You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
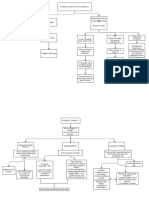
- Strict Liability - Torts - FlowchartDocument3 pagesStrict Liability - Torts - Flowchartfranco-44467% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Medtronic Kanghui Introduction and Trauma PortfolioDocument23 pagesMedtronic Kanghui Introduction and Trauma PortfolioFernandoBonnetNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- March 2022 MCQsDocument17 pagesMarch 2022 MCQsZeeshan Ahmad100% (2)
- Femoral Neck FractureDocument36 pagesFemoral Neck FractureAnonymous ekem7I100% (2)
- Asuncion, MayDocument5 pagesAsuncion, MayPrince Rener Velasco Pera100% (1)
- Bachicha, LutherDocument5 pagesBachicha, LutherPrince Rener Velasco PeraNo ratings yet
- Atiwon, Trina VeahDocument6 pagesAtiwon, Trina VeahPrince Rener Velasco PeraNo ratings yet
- Differentiating Abbreviations From Acronyms: MuscleDocument10 pagesDifferentiating Abbreviations From Acronyms: MusclePrince Rener Velasco PeraNo ratings yet
- Final Exam PHCDocument7 pagesFinal Exam PHCPrince Rener Velasco PeraNo ratings yet
- Bag TechniqueDocument3 pagesBag TechniquePrince Rener Velasco PeraNo ratings yet
- Psych Module 1 (HGD)Document14 pagesPsych Module 1 (HGD)Prince Rener Velasco PeraNo ratings yet
- Remedial Exam PsychDocument7 pagesRemedial Exam PsychPrince Rener Velasco PeraNo ratings yet
- TOS Psych PrelimsDocument1 pageTOS Psych PrelimsPrince Rener Velasco PeraNo ratings yet
- Remedial Part 2Document13 pagesRemedial Part 2Prince Rener Velasco PeraNo ratings yet
- TOS Psych PrelimsDocument1 pageTOS Psych PrelimsPrince Rener Velasco PeraNo ratings yet
- Psych BulletsDocument16 pagesPsych BulletsPrince Rener Velasco PeraNo ratings yet
- Notes On Dissociative DisordersDocument7 pagesNotes On Dissociative DisordersPrince Rener Velasco PeraNo ratings yet
- (ZOO301) Chapter 11 - MusclesDocument17 pages(ZOO301) Chapter 11 - MusclesRain Hong100% (1)
- Unrequited Lovers ClubDocument23 pagesUnrequited Lovers Clubanisasyira06No ratings yet
- Dental CeramicsDocument160 pagesDental CeramicsDenis TorresNo ratings yet
- Transportation LawDocument9 pagesTransportation LawGianno Gray TanNo ratings yet
- Lumbar Disc HerniationDocument14 pagesLumbar Disc HerniationAfifah NurNo ratings yet
- CHAPTER 8 Neck AssestDocument61 pagesCHAPTER 8 Neck AssestLinlin Lindayani KusnandarNo ratings yet
- Or Instruments SampleDocument9 pagesOr Instruments SampleSonia Letran SingsonNo ratings yet
- 11.0 - Incident Notification - Investigation and Reporting v3.0 EnglishDocument34 pages11.0 - Incident Notification - Investigation and Reporting v3.0 Englisheliezer33% (3)
- Plastic Welder Manual 96464Document12 pagesPlastic Welder Manual 96464kshwookNo ratings yet
- Situation Reaction Test Service Selection Test (SSB)Document3 pagesSituation Reaction Test Service Selection Test (SSB)Joseph SimsNo ratings yet
- Lateral Epicondylitis PresentationDocument16 pagesLateral Epicondylitis Presentationapi-317395769No ratings yet
- HerniaDocument61 pagesHerniaAhmed HassanNo ratings yet
- SplintingDocument9 pagesSplintingmichaelNo ratings yet
- Iliopsoas and Gluteal Muscles Are Asymmetric in TennisDocument10 pagesIliopsoas and Gluteal Muscles Are Asymmetric in TennisYoh ChenNo ratings yet
- Boyscout ComplaintDocument13 pagesBoyscout ComplaintlogicfirstNo ratings yet
- sport lec 7 شرحDocument11 pagessport lec 7 شرحShrouq BadrNo ratings yet
- Explanation of HINRI LabsDocument21 pagesExplanation of HINRI Labsjgoode73No ratings yet
- Understanding Hse Key Performance IndicatorsDocument6 pagesUnderstanding Hse Key Performance IndicatorsIsaac KobiNo ratings yet
- GoJu Ryu Karate TechniquesDocument6 pagesGoJu Ryu Karate TechniquesJeff HambreNo ratings yet
- Mosby's EMT Textbook - Revised Reprint, 2011 Update, 2nd Edition 14Document8 pagesMosby's EMT Textbook - Revised Reprint, 2011 Update, 2nd Edition 14Kathrina AlfonsoNo ratings yet
- Dentistry Semester 1 SAQDocument4 pagesDentistry Semester 1 SAQKan Chang YuNo ratings yet
- How The Brain Recovers2Document94 pagesHow The Brain Recovers2Anonymous x75qV3lGNo ratings yet
- Full Download pdf of Joint Structure and Function: A Comprehensive Analysis Fifth Edition all chapterDocument43 pagesFull Download pdf of Joint Structure and Function: A Comprehensive Analysis Fifth Edition all chapterlarcheardu100% (10)
- 2 Year Physical Therapy NotesDocument129 pages2 Year Physical Therapy Notesthwiseman94% (17)
- BiomechanicalDocument20 pagesBiomechanicalJunus EufrataNo ratings yet
- Anterior Triangle of NeckDocument13 pagesAnterior Triangle of NeckÑäd ÉèmNo ratings yet