Professional Documents
Culture Documents
Hyponatremia - Annals of Internal Medicine 2015
Uploaded by
ntnquynhproOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Hyponatremia - Annals of Internal Medicine 2015
Uploaded by
ntnquynhproCopyright:
Available Formats
Annals of Internal Medicine䊛
In the Clinic®
Hyponatremia Prevention
H
yponatremia is the most common elec-
trolyte disorder in hospitalized patients. Diagnosis
Hospital-associated hyponatremia in-
cludes admission hyponatremia (community-
acquired hyponatremia) and hospital-acquired Treatment
hyponatremia. The reported incidence of
hospital-associated hyponatremia ranges be-
tween 10% and 30%, depending on the defini- Practice Improvement
tion, patient population, and case mix. It is asso-
ciated with increased mortality, hospital length
of stay, hospital costs, intensive care unit (ICU) Tool Kit
days, and chance of readmission (1). Acute on-
set or rapid correction of severe chronic cases
can cause extensive or fatal brain damage, but
Patient Information
even mild chronic cases can have adverse out-
comes, such as decreased cognition, osteopo-
rosis, increased risk for falls, and fractures (2).
The CME quiz is available at www.annals.org/intheclinic.aspx. Complete the quiz to earn up to 1.5 CME credits.
Physician Writer CME Objective: To review current evidence for prevention, diagnosis, treatment, and practice
Dan A. Henry, MD improvement for hyponatremia.
Funding Source: American College of Physicians.
Disclosures: Dr. Henry, ACP Contributing Author, has disclosed no conflicts of interest.
Disclosures can also be viewed at www.acponline.org/authors/icmje/ConflictOfInterestForms
.do?msNum=M14-2454.
With the assistance of additional physician writers, Annals of Internal Medicine editors
develop In the Clinic using resources of the American College of Physicians, including
ACP Smart Medicine and MKSAP (Medical Knowledge and Self-Assessment Program).
In the Clinic does not necessarily represent official ACP clinical policy. For ACP clinical
guidelines, please go to https://www.acponline.org/clinical_information/guidelines/.
© 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Patients with no underlying dis- vasopressin (AVP), when plasma
ease can maintain normal plasma sodium levels fall below 135
sodium levels. Levels are deter- mEq/L. Hyponatremia develops if
mined by the total exchangeable more water is ingested than can
extracellular sodium and intracel- be excreted by the kidneys or if
lular potassium divided by total the ability to excrete a large vol-
body water. Hyponatremia is a ume of dilute urine is compro-
disorder of water balance. The mised because of kidney disease,
ability to excrete dilute urine al- diuretics, low protein intake, or the
lows people without any underly- presence of AVP. The amount of
ing disease to drink large amounts
free water excreted is determined
1. Amin A, Deitelzweig S, of water (nearly a liter an hour)
Christian R, et al. Evalua- by urine volume, sodium, and po-
tion of incremental health-
without becoming hyponatremic.
care resource burden and Maintenance of water balance re- tassium. If the sum of urinary so-
readmission rates associ-
quires normally functioning kid- dium and potassium is less that of
ated with hospitalized
hyponatremic patients in neys; sufficient urine urea (the plasma sodium, free water is ex-
the US. J Hosp Med.
2012;7:634-9. [PMID: end-product of protein metabo- creted (3). A complete overview of
22961813] lism); and suppressed secretion of sodium and water balance can be
2. Renneboog B, Musch W,
Vandemergel X, et al. the antidiuretic hormone, arginine found elsewhere (4).
Mild chronic hyponatre-
mia is associated with
falls, unsteadiness, and
attention deficits. Am J
Med. 2006;119:71.e1-8.
[PMID: 16431193]
Prevention
3. Rose BD, Post TW. Clinical Who is at risk for Diuretics impair the kidney's ability
Physiology of Acid-Base
and Electrolyte Disorders, hyponatremia? to excrete dilute urine. Thiazides
5th ed. New York: Up to 13% of individuals partici- are a particularly common cause of
McGraw-Hill: 2001; 699.
4. Eaton DC, Pooler JM. pating in endurance exercise hyponatremia—30% of thiazide-
Vander's Renal Physiol-
ogy, 8th ed. McGraw-Hill, (marathons and triathlons) de- treated patients develop hypona-
New York: McGraw-Hill; velop hyponatremia, which can tremia over 10 years (7). In 1 study
2013.
5. Almond CS, Shin AY, For- be severe (<120 mEq/L) when of patients who became hypona-
tescue EB, et al. Hypona-
tremia among runners in water intake exceeds water loss tremic after receiving thiazides, the
the Boston Marathon. N (5). Institutionalized patients with electrolyte disturbance developed
Engl J Med. 2005;352:
1550-6. [PMID: schizophrenia can become hy- within 2 weeks in approximately
15829535]
6. Kovesdy CP, Lott EH, Ju ponatremic, despite an intact two thirds of cases and within 5
JL, et al. Hyponatremia, ability to excrete maximally dilute days in half (8). In another study,
hypernatremia, and mor-
tality in patients with urine, after rapidly ingesting patients developed hyponatremia
chronic kidney disease after a median of 116 days (9). El-
with and without conges- large quantities of water. People
tive heart failure. Circula- who consume large quantities of derly patients as well as those with
tion. 2012;125:677-84.
[PMID: 22223429] fluid but little protein (beer poto- low body weight and hypokalemia
7. Leung AA, Wright A, Pazo have an increased risk for thiazide-
V, et al. Risk of thiazide- mania, or tea and toast diet) may
induced hyponatremia in also become hyponatremic, be- associated hyponatremia (9).
patients with hyperten-
sion. Am J Med. 2011; cause decreased excretion of Other drugs can interfere with the
124:1064-72. [PMID: ability to dilute the urine, most
22017784] urea results in limited water ex-
8. Chow KM, Kwan BC, Szeto cretion even when urine osmolal- commonly selective serotonin re-
CC. Clinical studies of
thiazide-induced hypona- ity is < 100 mOsm/kg. uptake inhibitors (SSRIs), selective
tremia. J Natl Med Assoc. norepinephrine reuptake inhibi-
2004;96:1305-8. [PMID:
15540881] Patients with severe kidney dis- tors (SNRIs), carbamazepine, and
9. Chow KM, Szeto CC, ease are unable to increase urine
Wong TY, et al. Risk factors oxcarbazepine. Hyponatremia
for thiazide-induced hy- water loss and are susceptible to develops in 0.5%–30% of pa-
ponatraemia. QJM. 2003;
96:911-7. [PMID: hyponatremia. tients receiving SSRIs and
14631057]
10. Wilkinson TJ, Begg EJ, SNRIs, usually within 2 weeks.
In a study of patients with chronic kidney disease
Winter AC, et al. Inci- Elderly patients, those who had
dence and risk factors for and a mean estimated glomerular filtration rate
hyponatraemia following (GFR) of 50.2 ± 14.1 mL/min/1.73 m2, preva- previous episodes of hypona-
treatment with fluoxetine
or paroxetine in elderly lence of hyponatremia was 13.6% at baseline tremia, and patients receiving
people. Br J Clin Phar-
macol. 1999;47:211-7.
and 26% of patients had >1 episode of hypona- concurrent thiazide treatment
[PMID: 10190657] tremia during a follow-up period of 5.5 years (6). are at increased risk (10).
姝 2015 American College of Physicians ITC2 In the Clinic Annals of Internal Medicine 4 August 2015
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
The ability to excrete water is What potential measures can
also limited when the posterior prevent or limit the severity of
pituitary continues to secrete hyponatremia?
AVP despite a low plasma so- Clinicians should encourage run-
dium concentration. AVP is se- ners to drink fluids only when
creted without an osmotic stimu-
they have increased thirst and to
lus if circulation is inadequate, as
monitor their body weight to
in patients with hypovolemia or
avoid weight gain during exer-
heart or liver disease. “Inappro-
cise. Plasma sodium levels
priate secretion” of AVP occurs in
the absence of both osmotic and should be checked 1–2 weeks
hemodynamic stimulus. Affected after initiation of thiazide, SNRI,
patients have the syndrome of and SSRI therapy, especially in
inappropriate antidiuretic hor- patients at high risk for hypona-
mone secretion (SIADH). Hypo- tremia. Thiazides should be
natremia due to SIADH is com- avoided in persons with high
mon in hospitalized patients fluid or low protein intake and
because AVP is released in re- during acute illness.
sponse to hypoxia, pain, or
Plasma sodium levels should be
stress. Patients at particularly
high risk include postsurgery pa- measured in all hospitalized pa-
tients, elderly persons, persons tients on admission; low sodium
admitted to the intensive care levels should be treated based
unit, and patients with central on the underlying cause. Hypo-
nervous system disorders. Finally, tonic fluids and thiazide diuret-
hyponatremia is especially com- ics should be avoided, espe-
mon among hospitalized chil- cially in patients at increased
dren receiving hypotonic fluids, risk for hyponatremia. Clinicians
and fewer patients develop hy- should monitor daily plasma
ponatremia if isotonic saline sodium levels in patients with
rather than hypotonic saline is hyponatremia or in those at in-
used to treat gastroenteritis (11). creased risk.
Prevention... Hyponatremia is common in patients participating in en-
durance exercise and those receiving thiazides, SSRIs, or SNRIs. Elderly
patients; those with congestive heart failure, cirrhosis, or pneumonia;
and persons admitted to the ICU are at increased risk for hospital-
acquired hyponatremia. Hypotonic fluids should be avoided in
hospitalized patients at increased risk.
