You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- التفكير بسرعة والتفكير ببطئ PDFDocument8 pagesالتفكير بسرعة والتفكير ببطئ PDFعبدالعزيز عابدNo ratings yet
- Datex-Ohmeda S/5™ Extension Frame, F-EXT4 (Rev. 03) S/5™ Extension Module, M-EXT (Rev. 02) Technical Reference ManualDocument26 pagesDatex-Ohmeda S/5™ Extension Frame, F-EXT4 (Rev. 03) S/5™ Extension Module, M-EXT (Rev. 02) Technical Reference Manualluis hernando bastidas duarteNo ratings yet
- مفهوم العبادة في الاسلامDocument33 pagesمفهوم العبادة في الاسلامعبدالعزيز عابدNo ratings yet
- المختصر في الحقوق الزوجية PDFDocument46 pagesالمختصر في الحقوق الزوجية PDFعبدالعزيز عابدNo ratings yet
- دليل المدرب في تدريب المدربين PDFDocument89 pagesدليل المدرب في تدريب المدربين PDFعبدالعزيز عابدNo ratings yet
- المختصر في الحقوق الزوجيةDocument46 pagesالمختصر في الحقوق الزوجيةعبدالعزيز عابدNo ratings yet
- الحوار مع الآخرDocument53 pagesالحوار مع الآخرعبدالعزيز عابدNo ratings yet
- التفكير بسرعة والتفكير ببطئ PDFDocument8 pagesالتفكير بسرعة والتفكير ببطئ PDFعبدالعزيز عابدNo ratings yet
- SAS-2 Operator Manual Setup and Operation GuideDocument23 pagesSAS-2 Operator Manual Setup and Operation Guideعبدالعزيز عابدNo ratings yet
- التفكير الإبداعي PDFDocument60 pagesالتفكير الإبداعي PDFعبدالعزيز عابدNo ratings yet
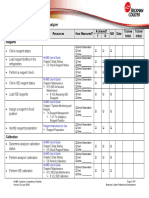
- AU480 Chemistry Analyzer: Competency ChecklistDocument4 pagesAU480 Chemistry Analyzer: Competency ChecklistTrần Văn BìnhNo ratings yet
- Operation Manual: IM17 Mitsar Co - LTDDocument70 pagesOperation Manual: IM17 Mitsar Co - LTDعبدالعزيز عابدNo ratings yet
- مستند جديد 2019-11-17 22.03.55 - 1-1Document1 pageمستند جديد 2019-11-17 22.03.55 - 1-1عبدالعزيز عابدNo ratings yet
- الحوار مع الآخرDocument53 pagesالحوار مع الآخرعبدالعزيز عابدNo ratings yet
- DOE Tutorial Explains Design OptimizationDocument16 pagesDOE Tutorial Explains Design OptimizationvilukNo ratings yet
- Transducer (Chp6)Document13 pagesTransducer (Chp6)medisaNo ratings yet
- How Glucose and Insulin Regulate Each Other in the BodyDocument9 pagesHow Glucose and Insulin Regulate Each Other in the Bodyعبدالعزيز عابدNo ratings yet
- SIEMENS ARTIS ZEE DMP-R Cath Lab - 2010-NDocument5 pagesSIEMENS ARTIS ZEE DMP-R Cath Lab - 2010-Nعبدالعزيز عابدNo ratings yet
- Principles of Programming: Flow Charts, Illustrations Through ExamplesDocument9 pagesPrinciples of Programming: Flow Charts, Illustrations Through Examplesعبدالعزيز عابدNo ratings yet
- Ultrasound Repair and TroubleshootingDocument4 pagesUltrasound Repair and TroubleshootingOliver GonzalezNo ratings yet
- Chapter 1 - Medical PHYSICS - 2019Document20 pagesChapter 1 - Medical PHYSICS - 2019عبدالعزيز محمد عابد العابدNo ratings yet
- Host Manual COBAS - INTEGRA - 400 - Plus PDFDocument144 pagesHost Manual COBAS - INTEGRA - 400 - Plus PDFnestordaniel7633% (3)
- Dallas RTCDocument18 pagesDallas RTCdr-SlumpNo ratings yet
- Ultrasound Preventative MaintenanceDocument1 pageUltrasound Preventative Maintenanceعبدالعزيز عابدNo ratings yet
- HQ-350XT Film Processor Service Manual: - Only For Service Person's ReferenceDocument40 pagesHQ-350XT Film Processor Service Manual: - Only For Service Person's Referenceعبدالعزيز عابدNo ratings yet
- The StudyDocument1 pageThe Studyعبدالعزيز عابدNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Silicon Containing Coralline Hydroxyapatite Bone GraftDocument1 pageSilicon Containing Coralline Hydroxyapatite Bone GraftfaluviekadianiNo ratings yet
- Limb Lengthening Surgery by Ilizarov Methodology PDFDocument3 pagesLimb Lengthening Surgery by Ilizarov Methodology PDFJessica Saing100% (1)
