
- Oral rehydrating solution (ORESOL) nursing responsibilitiesDocument8 pagesOral rehydrating solution (ORESOL) nursing responsibilitiesLeslie PaguioNo ratings yet
- Flank Pain, Anxiety...Document7 pagesFlank Pain, Anxiety...reneighdNo ratings yet
- NCP: Acute GastroenteritisDocument3 pagesNCP: Acute GastroenteritishauteanicoleNo ratings yet
- Assess and Care for Impaired Oral Mucous MembranesDocument2 pagesAssess and Care for Impaired Oral Mucous MembranesNolan Cabral100% (1)
- Multiodular non toxic goiter nursing care planDocument1 pageMultiodular non toxic goiter nursing care plankzbreakerrNo ratings yet
- NCP For Ineffective Breathing Pattern - RMC CasepressDocument2 pagesNCP For Ineffective Breathing Pattern - RMC Casepressmissyuri08No ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationArian May MarcosNo ratings yet
- NCP - Impaired Skin IntegrityDocument4 pagesNCP - Impaired Skin IntegrityColette Marie PerezNo ratings yet
- NCP HemothoraxDocument3 pagesNCP Hemothoraxroseonabreeze0% (2)
- Llacer FdarDocument2 pagesLlacer FdarRaidis PangilinanNo ratings yet
- NCPDocument3 pagesNCPeun kyung shinNo ratings yet
- Ncp-Readiness For Enhanced Knowledge Related To Preoperative CareDocument1 pageNcp-Readiness For Enhanced Knowledge Related To Preoperative CareAce Dioso Tubasco50% (2)
- Date/Time Focus Progress NotesDocument2 pagesDate/Time Focus Progress Notesanna jean oliquianoNo ratings yet
- Nursing Care Plan2 CVADocument4 pagesNursing Care Plan2 CVAhermesdave1No ratings yet
- NCP-Risk For Fluid Volume DeficitDocument3 pagesNCP-Risk For Fluid Volume DeficitJai Go100% (1)
- Short Term: Independent: Independent: Short TermDocument2 pagesShort Term: Independent: Independent: Short TermAndre ImperialNo ratings yet
- XI. Nursing Care Plan Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation SubjectiveDocument4 pagesXI. Nursing Care Plan Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation SubjectiveMartin Allen ClaudioNo ratings yet
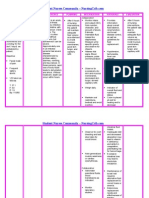
- Student Nurses’ Community NURSING CARE PLAN – Renal FailureDocument2 pagesStudent Nurses’ Community NURSING CARE PLAN – Renal FailureAldrein GonzalesNo ratings yet
- Multi Noduar Colloid GoiterDocument1 pageMulti Noduar Colloid GoiterVincent John Faller100% (1)
- GENERAL SANTOS DOCTORS’ MEDICAL SCHOOL FOUNDATION NURSING CARE PLANDocument4 pagesGENERAL SANTOS DOCTORS’ MEDICAL SCHOOL FOUNDATION NURSING CARE PLANFran LanNo ratings yet
- Impaired Skin IntegrityDocument1 pageImpaired Skin IntegrityHanya Bint PotawanNo ratings yet
- Clinical Example:: What Additional Assessments Would The Nurse Want To Make To Plan Care For This Client?Document2 pagesClinical Example:: What Additional Assessments Would The Nurse Want To Make To Plan Care For This Client?Kim Kristine D. GuillenNo ratings yet
- Nursing Care Plan for Rheumatoid ArthritisDocument3 pagesNursing Care Plan for Rheumatoid ArthritisJashAnia MarIe EvArdo FloresNo ratings yet
- Activity IntoleranceDocument2 pagesActivity IntoleranceJaney Ceniza تNo ratings yet
- Nursing Care Plan for Activity IntoleranceDocument3 pagesNursing Care Plan for Activity Intolerancelouie roderos0% (1)
- NCP PryllDocument6 pagesNCP PryllpjcolitaNo ratings yet