CLINICAL BOTTOM LINE
Diagnosis 11. Neville KA, Verge CF,
Rosenberg AR, O’Meara
What characteristic symptoms sciousness; seizures; and, rarely, MW, et al. Isotonic is
better than hypotonic
or physical findings should cardiorespiratory arrest). Nota- saline for intravenous
rehydration of children
alert clinicians to the diagnosis bly, mild chronic hyponatremia with gastroenteritis: a
of hyponatremia? (plasma sodium 125–135 mEq/L) prospective randomised
study. Arch Dis Child.
may cause subtle neurocognitive 2006;91:226-32. [PMID:
Hyponatremic patients can be deficits that can only be detected 16352625]
12. Bartter FC, Schwartz WB.
asymptomatic or have symptoms by careful testing; these deficits The syndrome of inap-
that are moderate (nausea, con- propriate secretion of
improve when the plasma so- antidiuretic hormone.
fusion, headache, vomiting) or dium is normalized (12). Because Am J Med. 1967;42:
790-806. [PMID:
severe (delirium; impaired con- hyponatremic patients are at risk 5337379]
4 August 2015 Annals of Internal Medicine In the Clinic ITC3 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
for osteoporosis, falls, and hip mia are usually clinically euvo-
Table 1. Major Causes of Hypona-
fractures, it should be considered lemic (see next section). CSW is
tremia Based on Volume Status
in the differential diagnosis of uncommon and can be difficult
Hypovolemia these conditions (2). to differentiate from SIADH. Con-
Extrarenal losses ditions associated with CSW in-
Vomiting
What conditions should
clude head injury, subarachnoid
Diarrhea clinicians consider when
hemorrhage, meningitis, enceph-
Pancreatitis evaluating patients with alitis, and central nervous system
Sweating hyponatremia? tumors or surgery. Patients with
Small bowel obstruction Hyponatremia can occur when CSW have urinary loss of sodium
Renal losses release of AVP is physiologically and water due to a proximal so-
Osmotic diuresis appropriate, due to decreased dium reabsorption deficit (also
Cerebral salt wasting effective circulating volume, or decreased reabsorption of urea
Salt-losing nephritis inappropriate (that is, no physio- and uric acid). Because it is often
Diuretics logic reason). Urine volume de- difficult to assess volume status in
Addison disease creases in response to the release postneurosurgery patients in the
of AVP, and hyponatremia will de- ICU, finding a significant negative
Euvolemia velop if water intake exceeds uri- fluid balance on reviews of the
Primary polydipsia nary and insensible losses of wa- chart—Intake/Output—may indi-
Decreased solute excretion ter. Patients are typically classified cate CSW. In these patients,
Diuretics based on their total body sodium
Hypothyroidism
volume depletion leads to non-
as hypovolemic, euvolemic, and
Cortisol deficiency
osmotic release of AVP and sub-
hypervolemic (Table 1).
Syndrome of inappropriate
sequent water retention. Similar
antidiuretic hormone secretion Hypovolemic hyponatremia to patients with SIADH, patients
Patients with hypovolemic hypo- with CSW have decreased serum
Hypervolemia natremia have a loss (renal or ex- levels of sodium and increased
Heart failure trarenal) of sodium and/or potas- urinary sodium and osmolality.
Liver disease with cirrhosis sium and water.
Nephrotic syndrome A rare but important cause of
Chronic kidney disease Extrarenal sodium losses can occur hypovolemic hyponatremia is
with excessive sweating, pancreati- primary adrenal insufficiency
tis, small bowel obstruction, vomit- (loss of mineralocorticoids and
ing, and diarrhea. If these losses glucocorticoids, also known as
are not replaced, they lead to de- Addison disease). Primary adre-
creased effective circulating vol- nal insufficiency leads to renal
ume and nonosmotic release of sodium wasting with subsequent
AVP. Hypovolemic hyponatremia volume depletion, causing non-
caused by diarrhea or third-space osmotic release of AVP. Lack of
loss results in low urine sodium cortisol also increases AVP re-
levels due to increased renal so- lease (see isolated glucocorticoid
dium reabsorption. Hypovolemia deficiency in euvolemic hypona-
caused by gastric losses of tremia). Patients with Addison
hydrochloric acid results in low disease typically present with hy-
urine chloride due to increased povolemia; hyponatremia; hyper-
renal chloride reabsorption, but kalemia; decreased bicarbonate;
urine sodium may not be low be- and increased urine sodium, an
cause of metabolic alkalosis and inappropriate renal response in
resulting bicarbonaturia. the setting of volume depletion.
However, not all patients with
Renal sodium losses occur with
primary adrenal insufficiency
glycosuria, cerebral salt wasting
have this classic presentation.
(CSW), primary adrenal insuffi-
13. Nerup J. Addison's ciency, and diuretics. Loop di- In a study of 102 patients with Addison dis-
disease-clinical studies. A
report of 108 cases. Acta uretics can cause hypovolemic ease, 88% were hypotensive (systolic blood
Endocrinol. 1974;76: hyponatremia, but patients with
127-41. [PMID:
pressure < 110 mm Hg), 12% were ortho-
4609691] thiazide-associated hyponatre- static, and only 66% were hyperkalemic (13).
姝 2015 American College of Physicians ITC4 In the Clinic Annals of Internal Medicine 4 August 2015
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Euvolemic hyponatremia
Table 2. Criteria for the Diagnosis of SIADH
Euvolemic hyponatremia occurs
when total body sodium content Essential
is either normal or slightly de- Decreased effective osmolality of the extracellular fluid (plasma osmolality
creased while total body water is <275 mOsm/kg H2O)
increased. Causes include Inappropriate urine concentration (urine osmolality >100 mOsm/kg H2O with
normal renal function) in the presence of decreased effective serum osmolality
SIADH, diuretic use, chronic kid-
Clinical euvolemia, as defined by the absence of signs of hypovolemia
ney disease, decreased solute (orthostasis, tachycardia, decreased skin turgor, dry mucous membranes) or
intake, primary polydipsia, gluco- hypervolemia (subcutaneous edema, ascites)
corticoid and thyroid deficiency, Absence of urinary sodium conservation (i.e., urine sodium <30 mmol/L) when
salt and water intake are normal
and reset osmostat.
Absence of other potential causes of euvolemic hypoosmolality: hypothyroidism,
SIADH is the most common hypocortisolism (pituitary ACTH insufficiency), and diuretic use
cause of euvolemic hyponatre-
Supplemental
mia. Patients with this syndrome
Plasma uric acid <4 mg/dL
have a decrease in total body
Blood urea nitrogen <10 mg/dL
sodium and an increase in total
Fractional sodium excretion >1%; fractional urea excretion >55%
body water resulting in clinical
Abnormal water load test (inability to excrete at least 90% of a 20 mL/kg water
euvolemia, but they have labora- load in 4 hours, failure to dilute urine osmolality to <100 mOsm/kg H2O, or
tory findings (decreased uric acid both)
and blood urea nitrogen [BUN]– Plasma AVP level inappropriately elevated relative to plasma osmolality
creatinine ratio) consistent with No significant correction of plasma sodium with volume expansion but
slight hypervolemia (12). Table 2 improvement after fluid restriction
presents criteria for diagnosis of ACTH = adrenocorticotrophic hormone; AVP = arginine vasopressin; SIADH = syndrome
SIADH. SIADH cannot be diag- of inappropriate secretion of antidiuretic hormone.
nosed in patients who are receiv-
ing diuretics (particularly thiazide Although some studies indicate
diuretics) or those who have se- that chlorthalidone treatment is
vere hypothyroidism or isolated associated with fewer cardio-
glucocorticoid insufficiency (sec- vascular events than hydrochlo-
ondary adrenal insufficiency). It is rothiazide (HCTZ), the former is
common in hospitalized patients more likely to cause hyponatre-
and patients treated with SSRIs mia. A recent study confirmed
and SNRIs (10). Table 3 presents that hyponatremia occurs more
common causes of SIADH. often when chlorthalidone is
prescribed in the same dose as
Diuretics commonly cause hypo- HCTZ; however, when the dose
natremia; thiazides are more of- of chlorthalidone is half of the
ten associated with hyponatre- HCTZ dose (12.5 mg vs. 25 mg),
mia than loop diuretics because there is no difference in the in-
unlike loop diuretics, thiazides cidence of hyponatremia (15).
impair the ability to excrete dilute
urine while preserving the ability Chronic kidney disease can cause 14. Rodenburg EM, Hoorn
EJ, Ruiter R, et al.
to concentrate the urine. Most euvolemic and hypervolemic hy- Thiazide-associated hypo-
patients with thiazide-induced ponatremia. Patients with chronic natremia: a population-
based study. Am J Kid-
hyponatremia are euvolemic kidney disease have a decreased ney Dis. 2013;62:67-72.
[PMID: 23602191]
(similar to SIADH). They initially ability to dilute and concentrate 15. Van Biijderveen JC,
lose sodium but are able to main- urine, and urine osmolality is often Straus SM, Rodenburg
EM, et al. Risk of hypona-
tain sodium balance with pro- fixed, which limits the ability to in- tremia with diuretics:
longed treatment. crease free water excretion (16). chlorthalidone versus
hydrochlorothiazide. Am
Kidney function must be normal J Med. 2014;127:
763-71 [PMID:
In a population-based study, 32.4% of patients for a diagnosis of SIADH. 24811554]
who developed hyponatremia had received 16. Tannen RL, Regan EM,
thiazides; exposure to thiazides was associated Primary polydipsia is an unusual Dunn MJ. Vasopressin-
resistant hyposthenuria
with a 5-fold greater risk for hyponatremia cause of hyponatremia; most pa- in advanced chronic
tients with polydipsia have psychi- renal disease. N Engl J
than a comparison group with no exposure Med. 1969;280:1135.