- Splints & Tractions in Orthopaedics: - DR - Akif A.BDocument67 pagesSplints & Tractions in Orthopaedics: - DR - Akif A.BChandrima MukherjeeNo ratings yet
- Operative Techniques in Foot and Ankle Surgery 2nd Edition Ebook PDFDocument61 pagesOperative Techniques in Foot and Ankle Surgery 2nd Edition Ebook PDFmaurice.honeycutt512100% (45)
- Article 13Document8 pagesArticle 13Waqas HaleemNo ratings yet
- DOC1656 Instruments Cardiac Vascular Surgery BrochureDocument94 pagesDOC1656 Instruments Cardiac Vascular Surgery BrochurePranabh KushwahaNo ratings yet
- Cep Halo MetricDocument6 pagesCep Halo MetricDaniel GamarraNo ratings yet
- A A L A M D B, N (1902-1956) : N Ccount of The Ife and Chievements of ISS Iana ECK EurosurgeonDocument5 pagesA A L A M D B, N (1902-1956) : N Ccount of The Ife and Chievements of ISS Iana ECK EurosurgeonAndreea IduNo ratings yet
- The Unstable ElbowDocument17 pagesThe Unstable ElbowwerwrNo ratings yet
- New Active Tie-Back Method for Space ClosureDocument1 pageNew Active Tie-Back Method for Space Closuredruzair007No ratings yet
- Evolution of The Septoplasty Maximizing Functional and Aesthetic Outcomes in Nasal SurgeryDocument9 pagesEvolution of The Septoplasty Maximizing Functional and Aesthetic Outcomes in Nasal SurgeryLeslie Lindsay AlvarezNo ratings yet
- Conserving Blood During Cardiac Surgery at Huntington University Hospital (A)Document6 pagesConserving Blood During Cardiac Surgery at Huntington University Hospital (A)Touba KhalidNo ratings yet
- Discuss Tension Band Principles: by DR Kabiru SALISU 11 Aug. 2017Document40 pagesDiscuss Tension Band Principles: by DR Kabiru SALISU 11 Aug. 2017Azmi FarhadiNo ratings yet
- A Collective Call - 12 October 2021 - 1050pmDocument22 pagesA Collective Call - 12 October 2021 - 1050pmBlogWatchNo ratings yet
- Prelim ExamDocument17 pagesPrelim Examsaci PTNo ratings yet
- Open Heart Surgery JournalDocument3 pagesOpen Heart Surgery Journalapi-546517574No ratings yet
- TURP (Transurethral Resection of The Prostate)Document5 pagesTURP (Transurethral Resection of The Prostate)shyam varmaNo ratings yet
- Johnson City Trauma ReportDocument9 pagesJohnson City Trauma ReportSlater TeagueNo ratings yet
- Spondilolistesis Klasifikasi MeyerdingDocument6 pagesSpondilolistesis Klasifikasi MeyerdingAriandindi AriandiNo ratings yet
- Operating Room ManagementDocument4 pagesOperating Room ManagementJeremy Lyle JabonilloNo ratings yet
- ERAS & TTSH Experience - Indonesia 2019 JakartaDocument79 pagesERAS & TTSH Experience - Indonesia 2019 JakartaFransisca Dewi KumalaNo ratings yet
- BeerDocument5 pagesBeerchristian makaryNo ratings yet
- Resorbable Material For Pediatric Orbital Floor ReconstructionDocument4 pagesResorbable Material For Pediatric Orbital Floor Reconstructionstoia_sebiNo ratings yet
- Lefort One - Google SearchDocument1 pageLefort One - Google SearchaeshaNo ratings yet
- AL-NUKHBAH Drug Store Company Profile Sept2018Document14 pagesAL-NUKHBAH Drug Store Company Profile Sept2018Hani AbushiekhaNo ratings yet
- Polio - Ankle and FootDocument9 pagesPolio - Ankle and FootDoc DelowerNo ratings yet
- DR Bharat Dave - SpinesurgeryfellowshipDocument2 pagesDR Bharat Dave - SpinesurgeryfellowshipPriyank GuptaNo ratings yet
- 10 Implant Imaging 1 by 1Document8 pages10 Implant Imaging 1 by 1bhupendraNo ratings yet
- Brain Surgery Ashley SwaffordDocument13 pagesBrain Surgery Ashley Swaffordapi-351075108No ratings yet
- Sarver Mission PossibleDocument13 pagesSarver Mission PossibleAndrea Cárdenas Sandoval100% (1)