You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- English For Academic and Professional Purposes: Quarter 1 - Module 2 Text StructureDocument25 pagesEnglish For Academic and Professional Purposes: Quarter 1 - Module 2 Text StructureBeverly Joy BragaisNo ratings yet
- English For Academic and Professional Purposes: Quarter 1 - Module 4 Stating The Thesis Statement of An Academic TextDocument26 pagesEnglish For Academic and Professional Purposes: Quarter 1 - Module 4 Stating The Thesis Statement of An Academic TextBeverly Joy BragaisNo ratings yet
- EAPP Module-1 FinalDocument23 pagesEAPP Module-1 FinalBeverly Joy BragaisNo ratings yet
- English For Academic and Professional Purposes: Quarter 1 - Module 6 Critical Approaches in Writing A Critique PaperDocument22 pagesEnglish For Academic and Professional Purposes: Quarter 1 - Module 6 Critical Approaches in Writing A Critique PaperBeverly Joy BragaisNo ratings yet
- English For Academic and Professional Purposes: Quarter 1 - Module 3 Techniques in Summarizing Variety of Academic TextDocument30 pagesEnglish For Academic and Professional Purposes: Quarter 1 - Module 3 Techniques in Summarizing Variety of Academic TextBeverly Joy BragaisNo ratings yet
- Asgnment No.1 Literary CDocument1 pageAsgnment No.1 Literary CBeverly Joy BragaisNo ratings yet
- Assignment in Foundation of EducationDocument2 pagesAssignment in Foundation of EducationBeverly Joy BragaisNo ratings yet
- Assignment No. 2 AsynchronousDocument1 pageAssignment No. 2 AsynchronousBeverly Joy BragaisNo ratings yet
- Written Output in Comparative EducationDocument1 pageWritten Output in Comparative EducationBeverly Joy BragaisNo ratings yet
- Lesson7explicitandimplicitclaimsinatext 170228091324Document36 pagesLesson7explicitandimplicitclaimsinatext 170228091324Ryan Negad100% (1)
- Asynchronous No. 3 Beverly Joy T. BragaisDocument1 pageAsynchronous No. 3 Beverly Joy T. BragaisBeverly Joy BragaisNo ratings yet
- Asynchronous 3Document1 pageAsynchronous 3Beverly Joy BragaisNo ratings yet
- DLL Per. Dev... Week 4 Nov 26 29Document3 pagesDLL Per. Dev... Week 4 Nov 26 29Beverly Joy Bragais83% (6)
- Elements of Art 11-24-19Document24 pagesElements of Art 11-24-19Beverly Joy BragaisNo ratings yet
- Bring On The Tough Stuff QADocument2 pagesBring On The Tough Stuff QABeverly Joy BragaisNo ratings yet
- Sample Resume TestDocument1 pageSample Resume TestMart Dumali SambaludNo ratings yet
- Elements of Art 11-24-19Document24 pagesElements of Art 11-24-19Beverly Joy BragaisNo ratings yet
- Long Test in PR 1Document1 pageLong Test in PR 1Beverly Joy BragaisNo ratings yet
- Challenges in Adolescence Nov26 30Document4 pagesChallenges in Adolescence Nov26 30Beverly Joy BragaisNo ratings yet
- DLLDocument2 pagesDLLBeverly Joy BragaisNo ratings yet
- RWS11 IVdg 12.4 Position PaperDocument3 pagesRWS11 IVdg 12.4 Position PaperBeverly Joy BragaisNo ratings yet
- Multiple IntelligenceDocument14 pagesMultiple IntelligenceBeverly Joy BragaisNo ratings yet
- Group 2 Quantitative Research Revision 4thDocument26 pagesGroup 2 Quantitative Research Revision 4thBeverly Joy BragaisNo ratings yet
- Challenges in Adolescence Nov26 30Document4 pagesChallenges in Adolescence Nov26 30Beverly Joy BragaisNo ratings yet
- DLL Research 4th WeekDocument4 pagesDLL Research 4th WeekBeverly Joy Bragais100% (2)
- Communication Planning For Career Advocates - FinalDocument77 pagesCommunication Planning For Career Advocates - FinalBeverly Joy Bragais0% (1)
- DLL No.6Document5 pagesDLL No.6Beverly Joy BragaisNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hand Wrist RadiographDocument26 pagesHand Wrist RadiographStephanie Joyce Coojacinto50% (2)
- Ganglions: History and Exam FindingsDocument3 pagesGanglions: History and Exam FindingsAnonymous vOJH2hLMh6No ratings yet
- Physical Therapy Toolkit ™: 66 Treatment Guides 211 HandoutsDocument4 pagesPhysical Therapy Toolkit ™: 66 Treatment Guides 211 HandoutsKiné Therapeut-manuelle Masseur GabiNo ratings yet
- Colle's FractureDocument22 pagesColle's FractureAkshata HingeNo ratings yet