(hazard ratio, 4.95 [95% CI, 4.12–5.96]) (14). atric disease, particularly acute [PMID: 5782121].
4 August 2015 Annals of Internal Medicine In the Clinic ITC5 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Exercise-associated hyponatre-
Table 3. Common Causes of SIADH
mia is an acute type of hypona-
Tumors tremia seen after vigorous endur-
Pulmonary/mediastinal (small cell carcinoma, mesothelioma, thymoma) ance exercise that occurs with
Nonchest carcinomas (duodenal, stomach, pancreatic, ureteral, prostate, excessive fluid intake in the pres-
bladder, uterine, nasopharyngeal) ence of increased AVP secretion.
Lymphoma
Ewing sarcoma Isolated glucocorticoid deficiency
caused by lack of adrenocortico-
Central nervous system disorders trophic hormone (ACTH) results in
Mass lesions (tumors, brain abscesses, subdural hematoma) hyponatremia because cortisol is
Inflammatory diseases (encephalitis, meningitis, systemic lupus, acute required to inhibit AVP secretion.
intermittent porphyria, multiple sclerosis) Aldosterone secretion is not
Degenerative/demyelinative diseases (Guillain-Barré syndrome, spinal cord affected because the renin–
lesions)
angiotensin–aldosterone system
Miscellaneous (subarachnoid hemorrhage, head trauma, acute and chronic
psychosis, delirium tremens, pituitary stalk section, transsphenoidal and levels of potassium control its
adenomectomy, hydrocephalus, cerebrovascular accident, cavernous sinus release. An ACTH stimulation test
thrombosis)
can diagnose secondary adrenal
insufficiency, but results can be
Drug-induced
normal in patients with recent loss
Stimulated AVP release (narcotics, nicotine, phenothiazines, tricyclics)
of ACTH.
Direct renal effects, potentiation of AVP antidiuretic effects (desmopressin,
oxytocin, prostaglandin synthesis inhibitors), or both Reset osmostat is a condition in
Mixed or uncertain actions (carbamazepine and oxcarbazepine, chlorpropamide, which the serum osmolality re-
clofibrate, clozapine, cyclophosphamide, ifosfamide, 3,4-methylenedioxy-
methamphetamine [“ecstasy”], serotonin reuptake inhibitors, vincristine) quired to stimulate the release of
AVP is shifted to a lower serum
Pulmonary diseases osmolality. This condition has
Infections (tuberculosis, acute bacterial and viral pneumonia, pulmonary abscess, been described in patients with
aspergillosis, emphysema) quadriplegia, tuberculosis,
Mechanical/ventilatory (acute respiratory failure, asthma, COPD, positive chronic malnutrition, and psycho-
pressure ventilation)
sis and should be considered in a
patient who is diagnosed with
Other
SIADH but has stable plasma so-
Rocky Mountain spotted fever
dium levels. The diagnosis is made
AIDS and early symptomatic HIV infection
by administering a water load to
Nausea, pain, stress
the patient. In contrast to those
Prolonged strenuous exercise (marathon, triathlon, ultramarathon, hot-weather
hiking) with SIADH, patients with reset
Mutations of the aquaretic vasopressin receptor osmostat are able to excrete free
Idiopathic water and reduce urine osmolality.
AVP = arginine vasopressin; COPD = chronic obstructive pulmonary disease; SIADH = Hypervolemic hyponatremia
syndrome of inappropriate secretion of antidiuretic hormone. Conditions associated with hyper-
volemic hyponatremia include
psychosis with schizophrenia. heart failure, cirrhosis with ascites,
They can develop hyponatremia chronic kidney disease, and the
through rapid ingestion of large nephrotic syndrome. Patients with
amounts of fluid that exceed the the former two conditions have a
kidney's ability to excrete the vol- decreased effective circulating
ume. Other factors that can con- volume. In patients with cirrhosis,
tribute to hyponatremia in these decreased effective circulating
patients include volume depletion volume is a result of arterial vaso-
causing increased urine osmolality dilation of the splanchnic circula-
17. Goldman MB, Luchins
DJ, Robertson GL. Mech- and decreased solute excretion; tion, which is probably due to in-
anism of altered water drugs known to cause SIADH; de- creased endothelial release of ni-
metabolism in psychotic
patients with polydipsia creased solute intake; and acute tric oxide. Patients with the
and hyponatremia. N psychosis, which itself causes an nephrotic syndrome have edema
Engl J Med. 1988;318:
397. [PMID: 3340117] increase in AVP release (17). usually due to primary sodium re-
姝 2015 American College of Physicians ITC6 In the Clinic Annals of Internal Medicine 4 August 2015
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
tention that results in overfilling of osmoles in plasma, osmolality is
the intravascular volume. calculated using the following
formula:
What is the overall approach to
the diagnosis of hyponatremia? (mOsm/kg H2O) = 2 × serum
Two papers have highlighted the [Na+] (mmol/L) + glucose (mg/
difficulties in identifying the dL)/18 + BUN (mg/dL)/2.8
cause of hyponatremia.
Hyponatremia due to increased
In the first study, 121 consecutive patients pre- plasma osmolality (>295 mOsm/
senting with plasma sodium levels <130 kg H2O) occurs when high con-
mEq/L were evaluated by an inexperienced
centrations of effective solutes
physician using an established algorithm, by a
senior physician, and by a senior endocrinolo-
increase the extracellular osmola-
gist who acted as the reference standard. The lity. As a result, intracellular water
agreement between algorithm and senior phy- moves into the extracellular fluid,
sician with the reference standard was 71% thus diluting the plasma sodium.
and 32%, respectively. The main diagnostic Hypertonic hyponatremia occurs
problem was SIADH, which was often diag- most commonly with hyperglyce-
nosed incorrectly before hypothyroidism and mia. Misdiagnosis can be
secondary adrenal insufficiency were ruled out avoided by correcting the plasma
(18).
sodium by a factor of 1.6 mEq/L
In the second study, physicians attempted to for each 100-mg/dL increase in
diagnose challenging cases of hyponatremia plasma glucose levels, if glucose
using 10 clinical diagnostic algorithms. The is < 400 mg/dL. A correction fac-
correct diagnosis in the 3 cases by any of the tor of 2.4 mEq/L should be used
10 algorithms was only 6%–12%. The primary if glucose level is > 400 mg/dL
obstacle was that 8 of 10 algorithms used as-
(20). Solutes that freely permeate
sessment of volume status as an important
variable; other problems were failure to rule
cell membranes (urea, alcohol,
out secondary adrenal insufficiency before and methanol) can also increase
making the diagnosis of SIADH and diagnos- plasma osmolality and should be
ing primary polydipsia based on urinary osmo- considered when plasma osmo-
lality <100 mOsm/kg H2O but not considering lality is being calculated. The cor-
decreased solute excretion (19). rection factors are as follows:
BUN (mg/dL), 1/2.8; ethanol
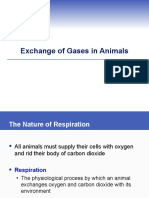
The Figure describes an approach
(mg/dL), 1/4.6; and methanol
to the diagnosis of hyponatremia.
(mg/L), 1/32.
As part of the initial evaluation,
clinicians should measure the pa- Pseudohyponatremia is charac-
tient's plasma osmolality, glucose, terized by normal plasma osmo-
urea, creatinine, and potassium. lality (275–295 mOsm/kg H2O)
Urine should be measured for os- and occurs when there is marked
molality, sodium, and chloride (if elevation of plasma lipids, pro- 18. Fenske W, Maier SK,
the patient is vomiting). Appendix teins, or both. The concentration Blechschmidt, et al.
Utility and limitations of
Figures 1 through 3 (available at of sodium per liter of plasma wa- the traditional diagnostic
www.annals.org) show further di- approach to hyponatre-
ter is unchanged; however, the mia: a diagnostic study.
agnostic workups based on the Am J Med. 2010;123:
concentration of sodium per liter 652-59. [PMID:
results of the initial evaluation.
of plasma overall is decreased 20609688]
19. Hoorn EJ, Halperin ML,
Measurement of plasma osmolal- because of the increased relative Zietse R. Diagnostic ap-
proach to a patient with
ity can help distinguish whether proportion occupied by lipids or hyponatremia: tradi-
the patient has true hyponatre- protein. The measured plasma tional versus physiology-
based options. QJM.
mia, pseudohyponatremia as a osmolality is not affected. Pseudo- 2005;98:529-40. [PMID:
hyponatremia can also be seen in 15955797]
result of hyperlipidemia or hyper- 20. Hillier TA, Abbott, RD,
proteinemia, or hypertonic hy- patients who have transurethral Barrett, EJ. Hyponatre-
mia: evaluating the
ponatremia due to elevated resection of the prostate and ab- correction factor for hy-
glucose. Because sodium, glu- sorption of variable amounts of perglycemia. Am J Med.
1999;106:399-403.
cose, and BUN are the major glycine or sorbitol. [PMID: 10225241]
4 August 2015 Annals of Internal Medicine In the Clinic ITC7 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Figure. Approach to the diagnosis of hyponatremia.
