You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Australasian Health Facility GuidelinesDocument36 pagesAustralasian Health Facility GuidelinesKarlson Spencer Sia TyNo ratings yet
- Nasa RVTL Studies EvtolDocument7 pagesNasa RVTL Studies EvtolKarlson Spencer Sia TyNo ratings yet
- Aia Lactation Wellness Room DesignDocument5 pagesAia Lactation Wellness Room DesignKarlson Spencer Sia TyNo ratings yet
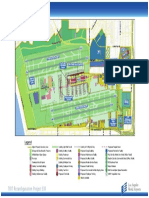
- Lax Master Plan PDFDocument1 pageLax Master Plan PDFKarlson Spencer Sia TyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Peme Not ExploratoryDocument6 pagesPeme Not ExploratoryAldos Medina Jr.No ratings yet
- Jama Mederos 2021 RV 200014 1655494806.72368Document9 pagesJama Mederos 2021 RV 200014 1655494806.72368Soni CollinNo ratings yet
- Economic ZoologyDocument14 pagesEconomic ZoologyHira AroojNo ratings yet
- United Republic of Tanzania: Ministry of Works and TransportDocument10 pagesUnited Republic of Tanzania: Ministry of Works and TransportKipindi Bahati maduhuNo ratings yet
- Eruption of Palatal Canines Following Surgical Exposure: A Review of Outcomes in A Series of Consecutively Treated CasesDocument5 pagesEruption of Palatal Canines Following Surgical Exposure: A Review of Outcomes in A Series of Consecutively Treated CasesAniket PotnisNo ratings yet
- Care Plan Presentation On Meningitis PatientDocument20 pagesCare Plan Presentation On Meningitis PatientDuop Jock LiemNo ratings yet
- Are The Effects? Note Convince The Panel That There Is A Need To Conduct The ResearchDocument5 pagesAre The Effects? Note Convince The Panel That There Is A Need To Conduct The ResearchRichmon SantosNo ratings yet
- Guide of Hypertensive Crisis PharmacotherapyDocument6 pagesGuide of Hypertensive Crisis PharmacotherapyAishah FarihaNo ratings yet
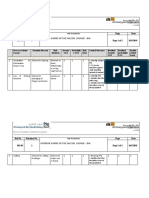
- 3 - Risk assemt.-DB & SMPDocument4 pages3 - Risk assemt.-DB & SMPAraf KalamNo ratings yet
- Immunology-1st Master QDocument20 pagesImmunology-1st Master QIslam Fathy El NakeepNo ratings yet
- Brosur LarutanDocument1 pageBrosur LarutanNingsihNo ratings yet
- Case 2 Acute Ischemic Stroke wk.6Document3 pagesCase 2 Acute Ischemic Stroke wk.6Nader AbdurasadNo ratings yet
- Transplantation of The Liver PDFDocument1,569 pagesTransplantation of The Liver PDFDiana Novac100% (1)
- BRAP PAMET Biosafety Guidance On COVID 19 Testing For Laboratorians EDocument179 pagesBRAP PAMET Biosafety Guidance On COVID 19 Testing For Laboratorians EMM ReyesNo ratings yet
- Praktikum Blok 18Document236 pagesPraktikum Blok 18Sherly MydoNo ratings yet
- A Comparison of Injuries in Elite Male and Female FootballDocument9 pagesA Comparison of Injuries in Elite Male and Female FootballAdrian RuizNo ratings yet
- Health TeamDocument5 pagesHealth TeamFahim AhmedNo ratings yet
- Vaers Data Use Guide: 1. Important Information About VAERSDocument17 pagesVaers Data Use Guide: 1. Important Information About VAERSMalu HadassaNo ratings yet
- Monograph On Lung Cancer July14Document48 pagesMonograph On Lung Cancer July14PatNo ratings yet
- Abortion Group AssignmentDocument26 pagesAbortion Group AssignmentJr Ajayi BNo ratings yet
- Democracy in The BalanceDocument180 pagesDemocracy in The BalanceJoe WigginsNo ratings yet
- Drugs Dilemmas and ChoicesDocument304 pagesDrugs Dilemmas and ChoicesClément JanequinNo ratings yet
- Epidemiology and Infection PreventionDocument32 pagesEpidemiology and Infection Preventionbkbaljeet116131No ratings yet
- Group B HypothyroidismDocument14 pagesGroup B HypothyroidismMari IllustriousNo ratings yet
- URTI and AnaesthesiaDocument6 pagesURTI and AnaesthesiaChuah Wei HongNo ratings yet
- Ferreira-Santos 2020 Artículo OriginalDocument10 pagesFerreira-Santos 2020 Artículo OriginalPaul SimononNo ratings yet
- Disorders of Sexual DevelopmentDocument19 pagesDisorders of Sexual DevelopmentJoanne May100% (1)
- Acne VulgarisDocument58 pagesAcne VulgarisNargisNo ratings yet
- iDA Case StudyDocument4 pagesiDA Case StudyKhizra AmjadNo ratings yet
- K.R.jolvisPou FermentationTheKeyStepintheProcessingDocument9 pagesK.R.jolvisPou FermentationTheKeyStepintheProcessingThuan DuongNo ratings yet