You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Low Testosterone: Testosterone Testicles Sex DriveDocument4 pagesLow Testosterone: Testosterone Testicles Sex DriveQ NOnk ChubyNo ratings yet
- CH 040 Evaluation and Management of Status Epilepticus in ChildrenDocument7 pagesCH 040 Evaluation and Management of Status Epilepticus in Childrensuheena.CNo ratings yet
- NCM104 Midterm ReviewerDocument17 pagesNCM104 Midterm ReviewerShort Rider PhNo ratings yet
- RANDOX Glucose (GLUC-PAP)Document1 pageRANDOX Glucose (GLUC-PAP)Yeliztli Marin CelsoNo ratings yet
- - أسئلة التغذيةDocument52 pages- أسئلة التغذيةMicheal Mikhail YoussefNo ratings yet
- Criterios de Clsificacion de Espondilitis AnquilosanteDocument16 pagesCriterios de Clsificacion de Espondilitis AnquilosanteWilkerson PerezNo ratings yet
- Upper Motor Neuron Vs Lower Motor Neuron AtfDocument4 pagesUpper Motor Neuron Vs Lower Motor Neuron AtfRishi VermaNo ratings yet
- Diagnosis and Treatment Plan in FPD - PPTX NewDocument99 pagesDiagnosis and Treatment Plan in FPD - PPTX Newreshma shaikNo ratings yet
- Sut Ams Medical College, TVMDocument7 pagesSut Ams Medical College, TVMDIVYA R.S100% (1)
- WB CC Critical Care Front MatterDocument18 pagesWB CC Critical Care Front MatterkushishaNo ratings yet
- Aschelminthes: by The Students of Class Xi, Roll Number:-01-05Document11 pagesAschelminthes: by The Students of Class Xi, Roll Number:-01-05Ryan WalkerNo ratings yet
- Obsessive-Compulsive Disorder in Sports-Beyond SuperstitionsDocument13 pagesObsessive-Compulsive Disorder in Sports-Beyond Superstitionsnicole dufournel salasNo ratings yet
- Protocol For Randomized Controlled Trial of ElectrDocument7 pagesProtocol For Randomized Controlled Trial of ElectrFatima Habbaba JibrinNo ratings yet
- Micro by DR - Hesham (GIT)Document65 pagesMicro by DR - Hesham (GIT)abcde990075No ratings yet
- II. PATHOPHYSIOLOGY (Schematic Diagram) : Risk Factors Predisposing FactorsDocument3 pagesII. PATHOPHYSIOLOGY (Schematic Diagram) : Risk Factors Predisposing FactorsYongNo ratings yet
- Blood Pressure Lab Report/ WorksheetDocument4 pagesBlood Pressure Lab Report/ WorksheetKate CamachoNo ratings yet
- Occupational Management of Workers With Diabetes MellitusDocument11 pagesOccupational Management of Workers With Diabetes Mellitusari gunawanNo ratings yet
- Activity Sheet HealthDocument2 pagesActivity Sheet HealthTummys TummieNo ratings yet
- Y8 Biology Worksheet Task 1,2 and 3 SerenaDocument3 pagesY8 Biology Worksheet Task 1,2 and 3 SerenaSERENA TAYNo ratings yet
- Pseudomembranous Colitis: Not Always Clostridium Difficile: Cleveland Clinic Journal of Medicine May 2016Document7 pagesPseudomembranous Colitis: Not Always Clostridium Difficile: Cleveland Clinic Journal of Medicine May 2016Fitria FieraNo ratings yet
- Cambridge English For Nursing Authentic Medical Forms and ChartsDocument11 pagesCambridge English For Nursing Authentic Medical Forms and ChartsAngela MercadoNo ratings yet
- Lesson Plan On Electroconvulsive TherapyDocument13 pagesLesson Plan On Electroconvulsive Therapysimranjeet kaurNo ratings yet
- PDF Neurologic Interventions For Physical Therapy Third Edition Kessler Ebook Full ChapterDocument53 pagesPDF Neurologic Interventions For Physical Therapy Third Edition Kessler Ebook Full Chapterannie.frey695100% (1)
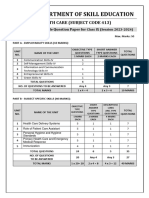
- 413 Health Care SQPDocument7 pages413 Health Care SQPAnil SarohaNo ratings yet
- Social Self ReportDocument74 pagesSocial Self ReportEsther Joy Hugo100% (1)
- Pe 10 Strategies 2ND GRADINGDocument8 pagesPe 10 Strategies 2ND GRADINGMarissa C AustriaNo ratings yet
- Cavitron Denstply PDFDocument145 pagesCavitron Denstply PDFMary Yohanna Cruz GuerreroNo ratings yet
- Valvular DisordersDocument1 pageValvular DisordersKevin VillaranteNo ratings yet
- LR ProtocolDocument159 pagesLR ProtocolJeevan VelanNo ratings yet
- Motivations For Participation in Physical Activity Across The LifespanDocument16 pagesMotivations For Participation in Physical Activity Across The LifespanPaopao MacalaladNo ratings yet