PNa < 136 mEq/L
Hypotonicity* Measure plasma
<275 mOsm/kg osmolality, urea,
and glucose
Measure Uosm , Normotonicity Hypertonicity with
275–295 mOsm/kg osmotically active
UNa, Ucl†
Hyperlipidemia solutes present
Hyperproteinemia > 295 mOsm/kg
Glycine Glucose
Mannitol
Glycine
Uosm < 100 Uosm 100–200 Uosm > 200
mOsm/kg mOsm/kg‡ mOsm/kg
Polydipsia Consider High probabiity Clinical
Decreased solute excertion Polydipsia Hypervolemia
of hypovolemia euvolemia
Beer potomania Decreased solute
Tea and toast diet excretion
Beer potomania
Tea and toast diet
Appendix Figure 1§ Appendix Figure 2§ Appendix Figure 3§
* After correcting for any ineffective osmoles (urea, alcohol).
† If patient is vomiting, measure UCl.
‡ If Uosm > 100 or <200 mOsm/kg, need to rule out the syndrome of inappropriate antidiuretic hormone secretion.
§ Available at www.annals.org.
If plasma osmolality is low (< 275 If urine osmolality is >200 mOsm/
mOsm/kg H2O) after increased kg H2O, the patient is not receiv-
urea and glucose are corrected ing diuretics, and kidney function
for, the patient has hypotonic is normal, then AVP is playing an
hyponatremia, the most common etiologic role. To determine the
form of hyponatremia. cause of AVP secretion, the next
step is to classify the patient's
What is the role of volume volume status on the basis of
status, urine osmolality, and the history and physical exami-
nation. Volume status is typi-
urinary sodium in the
cally classified into 3 categories:
evaluation of patients with hypovolemia, clinical euvol-
hyponatremia? emia, or hypervolemia.
If the patient has hypotonic hy-
ponatremia, the next step is to Patients with hypovolemic hypo-
measure urine osmolality (Fig- natremia are further subdivided
ure). If urine osmolality is < 100 into whether they are experienc-
ing extrarenal or renal sodium
mOsm/kg H2O, then polydipsia
losses. If extrarenal losses are
or decreased solute excretion is
likely (due to vomiting, diarrhea,
usually the cause. Urine osmola- pancreatitis, and small bowel ob-
lity <100 mOsm/kg H2O may struction), urinary studies should
also be found after volume re- show low sodium (< 30 mEq/L)
suscitation of patients with hy- and increased osmolality. One
povolemic hyponatremia if os- exception is vomiting patients; in
molality is measured after the these cases, urinary sodium
administration of isotonic could be > 30 mEq/L but urinary
saline. chloride will be < 30 mEq/L. Re-
姝 2015 American College of Physicians ITC8 In the Clinic Annals of Internal Medicine 4 August 2015
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
nal sodium losses occur with di- In patients with hypervolemia due
uretic use, primary adrenal insuf- to heart failure, cirrhosis, or the
ficiency, salt-losing nephritis, and nephrotic syndrome, the diagnosis
CSW. In these patients, urinary is usually based on history and
sodium will be > 30 mEq/L. physical examination. The urinary
sodium should be < 30 mEq/L in
Clinical euvolemia can be difficult
these patients unless they are re-
to differentiate from mild hypo-
ceiving diuretics.
volemia. Even with a history sug-
gestive of sodium loss (e.g., diar- What is the role of imaging
rhea), water retention may make studies in the diagnosis of
the patient seem euvolemic. In hyponatremia?
these cases, measurement of uri-
nary sodium can be very useful in Patients with unexplained
differentiating between hypovo- SIADH should have imaging
lemia and euvolemia. Urinary so- studies to identify the potential
dium level < 30 mEq/L has 63%– underlying cause. All patients
80% sensitivity and 72%–100% should have chest radiography,
specificity for hypovolemia, and clinicians should consider
whereas urinary sodium >30 ordering chest computed to-
mEq/L has 87%–100% sensitivity mography in smokers. Magnetic
and 52%– 83% specificity for euv- resonance imaging of the brain
olemia (21–22). Administration of is indicated if neurologic
normal saline as a diagnostic test abnormalities are found on
may be necessary in patients with physical examination after
urinary sodium < 20 and > 20 plasma sodium has been
mEq/L or < 40 mEq/L to distin- normalized.
guish between hypovolemic hy-
When should clinicians consult
ponatremia and SIADH, with co-
existent salt depletion. Patients a nephrologist or an
with salt-depleted SIADH do not endocrinologist?
normalize plasma sodium after Clinicians should consult with a
administration of normal saline; nephrologist or endocrinologist
urine osmolality remains high, if the cause of hyponatremia is
and the administered sodium is unknown and if guidance is
excreted in the urine. By contrast, needed for the appropriate evalu-
hypovolemic hyponatremia im- ation of SIADH. These specialists
proves after administration of can also give advice on the use of
normal saline; the urine osmolal- normal saline in patients with pos-
ity decreases, and urinary sodium sible SIADH and plasma sodium
does not increase until the pa- levels < 120 mEq/L.
tient becomes euvolemic.
21. Chung HM, Kluge R,
Diagnosis... Identifying the cause of hyponatremia can be challenging Schrier RW, et al. Clinical
assessment of extracellu-
because it is often difficult to distinguish whether the patient is slightly lar fluid volume in hypo-
volume depleted or euvolemic. In patients for whom volume status is natremia. Am J Med.
uncertain, saline infusion may be useful. Before SIADH is diagnosed, the 1987;83:905-8. [PMID:
3 674097]
thiazide treatment must be stopped to determine the effect on plasma 22. Musch W, Thimpont J,
sodium and to rule out secondary adrenal insufficiency and Vandervelde D, et al.
Combined fractional
hypothyroidism. excretion of sodium and
urea better predicts re-
sponse to salaine in
hyponatremia than do
CLINICAL BOTTOM LINE usual clinical and bio-
chemical parameters. Am
J Med. 1995;99:348-55.
[PMID: 7573088]
4 August 2015 Annals of Internal Medicine In the Clinic ITC9 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Treatment
What is the overall approach to tremia as 130 –135 mEq/L, moder-
treatment of hyponatremia? ate as 125–129 mEq/L, and severe
The overall approach to hypona- as < 125 mEq/L (24).
tremia treatment depends on acu- How rapidly should sodium
ity, severity, and cause. Hyponatre-
levels be corrected in acute and
mia is “acute” if the duration is
severely symptomatic
known to be < 48 hours and
“chronic” if the duration is un- hyponatremia, and how should
known or > 48 hours. Endurance they be monitored?
exercise with water intoxication, In patients with acute hyponatre-
psychogenic polydipsia, use of mia or severely symptomatic
such drugs as 3, 4-methyle- chronic hyponatremia (altered
dioxymethamfetamine (ecstasy), mental status, seizures, and fre-
colonoscopy preparation, and quent vomiting), it is important to
postoperative states are associ- rapidly reverse cerebral edema by
ated with acute hyponatremia. increasing plasma sodium by 5
Acute hyponatremia can be char- mEq/L. On the other hand, in pa-
acterized by swelling of brain cells tients with chronic hyponatremia,
and can lead to cerebral edema the plasma sodium level should
with risk for brain herniation. Thus, not be raised > 10 mEq/L within
patients with acute hyponatremia 24 hours and/or > 18 mEq/L within
require urgent normalization of 48 hours. These are limits that
sodium levels. Over 24 – 48 hours, should not be exceeded rather
the brain can adapt to hyponatre- than goals of therapy. Because it is
mia by losing organic solutes, easy to “overshoot the mark” (see
which allows intracellular osmolal- below), the goal of therapy should
ity to equal plasma osmolality with- be set well below the therapeutic
out a large increase in brain cell limit. Recommended rates of cor-
water. After 48 hours, this loss of rection in patients with chronic
solutes predisposes patients with hyponatremia at high risk for
chronic hyponatremia to brain osmotic demyelination are 4 – 6
damage if hyponatremia is cor- mEq/L per day.
rected too rapidly.
Guidance for the treatment of hos-
The severity of hyponatremia is pitalized patients with acute and
typically classified as mild, moder- chronic symptomatic hyponatre-
ate, or severe. Guidelines released mia, including monitoring of
by professional societies have plasma sodium, is presented in
some minor differences in the so- Table 4. It is primarily based on
dium levels associated with these the European recommendations
categories. In 2013, a recommen- (24) as well as U.S. expert panel
dations from a U.S.-based expert recommendations whenever there
panel classified mild hyponatremia are significant differences (23).
23. Verbalis JG, Goldsmith
SR, Greenberg A, et al. as 130 –135 mEq/L, moderate as
Diagnosis, evaluation,
120 –129 mEq/L, and severe as Data on outcomes of 56 patients with plasma so-
and treatment of hy-
ponatremia:expert panel < 120 mEq/L (23). In 2014, a clini- dium levels ≤ 105 mmol/L were obtained from
recommendations. Am J members of the American Society of Nephrology.
