You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- ITE Crash Course - CardiologyDocument260 pagesITE Crash Course - CardiologyDre2323No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Aortic Dissection PP PresentationDocument64 pagesAortic Dissection PP PresentationKonstantin DimitrovNo ratings yet
- Aortoiliac DiseaseDocument110 pagesAortoiliac DiseaseAmr AbdelghaffarNo ratings yet
- Extracranial Carotid Artery Aneurysm - UpToDateDocument25 pagesExtracranial Carotid Artery Aneurysm - UpToDateDiego RodriguesNo ratings yet
- Amls Pretest BlsDocument13 pagesAmls Pretest BlsrkopecmdNo ratings yet
- Chest Pain and DiscomfortDocument2 pagesChest Pain and DiscomfortGerryNickNo ratings yet
- Evaluation and Treatment of Hypertensive Emergencies in Adults - UpToDateDocument13 pagesEvaluation and Treatment of Hypertensive Emergencies in Adults - UpToDaterolland_arrizaNo ratings yet
- Test Taking StrategyDocument15 pagesTest Taking StrategyAumrishNo ratings yet
- Chest X-RayDocument39 pagesChest X-Rayendah cahya sufianyNo ratings yet
- Use of "Bioglue" in Aortic Surgical RepairDocument3 pagesUse of "Bioglue" in Aortic Surgical RepairLeonardoCampanelliNo ratings yet
- Abdominal Aortic AneurysmDocument10 pagesAbdominal Aortic AneurysmSNo ratings yet
- Erythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesDocument27 pagesErythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesMisbah KaleemNo ratings yet
- Stroke Mimics: Incidence, Aetiology, Clinical Features and TreatmentDocument18 pagesStroke Mimics: Incidence, Aetiology, Clinical Features and TreatmentCristianNo ratings yet
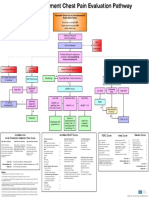
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Philippines Relative Value Unit:Surgeries 2007Document6 pagesPhilippines Relative Value Unit:Surgeries 2007Katherine 'Chingboo' Leonico Laud50% (2)
- DsaDocument235 pagesDsaLalaine De Jesus100% (1)
- Chest Pain in Pediatrics: Tisha K. Yeh, MD and Jay Yeh, MDDocument5 pagesChest Pain in Pediatrics: Tisha K. Yeh, MD and Jay Yeh, MDMahmoud AbouelsoudNo ratings yet
- Radiology Ordering GuideDocument27 pagesRadiology Ordering GuideRahim Rajab AliNo ratings yet
- Unit Exam #1: Blood Vessels: B.) Advanced Glycation End ProductsDocument85 pagesUnit Exam #1: Blood Vessels: B.) Advanced Glycation End ProductsCherry RahimaNo ratings yet
- IVMS-Gross Pathology, Histopathology, Microbiology and Radiography High Yield Image PlatesDocument151 pagesIVMS-Gross Pathology, Histopathology, Microbiology and Radiography High Yield Image PlatesMarc Imhotep Cray, M.D.100% (2)
- Cardiologia Croatica 2021 16 - 1-2 - 83Document1 pageCardiologia Croatica 2021 16 - 1-2 - 83daia4322746No ratings yet
- Journal (10 24 22)Document3 pagesJournal (10 24 22)Louigen DagaydayNo ratings yet
- Acute Limb IschemicDocument14 pagesAcute Limb IschemicLuke FloydNo ratings yet
- Turner Syndrome: A Guide For FamiliesDocument30 pagesTurner Syndrome: A Guide For FamiliesTatiana Pogo RamosNo ratings yet
- Internal Medicine Essentials For Clerkship Students 2Document369 pagesInternal Medicine Essentials For Clerkship Students 2asdf234234888100% (5)
- Vascular EmergenciesDocument43 pagesVascular EmergenciesMohammad BanisalmanNo ratings yet
- Full Download pdf of Vascular Medicine: A Companion to Braunwald’s Heart Disease 3rd Edition Mark Creager - eBook PDF all chapterDocument69 pagesFull Download pdf of Vascular Medicine: A Companion to Braunwald’s Heart Disease 3rd Edition Mark Creager - eBook PDF all chapterlugeydieen100% (4)
- ABSTRACT TEVAR - Achmad Ismail S Putra NewDocument3 pagesABSTRACT TEVAR - Achmad Ismail S Putra NewPutra AchmadNo ratings yet
- Diseccion Aortica Acguda CronicaDocument10 pagesDiseccion Aortica Acguda Cronicaarturo garciaNo ratings yet
- Old Free 120 - Answers & Explanations (BW)Document17 pagesOld Free 120 - Answers & Explanations (BW)frabziNo ratings yet