- NCP HyperthermiaDocument2 pagesNCP HyperthermiaKirby ContaoiNo ratings yet
- NCP DMDocument6 pagesNCP DMstara123No ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Implementation Rationale EvaluationDocument1 pageNursing Care Plan Assessment Diagnosis Planning Implementation Rationale EvaluationMyrien BanaagNo ratings yet
- Risk For Deficient Fluid Volume Best NCPDocument2 pagesRisk For Deficient Fluid Volume Best NCPMikko Anthony Pingol Alarcon83% (46)
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- NCP Deficit Fluid VolumeDocument4 pagesNCP Deficit Fluid VolumeKingJayson Pacman06No ratings yet
- Nursing Care PL WPS OfficeDocument3 pagesNursing Care PL WPS OfficeDhan IvanNo ratings yet
- NURSING CARE PLAN - CholeraDocument2 pagesNURSING CARE PLAN - Choleraderic87% (30)
- Nursing Care Plan Human Response Pattern AMB/Manifestation Nursing Diagnosis Goal/ Outcome Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan Human Response Pattern AMB/Manifestation Nursing Diagnosis Goal/ Outcome Nursing Intervention Rationale EvaluationMarielle Chua100% (1)
- Nursing Care Plan for Diabetic Client with Imbalanced NutritionDocument3 pagesNursing Care Plan for Diabetic Client with Imbalanced NutritionSean Philippe CabralNo ratings yet
- Final NCP1 2Document2 pagesFinal NCP1 2hahahahaaaaaaaNo ratings yet
- DM NCP - Trixia U. Almendral GRP 6Document3 pagesDM NCP - Trixia U. Almendral GRP 6Trixia AlmendralNo ratings yet
- PneumoniaDocument1 pagePneumoniaAlbean DelojeroNo ratings yet
- Myocardial InfarctionDocument2 pagesMyocardial InfarctionAlbean DelojeroNo ratings yet
- Classification: PneumoniaDocument2 pagesClassification: PneumoniaAlbean DelojeroNo ratings yet
- Myocardial InfarctionDocument2 pagesMyocardial InfarctionAlbean DelojeroNo ratings yet
- Fetal Alcohol SyndromeDocument1 pageFetal Alcohol SyndromeAlbean DelojeroNo ratings yet
- AsthmaDocument2 pagesAsthmaAlbean DelojeroNo ratings yet
- Education Role Nurses Health CareDocument2 pagesEducation Role Nurses Health CareAlbean DelojeroNo ratings yet
- Basic Principles of TeachingDocument5 pagesBasic Principles of TeachingAlbean DelojeroNo ratings yet
- What Is PsoriasisDocument6 pagesWhat Is PsoriasisAlbean DelojeroNo ratings yet
- TheDocument1 pageThejelaicaNo ratings yet
- Good Morning Everyone, Our Topic To Tackle About Is Balantidium ColiDocument1 pageGood Morning Everyone, Our Topic To Tackle About Is Balantidium ColiAlbean DelojeroNo ratings yet
- The Nurse As An EducatorDocument4 pagesThe Nurse As An EducatorAlbean DelojeroNo ratings yet
- Juliet and RomeoDocument1 pageJuliet and RomeoAlbean DelojeroNo ratings yet
- COVID-19 causes, symptoms, transmission and preventionDocument1 pageCOVID-19 causes, symptoms, transmission and preventionAlbean DelojeroNo ratings yet
- Romeo and JulietDocument1 pageRomeo and JulietAlbean DelojeroNo ratings yet
- Life of PiDocument1 pageLife of PiAnonymous ISxk3Q5AL3No ratings yet
- Europe Notes PDF-1Document9 pagesEurope Notes PDF-1Abe Carelle B. GonzalesNo ratings yet
- Choose and Encircle The Letter of The Correct AnswerDocument1 pageChoose and Encircle The Letter of The Correct AnswerAlbean DelojeroNo ratings yet
- Self-Assessment of Nursing Standards of PracticeDocument32 pagesSelf-Assessment of Nursing Standards of Practiceapi-242114301No ratings yet