Med. 2013;126:S1-42. cal practice guideline on diagnosis
Increased chronicity of hyponatremia and a high rate
[PMID: 24074529] and treatment of hyponatremia
24. Spasovski G, Vanholder of correction in the first 48 hours of treatment were
R, Allolio B, et al. Hypo- from the European Society of En- significantly associated with complications. No neu-
natremia Guideline De-
velopment Group. Clini-
docrinology, the European Society rologic complications were observed among pa-
cal practice guideline on of Intensive Care Medicine, and tients corrected by < 12 mmol/L per 24 hours, or
diagnosis and treatment
of hyponatremia. Eur J the European Renal Association– by < 18 mmol/L per 48 hours. In this cohort of pa-
Endocrinol. 2014;170: European Dialysis and Transplant
G1-G47. [PMID:
tients with severe chronic hyponatremia, neurologic
24074529] Association classified mild hypona- complications—which were probably secondary to
姝 2015 American College of Physicians ITC10 In the Clinic Annals of Internal Medicine 4 August 2015
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Table 4. Treatment of Hospitalized Patients With Hyponatremia, According to Symptoms
Severe (cardiorespiratory arrest, Administer 150 mL 3% saline over 20 min, then check plasma sodium levels while
seizures, deep somnolence, repeating the infusion of hypertonic saline over 20 min; continue 3% saline with target of
and coma) 5-mEq/L increase in plasma sodium, then stop hypertonic saline
Expert panel: 100 mL of 3% saline infused over 10 min x 3 as needed with urgent
correction 4–6 mEq/L
Do not increase plasma sodium more than 10 mEq/L in 24 h and in the next 24 h greater
than 8 mEq/L
For the first 24 h, monitor plasma sodium levels every 6 h depending on changes; when
stable, measure levels every 24 h
No improvement Continue 3% saline aiming for an additional 1-mEq/L/h increase in plasma sodium
Stop 3% saline infusion when symptoms improve, plasma sodium levels increases
10 mEq/L, or it reaches 130 mEq/L, whichever occurs first
Monitor plasma sodium every 4 h for the duration of hypertonic saline infusion, then every
6 h for the first 24 h; when stable, measure plasma sodium every 24 h
Acute hyponatremia without If acute, decrease in plasma sodium >10 mEq/L infuse 150 mL 3% saline over 20 min
severe or moderately severe Expert panel: Mild to moderate symptoms with a low risk of herniation, 3% hypertonic
symptoms saline infused at 0.5–2 mL/kg/h
Monitor plasma sodium after 4, 12, and 24 h; when stable measure plasma sodium every
24 h
Moderately severe (nausea Immediate treatment with 150 mL 3% hypertonic saline over 20 min; aim for a 5- mEq/
confusion, headache, L/24 h increase but limit plasma sodium to a 10-mEq/L increase in the first 24 h and 8
vomiting) mEq/L during every 24 h thereafter until plasma sodium reaches 130 mEq/L
Check plasma sodium levels after 1, 6, and 12 h
Expert panel: No indication for hypertonic saline; minimum correction of plasma sodium
by 4–8 mEq/L per day with a lower goal of 4–6 mEq/L per day if risk for ODS is high;
limits should not exceed 8 mEq/L in any 24-h period if risk for ODS is high
Chronic hyponatremia without Stop nonessential fluids, medications, and other factors that can contribute to or provoke
severe or moderately severe hyponatremia
symptoms Do not treat with the sole aim of increasing the plasma sodium
Avoid an increase in plasma sodium >10 mEq/L during the first 24 h and >8 mEq/L during
each 24 h thereafter
Monitor plasma sodium every 6 h until the plasma sodium stabilizes
Overrapid correction Overcorrection of hyponatremia is a medical emergency. In most cases, excessive
correction results from the emergence of a water diuresis after resolution of the cause of
hyponatremia
If plasma sodium has increased by > 10 mEq/L in 24 h or 18 mEq/L in 48 h, discontinue
ongoing active treatment
Consult an expert as to administer 5% dextrose in water in individual doses and
desmopressin to reduce urine volume until the plasma sodium is less than the limits of
overcorrection
Monitor plasma sodium every 2 h until it corrects, then every 4-6 h for the first 48 h
ODS = osmotic demyelination syndrome.
pontine and extrapontine myelinolysis—were less tem” that does not take into con-
frequent in patients whose electrolyte imbalance sideration urinary loss of electro-
was corrected more slowly (25). lytes or water, which substantially
It is extremely difficult to predict affects the actual change in plasma
the rate of correction of plasma sodium.
sodium levels. Initially, when pa- In a retrospective study of 62 hyponatremic pa-
tients are given hypertonic saline, tients treated with a low rate of hypertonic saline,
the formula that is often used to several patients were unintentionally overcor-
predict the initial increase in rected (11% by > 12 mEq/L in 24 h and 9.7% by
plasma takes into account the ad- >18 mEq/L in 48 h), despite frequent adjust-
25. Sterns RH, Cappuccio JD,
ministered amount of volume, so- ments in the infusion rate and/or administration Silver SM, et al. Neuro-
dium, and potassium and total of 5% dextrose in water. Using a predictive for- logic sequelae after treat-
ment of severe hypona-
body water (based on age and mula in patients with plasma sodium < 120 tremia:a multicenter
sex). It should be noted that this perspective. J Am Soc
mEq/L, the observed increase in plasma sodium Nephrolol. 1994;4:1522-
formula is based on a “closed sys- exceeded the formula's estimated increase in 30. [PMID: 8025225]
4 August 2015 Annals of Internal Medicine In the Clinic ITC11 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Table 5. Treatment of Patients with Asymptomatic Chronic Hyponatremia
Condition Treatment
Hypovolemia due to gastrointestinal Isotonic saline; consider concomitant desmopressin
losses and sweating*
Diuretics* Discontinue diuretics and if no improvement administer isotonic saline
Addison disease* Isotonic saline; glucocorticoid and mineralocorticoid replacement
Glucocorticoid insufficiency* Glucocorticoid replacement
Primary polydipsia* Restrict water; discontinue diuretics and any drug known to cause SIADH; if
volume-depleted or decreased solute excretion, cautiously administer isotonic
saline and consider desmopressin (if no access to fluids) initially or if there is a
rapid increase in urine output and/or plasma sodium
Decreased solute intake* Restrict water; discontinue diuretics and any drug known to cause SIADH; if
volume-depleted or decreased solute excretion, cautiously administer isotonic
saline and consider desmopressin (if no access to fluids) initially or if there is a
rapid increase in urine output and/or plasma sodium; increase electrolytes and
protein in their diet
Heart failure Restrict water and salt; loop diuretics in cases of fluid overload†
Cirrhosis with ascites Restrict water and salt; administer diuretics; possible albumin infusion with diuretics†
Nephrotic syndrome Restrict water and salt; diuretics; if clinically decreased effective circulating volume,
administer albumin with diuretics
Chronic kidney disease Restrict water and salt; loop diuretics if fluid overload is present
SIADH Discontinue diuretics and any drug known to cause SIADH; restrict water but not salt;
consider oral urea, salt tablets, furosemide with salt tablets, and demeclocycline if
water restriction is not effective; do not use vaptans unless benefit is greater than
risk and only for 1 month if following FDA guidelines
FDA = U.S. Food and Drug Administration; SIADH = syndrome of inappropriate antidiuretic hormone secretion.
* All patients are at risk for rapid correction.
† Loop diuretics should increase free water clearance.
74.2%. Inadvertent overcorrection was due to tion alone is usually unsuccessful
documented water diuresis in 40% of cases (26) if the sum of urinary sodium con-
How are patients with chronic centration plus potassium is
more than half the plasma so-
asymptomatic hyponatremia
dium concentration (27).
treated?
Table 5 presents guidance for What are manifestations of the
the treatment of patients with osmotic demyelination
chronic asymptomatic hyponatre- syndrome and who is at risk?
mia. Recommendations are When chronic hyponatremia is
based on expert consensus. It is corrected too rapidly, the inabil-
important not to administer iso- ity of the brain to rapidly recover
tonic saline to symptomatic or organic solutes lost in the adap-
asymptomatic clinically euv- tation to hyponatremia may lead
olemic patients with plasma so- to the osmotic demyelination
dium ≤ 120 mEq/L because lev- syndrome (ODS). The neurologic
els may decrease if urine is symptoms of this syndrome (dys-
hypertonic (i.e., the sum of uri- arthria, dysphagia, paraparesis or
nary concentrations of sodium quadriparesis, confusion, obtun-
plus potassium exceeds plasma dation, and coma) typically occur
26. Mohmand HK, Issa D,
Ahmad Z, et al. Hyper- sodium concentration) (3). The 2– 6 days after correction. Factors
tonic saline for hypona-
tremia: risk of inadver-
initial treatment of patients with that increase risk for ODS include
tent overcorrection. Clin euvolemic hypovolemia includes initial plasma sodium level < 105
J Am Soc Nephrol. 2007;
2:1110-7. [PMID: fluid restriction and stopping any mEq/L; hypokalemia; and a his-
17913972] medications that could cause
27. Furst H, Hallows KR, Post
tory of alcoholism, malnutrition,
J, et al. The urine/plasma SIADH. Salt should not be re- and advanced liver disease. ODS
electrolyte ratio: a predic-
tive guide to water re- stricted in patients with SIADH is more likely to occur if the in-
striction. Am J Med Sci. because they have decreased crease in plasma sodium exceeds
2000;319:240. [PMID:
10768609] total body sodium. Fluid restric- 10 mEq/L within 24 hours and 18
姝 2015 American College of Physicians ITC12 In the Clinic Annals of Internal Medicine 4 August 2015
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
mEq/L within 48 hours. Further- < 125 mEq/L, or risk factors for
more, plasma sodium may in- ODS should be hospitalized.