- Thesis by Woong Kim SmallerDocument415 pagesThesis by Woong Kim SmallerWoong KimNo ratings yet
- TCM Protocol For ClassicalDocument26 pagesTCM Protocol For ClassicalDrnarendra KumarNo ratings yet
- Fundamentals of Hand Therapy Clinical Reasoning and Treatment Guidelines For Common Diagnoses of The Upper Extremity PDFDocument561 pagesFundamentals of Hand Therapy Clinical Reasoning and Treatment Guidelines For Common Diagnoses of The Upper Extremity PDFDirk Gently100% (5)
- Instability of The Distal Radioulnar JointDocument12 pagesInstability of The Distal Radioulnar JointOryza SatriaNo ratings yet
- Fracture Treatment ProtocolsDocument14 pagesFracture Treatment ProtocolsZikrul IdyaNo ratings yet
- Leprosy in OrthopedicsDocument91 pagesLeprosy in OrthopedicsAnkit Agur67% (3)
- 판독 양식 (사랑 병원에서 쓰던거)Document24 pages판독 양식 (사랑 병원에서 쓰던거)eosfieldNo ratings yet
- The Treatment of Wrist Instability: Instructional CourseDocument7 pagesThe Treatment of Wrist Instability: Instructional CourseBasmah Al-DhafarNo ratings yet
- White Book On Hand Surgery in Europe EBHSDocument21 pagesWhite Book On Hand Surgery in Europe EBHSmerdan serinNo ratings yet
- Acland's DVD Atlas of Human Anatomy Vol-1-TranscriptDocument36 pagesAcland's DVD Atlas of Human Anatomy Vol-1-TranscriptJaime Quimbayo EdogawaNo ratings yet
- Acupuncture Points - Acupuncture School Online - Learning Acupuncture and Moxibustion Courses OnlineDocument7 pagesAcupuncture Points - Acupuncture School Online - Learning Acupuncture and Moxibustion Courses Onlinecarlos coelhoNo ratings yet
- Lock Distal Radius SystemDocument20 pagesLock Distal Radius SystemBilal AhmadNo ratings yet
- Elbow Joint - 1Document27 pagesElbow Joint - 1SAI BIRADAENo ratings yet
- The Reverse Posterior Interosseous Artery Flap: Technical Considerations in Raising An Easier and More Reliable FlapDocument9 pagesThe Reverse Posterior Interosseous Artery Flap: Technical Considerations in Raising An Easier and More Reliable FlapyeapdshengNo ratings yet
- Fractures of The Distal End of The Radius Treated by Internal Fixation and Early Function. A Preliminary Report of 20 CasesDocument6 pagesFractures of The Distal End of The Radius Treated by Internal Fixation and Early Function. A Preliminary Report of 20 Casessanjay chhawraNo ratings yet
- Classification of Established Volkmann's Ischemic Contracture and The Program For Its TreatmentDocument11 pagesClassification of Established Volkmann's Ischemic Contracture and The Program For Its Treatmentanand swaroopNo ratings yet
- Foundations of Athletic Training Prevention Assessment and Management 6th Edition Ebook PDFDocument62 pagesFoundations of Athletic Training Prevention Assessment and Management 6th Edition Ebook PDFjoshua.lewis822100% (43)
- Volkmann Contracture Causes, Symptoms, and TreatmentDocument4 pagesVolkmann Contracture Causes, Symptoms, and TreatmentAdre RefdianNo ratings yet
- Muscles of the Pectoral Region and BackDocument9 pagesMuscles of the Pectoral Region and Backshananana1616No ratings yet
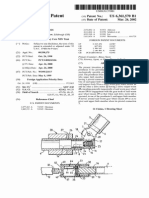
- United States Patent: Gow (10) Patent N0.: (45) Date of PatentDocument5 pagesUnited States Patent: Gow (10) Patent N0.: (45) Date of PatentAdam SalehNo ratings yet
- Basic Principles and Disorders of the Hand, Wrist, Elbow, Forearm and NerveDocument3 pagesBasic Principles and Disorders of the Hand, Wrist, Elbow, Forearm and NerveAlex OprisanNo ratings yet
- RADPOSDocument59 pagesRADPOSLeahjen MaeNo ratings yet
- Manual of Diagnosis and Treatment Su Jok PDFDocument12 pagesManual of Diagnosis and Treatment Su Jok PDFДипак СешадриNo ratings yet
- Acute Carpal Tunnel Syndrome: A Review of Current LiteratureDocument9 pagesAcute Carpal Tunnel Syndrome: A Review of Current LiteratureUlos BenardNo ratings yet
- Neumann: Kinesiology of The Musculoskeletal System, 2nd EditionDocument4 pagesNeumann: Kinesiology of The Musculoskeletal System, 2nd EditionVictor MarianNo ratings yet
- The Ultimate Emergency Medicine Guide Ebook PDF VersionDocument61 pagesThe Ultimate Emergency Medicine Guide Ebook PDF Versiontom.dimaggio515100% (34)