- Lesson Plan On Antenatal CareDocument23 pagesLesson Plan On Antenatal CareRavina Patel91% (22)
- MSCDFSM Prog. GuideDocument108 pagesMSCDFSM Prog. Guidesamraju1No ratings yet
- Movie Review - Psychological Disorder PortrayedDocument3 pagesMovie Review - Psychological Disorder Portrayedwebster080808No ratings yet
- Bender Gestalt TestDocument3 pagesBender Gestalt TestAleena ThakurtaNo ratings yet
- Volunteer Handbook 2019Document12 pagesVolunteer Handbook 2019Katharine Tondra100% (1)
- S2 2021 447732 BibliographyDocument4 pagesS2 2021 447732 BibliographyNovriani Warap SariNo ratings yet
- 17 Types of Working Conditions - SimplicableDocument23 pages17 Types of Working Conditions - SimplicableSharina Canaria ObogNo ratings yet
- Treat Chronic DacryocystitisDocument34 pagesTreat Chronic DacryocystitisAriyanie NurtaniaNo ratings yet
- 10.1007@s11065 020 09443 7Document14 pages10.1007@s11065 020 09443 7José NettoNo ratings yet
- Teks EksposisiDocument2 pagesTeks EksposisiHadiq IbnuNo ratings yet
- Aubf Lab 7Document1 pageAubf Lab 7Regina SalazarNo ratings yet
- Article Zoë Dubus: Utiliser Les Psychédéliques Pour Guérir Des Adolescents Homosexuels ? Essai de Thérapie de Conversion, France, 1960Document16 pagesArticle Zoë Dubus: Utiliser Les Psychédéliques Pour Guérir Des Adolescents Homosexuels ? Essai de Thérapie de Conversion, France, 1960France3AlsaceNo ratings yet
- Agency ProjectDocument14 pagesAgency Projectapi-304517936No ratings yet
- Becoming a NeurologistDocument3 pagesBecoming a NeurologistnorlelaoNo ratings yet
- Myanmar Health Assistant Association Vacancy Announcement (VA - 052/2023 MHAA-HR)Document3 pagesMyanmar Health Assistant Association Vacancy Announcement (VA - 052/2023 MHAA-HR)Zawhtet HtetNo ratings yet
- 681 FullDocument6 pages681 FullKurnia AnharNo ratings yet
- Mental: Your Health MattersDocument2 pagesMental: Your Health MattersKrsnaPentayahNo ratings yet
- Fast Food Nation EssayDocument5 pagesFast Food Nation EssayBen SmithNo ratings yet
- Sample Risk Assessment MatrixDocument32 pagesSample Risk Assessment Matrixrobinrubina100% (2)
- Baking Soda Cures Cancer, Fungus and InflammationDocument6 pagesBaking Soda Cures Cancer, Fungus and Inflammationsheriff77080% (5)
- Aplastic AnemiaDocument21 pagesAplastic AnemiaJennifer DixonNo ratings yet
- TFN Resource UnitDocument80 pagesTFN Resource UnitAira Alaro50% (2)
- Psychology Dissertation Research TopicsDocument7 pagesPsychology Dissertation Research TopicsHelpWritingPapersSingapore100% (1)
- MBBS-BDS Stray - Round - SelectionList R4Document462 pagesMBBS-BDS Stray - Round - SelectionList R4Lakshmi ManasaNo ratings yet
- The Durex Story Stretching The MarketDocument4 pagesThe Durex Story Stretching The MarketShwetaGoudNo ratings yet
- The Advanced Bonewits Cult Danger Eval FrameDocument6 pagesThe Advanced Bonewits Cult Danger Eval FrameKelly LincolnNo ratings yet
- TetanusDocument7 pagesTetanusRaven ReyesNo ratings yet
- Tips For Triage NursesDocument4 pagesTips For Triage NursesCamille05No ratings yet
- 5 Horrifying Facts About FDA-Vaccine-Approval-Process-2019Document24 pages5 Horrifying Facts About FDA-Vaccine-Approval-Process-2019Pollyana Furtado JunqueiraNo ratings yet