crease more than intended if the
How should clinicians counsel
cause of hyponatremia is revers-
ible. When the reason for hypo- patients about salt and fluid
natremia is removed (by volume intake and when to seek
resuscitation, discontinuation of a clinical care?
medication, cortisol replacement, Treatment of patients with hyper-
correction of hypoxia, or recov- volemic hyponatremia due to
ery from stress), AVP secretion is heart failure includes restriction of
suppressed, and excretion of di- dietary salt to 1.5 to 3.0 g/day and
lute urine (water diuresis) results fluid restriction. Some studies have
in a rapid increase in the plasma shown poorer clinical outcomes
sodium concentration. with lower salt intake. In general,
patients should be counseled to
Overcorrection of hyponatremia is limit fluid intake to 1.5–2 L/day un-
a medical emergency and should less hyponatremia worsens (30).
be avoided. If plasma sodium in- Patients with SIADH should be ad-
creases too rapidly, desmopressin vised to limit fluid intake to around
(synthetic AVP) can be given to
800 mL/day and not to restrict salt
prevent further urinary water
intake. Patients should seek care if
losses. Some authors have sug-
they experience altered mental
gested that desmopressin be given
status, falls, or persistent nausea
as soon as the targeted daily in-
because these may be symptoms
crease in plasma sodium levels (6–8
of hyponatremia.
mEq/L) has been achieved or water
diuresis begins. Others suggest giv- What other therapies,
ing desmopressin immediately to including medications, are
patients with reversible causes of used in the management of
hyponatremia, in anticipation of, hyponatremia?
rather than in response to, an unwel- The Appendix Table (available
come water diuresis. Plasma sodium at www.annals.org) presents an
is then increased with a slow infusion
overview of medications used to
of hypertonic saline, adjusted to
treat patients with asymptomatic
correct hyponatremia by 6 mEq/L
hyponatremia. When fluid re- 28. Sood L, Sterns RH, Hix
per day (28), while repeated doses JK, et al. Hypertonic
striction is unsuccessful, treat- saline and desmopres-
of desmopressin are given to pre-
ment options include use of salt sin: a simple strategy for
vent urinary water losses. In a recent safe correction of severe
tablets alone or with loop diuret- hyponatremia. Am J
review (29), the authors suggested Kidney Dis. 2013;61:
ics (particularly if the urine os-
starting desmopressin along with 571-8. [PMID:
molality is > 500 mOsm/kg). Al- 23266328]
isotonic saline in hypovolemic pa- 29. Tzamaloukas AH, Shapiro
though urea (usually 30 g/d) has JI, Raj DS, et al. Manage-
tients, psychiatric patients with hypo-
been shown to be as effective as ment of severe hypona-
natremia due to polydipsia (not cur- tremia: infusion of hyper-
tolvaptan (31), it is not readily tonic saline and
rently drinking), and patients with desmopressin or infusion
available in the United States
low solute intake who have a rapid of vasopressin inhibitors?
increase in urine output. The role of and not very palatable. Deme- Am J Med Sci 2014;0(0]:
1-8. [PMID: 25247759]
desmopressin in managing hypona- clocycline acts on the collecting 30. Yancy CW, Jessup M,
duct to decrease its response to Bozkurt B, et al. 2013
tremia requires further research (29). ACCF/AHA Guidelines for
AVP and has been used to treat the management of
When should patients be heart failure: executive
hyponatremia. The European summary. Circulation.
hospitalized for management guidelines (24) recommend 2013;128:1810-52.
[PMID: 23741057]
of hyponatremia? against demeclocycline because 31. Soupart A, Coffernils M,
Couturier B, et al. Efficacy
Hyponatremic patients who are of its delayed onset of action and tolerance of urea
symptomatic (e.g., confusion, and increased chance of acute compared with vaptans
for long-term treatment
headache, vomiting, and sei- kidney injury. The U.S. expert of patients with SIADH.
zures) and those with acute hypo- panel recommends demeclocy- Clin J Am Soc Nephrol.
2012;7:742-7. [PMID:
natremia, plasma sodium level cline as an alternative treatment 22403276]
4 August 2015 Annals of Internal Medicine In the Clinic ITC13 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
if fluid restriction is unsuc- The U.S. Food and Drug Admin-
cessful. Loop diuretics can be istration (FDA) has limited
useful in managing hyponatre- tolvaptan use to 1 month, based
mia in patients with heart failure on reports of hepatotoxicity as-
by increasing free water excre- sociated with high doses in pa-
tion. In severely symptomatic tients with autosomal dominant
hyponatremic patients with con- polycystic kidney disease. The
gestive heart failure (CHF) FDA also limits use to patients
and/or liver disease with ascites, with plasma sodium < 125
administration of loop diuretics mEq/L, unless they are symp-
with hypertonic saline can de- tomatic and have not re-
crease the chance of fluid over- sponded to fluid restriction.
load. The expert panel (23) acknowl-
edged the concern about vap-
When should clinicians
tans and hepatotoxicity. To
consider use of vasopressin-
avoid overcorrection, the panel
receptor antagonists? recommended that vaptans be
Vasopressin-receptor antago- used alone rather than in con-
nists (vaptans) block the effect junction with other treatments
of AVP, leading to increased for hyponatremia. The panel rec-
free water excretion. Conivap- ommended checking plasma so-
tan is an intravenous formula- dium levels every 6 – 8 hours dur-
tion and is approved for treat- ing initiation of vaptan treatment
ment of SIADH. Tolvaptan is an and not initially restricting fluid
oral formulation approved for intake. Although the panel stated
managing hyponatremia in CHF that these drugs could be used as
and SIADH. The 2014 European long-term therapy, it noted that
guidelines (24) recommend such use would probably be lim-
against vaptans for treatment of ited by high cost and FDA restric-
hyponatremia in patients with tions. Even with these significant
SIADH and expanded extracel- concerns, clinicians should con-
lular fluid. Although these sider treatment with vaptans in
guidelines acknowledge that patients who have not responded
vaptans increase plasma so- to other measures (i.e., plasma
dium in these patients, they also sodium < 125 mEq/L and/or per-
express concerns about the in- sistent symptoms believed to be
creased risk for rapid correction due to hyponatremia) if the antici-
of plasma sodium and lack of pated benefit exceeds the risk.
mortality benefit. There are re-
ports of neurologic sequelae in When should clinicians
patients who were treated with consult a nephrologist or
tolvaptan whose plasma sodium endocrinologist for treatment
correction exceeded the sug- of hyponatremia?
gested rate and possibly in- Clinicians should consult a neph-
creased the risk for death. rologist or endocrinologist for
During the past year, several guidance when administration of
national recommendations and hypertonic saline and/or vaptans is
guidelines (from the United considered. Consultations are also
Kingdom, Sweden, and Spain) indicated for acute, severe, or
have been published on man- symptomatic hyponatremia
agement of hyponatremia. Each (plasma sodium < 120 mEq/L) and
recommended use of tolvaptan for help in managing patients with
if fluid restriction was unsuc- risk factors for ODS, patients who
cessful in managing plasma have had overly rapid correction,
sodium levels in patients with or those who require long-term
hyponatremia. therapy for hyponatremia.
姝 2015 American College of Physicians ITC14 In the Clinic Annals of Internal Medicine 4 August 2015
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Treatment... Patients with severe hyponatremia, acute hyponatremia, or
moderate to severe symptoms should be hospitalized for diagnosis and
treatment. It is important to administer hypertonic saline to rapidly cor-
rect plasma sodium levels in patients with acute hyponatremia, even if
they are asymptomatic (e.g., exercise-associated hyponatremia), and
patients with moderate to severe symptoms (chronic or acute). It is also
important to monitor patients closely and not to increase levels > 10
mEq/L within 24 hours or 18 mEq/L within 48 hours. The recommended
rates of sodium correction are lower in patients at risk for ODS. Factors
that increase risk for this syndrome include an initial plasma sodium
level < 105 mEq/L, hypokalemia, alcoholism, malnutrition, and ad-
vanced liver disease. Clinicians considering tolvaptan should take into
account the FDA recommendation not to exceed 1 month of use.
CLINICAL BOTTOM LINE
Practice Improvement
What do professional management of all aspects of
organizations recommend heart failure, including sodium
regarding the diagnosis and and water restriction (30) (http:
treatment of hyponatremia? //circ.ahajournals.org/content
The 2013 US Expert Panel Rec- /128/16/1810.full?sid
ommendations (23) and 2014 =6716f9b4-016f-4ed6-8a58
European Clinical Practice -d74807c7eeb9).
Guidelines (24) are recent guide- Guidelines from the European
lines addressing the diagnosis Society of Cardiology address
and treatment of hyponatremia. the diagnosis and treatment of
heart failure (http://eurheartj.
IntheClinic
Guidelines from the American
College of Cardiology/American oxfordjournals.org/content/33
Heart Association address the /14/1787.long).
In the Clinic NIH MedLine Plus
www.nlm.nih.gov/medlineplus/ency/article/000394.htm
Tool Kit Clinical Guidelines
www.ese-hormones.org/guidelines/joint.aspx
www.eje-online.org/content/170/3/G1.full
Description and Information
www.mayoclinic.org/diseases-conditions
Hyponatremia /hyponatremia/basics/definition/CON-20031445?p=1
Patient Resources
www.mayoclinic.org/diseases-conditions
/hyponatremia/basics/definition/con-20031445
http://umm.edu/health/medical/ency/articles
/hyponatremia
Patient Resources in Spanish
http://nkdep.nih.gov/inicio.shtml
4 August 2015 Annals of Internal Medicine In the Clinic ITC15 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
WHAT YOU SHOULD In the Clinic
Annals of Internal Medicine
KNOW ABOUT
HYPONATREMIA
What Is Hyponatremia?
Hyponatremia is a condition that occurs when so-
dium levels in the body are too low. Sodium, or
salt, is a mineral in the blood. Sodium helps to
control the amount of water in your body. When
sodium levels are low, your body holds onto too
much water. Too much water in the body can be
dangerous and cause serious health problems.
Low sodium levels can be caused by:
• Certain medications, like water pills (diuretics)
or some antidepressants
• Some health conditions, like heart failure,
kidney disease, or liver problems
• Drinking too much water after intense
exercise, such as running a marathon
What Are the Warning Signs of
Questions for My Doctor
Hyponatremia? • Do I need to drink less water?
• Sometimes hyponatremia has no symptoms. • Should I eat more salt?
• Other times, symptoms include nausea, • Do I need to change my diet?
confusion, headache, or vomiting. • When can I expect my symptoms to go away?
• On rare occasions, symptoms are more • Could this cause any long-term problems?
severe. Severe symptoms can include • Should I change the medicines I take?
seizures, temporary loss of mental abilities, • How can I prevent this from happening in the
and trouble breathing. future?
• When should I contact my doctor?
How Is Hyponatremia Diagnosed?
• Your doctor will collect a blood and urine Bottom Line
Patient Information
sample to test sodium levels. • Hyponatremia is a condition that occurs when
• Imaging tests may be ordered to check for sodium levels in the body are too low. The
signs of hyponatremia. These tests may sodium in your blood helps to control the
include an x-ray to check for normal fluid amount of water in your body. When sodium is
levels in your lungs or an MRI of the brain to too low, there is too much water in your body.
look for things that might cause hyponatremia This can be dangerous and cause health
(for example, brain tumors). problems.
• Symptoms of hyponatremia can range from
How Is Hyponatremia Treated? headache or nausea to serious confusion and
• In mild cases, your doctor may simply advise seizures.
you to drink less fluid or change your • To check for hyponatremia, your doctor will
medications. collect a blood and urine sample. He or she
• Sometimes your doctor will give you a may also order further testing, like x-ray or an
medicine that helps reduce the amount of MRI.
water in your body. • Treatment will depend on how severe your
• In more severe cases, you may need to go to symptoms are. Treatment could include using
the hospital for diagnosis and treatment. An IV an IV to increase your sodium levels, taking a
filled with a salt-based fluid may be used to medicine to lessen the water in your body, or
increase your sodium levels. simply drinking less water.
For More Information
Medline Plus
www.nlm.nih.gov/medlineplus/ency/article/000394.htm
National Kidney Foundation
https://www.kidney.org/atoz/content/Hyponatremia
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Appendix Figure 1. Approach to the diagnosis of hypovolemic hyponatremia.
High Probability of
Hypovolemia
Based on clinical history
and physical examination
Variable UNa <30 UNa >30
UNa mEq/L mEq/L†
Diuretics Extrarenal losses Renal
Vomiting* losses
Diarrhea
D/C Pancreatitis
diuretics Sweating
Osmotic diuresis Sait-Iosing
Small bowel ACTH-
(glucose, urea nephritis
obstruction stimulation
bicarbonaturia) Addison
Failure to test
disease
normalize
CSW
PNa Consistent with
Addison disease
Administer Treatment:
0.9% saline Glucocorticoids and
mineralocorticoids
Failure to Normalize PNa
normalize PNa
Hypovolemia
Decreasing Uosm No change in Uosm
UNa increases
Hypovolemia Salt-depleted
SIADH
ACTH = adrenocorticotrophic hormone; CSW = cerebral salt wasting; D/C = discontinue; SIADH = syndrome of inappropriate antidiuretic
hormone secretion.
* If patient is vomiting, UCl should be low.
† Volume-depleted elderly patients can have urinary sodium > 30 mEq/L but FENa <0.5%.
4 August 2015 Annals of Internal Medicine In the Clinic 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Appendix Figure 2. Approach to the diagnosis of euvolemic hyponatremia.
Clinical Euvolemia
UNa <20 Variable UNa >20 UNa <40 UNa >40
mEq/L mEq/L mEq/L
Probable Hypovolemia Probable
D/C diuretics
hypovolemia or euvolemia euvolemia
SIADH
PNa Failure of PNa Cortisol
normalizes to normalize deficiency
Hypothyroidism*
Not SIADH Unclear diagnosis after
ruling out cortisol deficiency,
hypothyroidism
Administer 1–2 L
0.9% saline†
PNa decreases or PNa increases
no change
SIADH Decreased UNa No change in Uosm
UNa increases
Administer
additional SIADH
saline
Decreasing Uosm No change in Uosm
UNa increases
Hypovolemia Salt-depleted
SIADH
D/C = discontinue; SIADH = syndrome of inappropriate antidiuretic hormone secretion.
* Severe hypothyroidism = urinary sodium < 20 mEq/L.
† If plasma sodium < 120 mEq/L, consult endocrinologist or nephrologist for guidance.
Appendix Figure 3. Approach to
the diagnosis of hypervolemic
hyponatremia.
Hypervolemia
UNa <30 UNa >30
mEq/L* mEq/L
Heart failure Chronic kidney
Liver disease disease†
Nephrotic Diuretic use in:
syndrome Heart failure
Liver disease
Nephrotic
syndrome
* If patient is receiving diuretics, urinary so-
dium can be >30 mEq/L.
† Patients with chronic kidney disease can
also be euvolemic.
姝 2015 American College of Physicians In the Clinic Annals of Internal Medicine 4 August 2015
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
Appendix Table. Drug and Nondrug Treatment for Hyponatremia
Drug or Drug Class Dosing Side Effects Precautions Clinical Use
Sodium chloride 5–15 g daily Hypernatremia, fluid overload SIADH common when
tablets combined with
furosemide
Furosemide (Lasix) 20–80 mg daily Orthostatic hypotension, Water and electrolyte Combined with sodium
hyperuricemia, azotemia, depletion; caution supplementation in
ototoxicity, impaired with sulfonamide SIADH, CHF, and
glucose tolerance, hypersensitivity, liver disease with
pancreatitis CKD, hepatic ascites
impairment*
Urea 15–30 g daily Too rapid an increase in Monitor serum SIADH
serum sodium, poor sodium levels
palatability, azotemia at
higher doses
Demeclocycline 600–1200 mg total CNS side effects, nausea, Avoid with SIADH
(Declomycin) daily dose, vomiting, diarrhea, pregnancy; caution
dosed 3 to 4 photosensitivity, azotemia, with hepatic
times daily acute renal failure, disease, CKD; do
hematologic effects with not administer
long-term therapy within 4 hours of
drugs containing
divalent or trivalent
cations; administer
1 h before or 2 h
after meals
Tolvaptan (Samsca) 15 mg daily, then Xerostomia, asthenia, Initiate and reinitiate Can be useful in SIADH
30 mg daily; hyperglycemia, anorexia, in a hospital and and CHF if benefit
maximum 60 hepatic disease, monitor serum exceeds risk
mg daily constipation, thirst, sodium levels;
pollakiuria, polyuria, avoid if CrCl*
dehydration, orthostatic
hypotension, neurologic
sequelae when correction
of serum sodium exceeds
the suggested rate
CHF = congestive heart failure; CKD = chronic kidney disease; CNS = central nervous system; CrCl = creatinine clearance; CYP =
cytochrome P450 isoenzyme; P-gp = P-glycoprotein; SCr = serum creatinine; SIADH = syndrome of inappropriate antidiuretic
hormone secretion.
* Black box warning.
4 August 2015 Annals of Internal Medicine In the Clinic 姝 2015 American College of Physicians
Downloaded From: http://annals.org/ by a University of York User on 11/18/2016
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)Document61 pages2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)AdelaNo ratings yet
- Sepsis and ShockDocument13 pagesSepsis and ShockUther Pendragon100% (2)
- Sun 2012Document6 pagesSun 2012ntnquynhproNo ratings yet
- Ni Hms 316844Document15 pagesNi Hms 316844ntnquynhproNo ratings yet
- NIH Public Access: Author ManuscriptDocument23 pagesNIH Public Access: Author ManuscriptntnquynhproNo ratings yet
- Dapus PDFDocument49 pagesDapus PDFsyahyuniNo ratings yet
- SAE Delirium PDFDocument14 pagesSAE Delirium PDFandi widizNo ratings yet
- 2020 Respiratory Drive in The Acute Respiratory Distress SyndromeDocument13 pages2020 Respiratory Drive in The Acute Respiratory Distress SyndromegiseladlrNo ratings yet
- Defining Immune Reconstitution Inflammatory SyndromeDocument9 pagesDefining Immune Reconstitution Inflammatory SyndromentnquynhproNo ratings yet
- Pulmonary IRIS ERS PDFDocument8 pagesPulmonary IRIS ERS PDFAswith JonnalagaddaNo ratings yet
- CNS-Immune Reconstitution Inflammatory Syndrome in The Setting of HIV Infection, Part 1Document11 pagesCNS-Immune Reconstitution Inflammatory Syndrome in The Setting of HIV Infection, Part 1ntnquynhproNo ratings yet
- Immune Reconstitution Inflammatory SyndromeDocument2 pagesImmune Reconstitution Inflammatory SyndromentnquynhproNo ratings yet
- The Three C's of Antibiotic Allergy - Classification, Cross - Reactivity and CollaborationDocument22 pagesThe Three C's of Antibiotic Allergy - Classification, Cross - Reactivity and CollaborationntnquynhproNo ratings yet
- Approach To Pancytopenia: Moderator - DR Vishal Gupta MD Medicine Presented By-Dr Narendra Singh Resident Doctor 2Document35 pagesApproach To Pancytopenia: Moderator - DR Vishal Gupta MD Medicine Presented By-Dr Narendra Singh Resident Doctor 2ntnquynhproNo ratings yet
- Defining Immune Reconstitution Inflammatory Syndrome: Evaluation of Expert Opinion Versus 2 Case Definitions in A South African CohortDocument9 pagesDefining Immune Reconstitution Inflammatory Syndrome: Evaluation of Expert Opinion Versus 2 Case Definitions in A South African CohortntnquynhproNo ratings yet
- CNS-Immune Reconstitution Inflammatory Syndrome in The Setting of HIV Infection, Part 2Document11 pagesCNS-Immune Reconstitution Inflammatory Syndrome in The Setting of HIV Infection, Part 2ntnquynhproNo ratings yet
- Immune Reconstitution Inflammatory Syndrome in HIV Infected Late Presenters Starting Integrase Inhibitor Containing Antiretroviral TherapyDocument10 pagesImmune Reconstitution Inflammatory Syndrome in HIV Infected Late Presenters Starting Integrase Inhibitor Containing Antiretroviral TherapyntnquynhproNo ratings yet
- HIV and Immune Reconstitution Inflammatory Syndrome HIV IRISDocument8 pagesHIV and Immune Reconstitution Inflammatory Syndrome HIV IRISntnquynhproNo ratings yet
- Cryptococcal Lung DiseaseDocument7 pagesCryptococcal Lung DiseasentnquynhproNo ratings yet
- Central Nervous System Immune Reconstitution Inflammatory SyndromeDocument19 pagesCentral Nervous System Immune Reconstitution Inflammatory SyndromentnquynhproNo ratings yet
- Current Diagnosis and Treatment of Cryptococcal Meningitis Without Acquired Immunodeficiency SyndromeDocument8 pagesCurrent Diagnosis and Treatment of Cryptococcal Meningitis Without Acquired Immunodeficiency SyndromentnquynhproNo ratings yet
- Comparative Effectiveness of Induction Therapy For Human Immunodeficiency Virus-Associated Cryptococcal Meningitis: A Network Meta-AnalysisDocument12 pagesComparative Effectiveness of Induction Therapy For Human Immunodeficiency Virus-Associated Cryptococcal Meningitis: A Network Meta-AnalysisntnquynhproNo ratings yet
- Combination Versus Monotherapy For The Treatment of HIV Associated Cryptococcal Meningitis PDFDocument3 pagesCombination Versus Monotherapy For The Treatment of HIV Associated Cryptococcal Meningitis PDFntnquynhproNo ratings yet
- Shedding Light On IRIS: From Pathophysiology To Treatment of Cryptococcal Meningitis and Immune Reconstitution Inflammatory Syndrome in HIV-Infected Individuals PDFDocument10 pagesShedding Light On IRIS: From Pathophysiology To Treatment of Cryptococcal Meningitis and Immune Reconstitution Inflammatory Syndrome in HIV-Infected Individuals PDFntnquynhproNo ratings yet
- A Phase II Randomized Trial of Amphotericin B Alone or Combined With Fluconazole Cryptococcal Meningitis:AIDS Info PDFDocument9 pagesA Phase II Randomized Trial of Amphotericin B Alone or Combined With Fluconazole Cryptococcal Meningitis:AIDS Info PDFntnquynhproNo ratings yet
- An Update On Cryptococcosis Among HIV-Infected Persons PDFDocument13 pagesAn Update On Cryptococcosis Among HIV-Infected Persons PDFntnquynhproNo ratings yet
- Majorarticle: Hiv/AidsDocument8 pagesMajorarticle: Hiv/AidsntnquynhproNo ratings yet
- Revista Iberoamericana de Micologı A: Rafael Laniado-Laborı N and Maria Noemı Cabrales-VargasDocument5 pagesRevista Iberoamericana de Micologı A: Rafael Laniado-Laborı N and Maria Noemı Cabrales-VargasYashveerDabasNo ratings yet
- Symptomatic Relapse of HIV-associated Cryptococcal Meningitis in South Africa: The Role of Inadequate Secondary Prophylaxis PDFDocument10 pagesSymptomatic Relapse of HIV-associated Cryptococcal Meningitis in South Africa: The Role of Inadequate Secondary Prophylaxis PDFntnquynhproNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Surgical Diseases of PancreasDocument17 pagesSurgical Diseases of PancreasIris BakerNo ratings yet
- Exchange of Gases in AnimalsDocument23 pagesExchange of Gases in AnimalsHenry JacobNo ratings yet
- Features of The Muscular SystemDocument34 pagesFeatures of The Muscular SystemQuỳnh NhưNo ratings yet
- Top 100 Pathology Secrets List W/ NotesDocument6 pagesTop 100 Pathology Secrets List W/ NotesPA2014100% (4)
- Understanding Inflammatory Bowel DiseaseDocument4 pagesUnderstanding Inflammatory Bowel DiseaseKathleen B BaldadoNo ratings yet
- Validity and Reliability of The St. Georges Respiratory Questionnaire in Assessing Health Status in Patients With Chronic Pulmonary Aspergillosis.Document9 pagesValidity and Reliability of The St. Georges Respiratory Questionnaire in Assessing Health Status in Patients With Chronic Pulmonary Aspergillosis.Annas Diah L.No ratings yet
- Diagnostic Approach To and Treatment of Thyroid Nodules - UpToDate PDFDocument36 pagesDiagnostic Approach To and Treatment of Thyroid Nodules - UpToDate PDFDANIEL SANTAMARIANo ratings yet
- RPG Series Ophthalmology Buster PDFDocument299 pagesRPG Series Ophthalmology Buster PDFDanielle SangalangNo ratings yet
- Daftar Pustaka Covid-19 LiteratureDocument4 pagesDaftar Pustaka Covid-19 LiteratureReynida HutagalungNo ratings yet
- PCR ReportDocument2 pagesPCR Reportpriyanka senNo ratings yet
- What Is A Palliative ApproachDocument4 pagesWhat Is A Palliative ApproachJayanti Ika siwiNo ratings yet
- Lesson Plan Personality Disorders A Class of Their Own - 0Document9 pagesLesson Plan Personality Disorders A Class of Their Own - 0Sanjay SinghNo ratings yet
- MINDMAPDocument2 pagesMINDMAPrayzaoliveira.ausNo ratings yet
- Writing 3 and Model AnswersDocument4 pagesWriting 3 and Model AnswersAsadullah khanNo ratings yet
- Health-Related Quality of Life ScaleDocument4 pagesHealth-Related Quality of Life ScaleMihaela Cosmina NiculescuNo ratings yet
- Human Capital: Education and Health in Economic DevelopmentDocument16 pagesHuman Capital: Education and Health in Economic DevelopmentRoselle Jane LanabanNo ratings yet
- Occupational Diseases 302-04280 enDocument19 pagesOccupational Diseases 302-04280 enJithesh S VNo ratings yet
- Vincristine - Canton Bsn3bDocument3 pagesVincristine - Canton Bsn3bMavy CantonNo ratings yet
- FAQs on TB Causes, Symptoms, Tests & TreatmentDocument4 pagesFAQs on TB Causes, Symptoms, Tests & TreatmentMystery ShopperNo ratings yet
- COVID-19 Healthcare Settings SummaryDocument27 pagesCOVID-19 Healthcare Settings SummaryBeugh RiveraNo ratings yet
- Test Bank For Varcarolis Foundations of Psychiatric Mental Health Nursing 8th Edition by HalterDocument10 pagesTest Bank For Varcarolis Foundations of Psychiatric Mental Health Nursing 8th Edition by HalterJohn Ngo100% (26)
- Gallstones: Causes, Complications and Treatment OptionsDocument6 pagesGallstones: Causes, Complications and Treatment Optionsricky aditNo ratings yet
- Draft List of MicroorganismsDocument36 pagesDraft List of MicroorganismsAngadNo ratings yet
- Common Inflammatory and Infectious Conditions of The EyelidDocument7 pagesCommon Inflammatory and Infectious Conditions of The EyelidinayahNo ratings yet
- Course Plan For MSN-IIDocument16 pagesCourse Plan For MSN-IIRuchika KaushalNo ratings yet
- Ayurvedic Recipes for Common Ailments Using Indian Gooseberry, Betel Leaves and MoreDocument91 pagesAyurvedic Recipes for Common Ailments Using Indian Gooseberry, Betel Leaves and MoreKanjarla Hanmonthrao Panthulu Laxmana0% (1)
- Pharmacology SummaryDocument31 pagesPharmacology Summarydesshe09No ratings yet
- 2 Drug-StudyDocument2 pages2 Drug-StudyNoreen GyleNo ratings yet
- 17 The Brigham Board Review in Critical Care Medicine 2017Document1,355 pages17 The Brigham Board Review in Critical Care Medicine 2017Thanh NguyenNo ratings yet
- OCD ChecklistDocument3 pagesOCD ChecklistfarrukhakhtarNo ratings yet