You might also like
- Spinal Cord: Anatomy and NeuroimagingDocument52 pagesSpinal Cord: Anatomy and NeuroimagingslojnotakNo ratings yet
- Spinal Nerve Plexuses and Dermatomes/MyotomesDocument25 pagesSpinal Nerve Plexuses and Dermatomes/Myotomesdsdfsa100% (1)
- Radial Nerve: Rajadurai R Crri, Orthopedics Ii Unit RGGGHDocument31 pagesRadial Nerve: Rajadurai R Crri, Orthopedics Ii Unit RGGGHrajaeasNo ratings yet
- Week 6 - PCPDocument6 pagesWeek 6 - PCPapi-479754549No ratings yet
- แกะเทป Developmental of Musculoskeletal SystemDocument50 pagesแกะเทป Developmental of Musculoskeletal Systemjulesarojinee100% (1)
- Dermatomes and Myotomes and Its Clinical Special Test in Upper Limb and Lower LimbDocument42 pagesDermatomes and Myotomes and Its Clinical Special Test in Upper Limb and Lower LimbkkaammiillaahhNo ratings yet
- Intramedullary Spinal Cord TumorsDocument7 pagesIntramedullary Spinal Cord TumorsmutalimNo ratings yet
- 4th Lecture HeadNeck and LympaticsDocument77 pages4th Lecture HeadNeck and LympaticsJeffrey Valdez Esteron100% (1)
- Elbow Complex (Kinesiology)Document2 pagesElbow Complex (Kinesiology)Kimmybee Garcia50% (2)
- DR - Rieva Kuliah 7 November - 2018Document38 pagesDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- Kamars RadiologyDocument135 pagesKamars RadiologyNayantara Nair100% (1)
- SCOLIOSISDocument19 pagesSCOLIOSISEspers BluesNo ratings yet
- 33-Hour Chick ReviewerDocument5 pages33-Hour Chick ReviewerBeatriceNo ratings yet
- Dumaguit (2021)Document12 pagesDumaguit (2021)Dimple May Gianne DumaguitNo ratings yet
- Clinical Features and Diagnosis of FracturesDocument43 pagesClinical Features and Diagnosis of FracturesChenna Kesava100% (2)
- Cranial NervesDocument16 pagesCranial Nervesapi-302547403100% (1)
- Development Urinary SystemDocument33 pagesDevelopment Urinary Systempavi7muruganathan75% (4)
- Rehabilitation of Cerebral Palsy & Motor DelayDocument49 pagesRehabilitation of Cerebral Palsy & Motor DelayasloocltNo ratings yet
- Radial Nerve Compression RaDocument28 pagesRadial Nerve Compression RaIndra RanteNo ratings yet
- Cervical SpondylosisDocument9 pagesCervical SpondylosisNurHidayah Borhanudin100% (1)
- Causes and Tests of Upper Cervical Spine PainDocument22 pagesCauses and Tests of Upper Cervical Spine PainiikemNo ratings yet
- Week 3 - PCPDocument3 pagesWeek 3 - PCPapi-479754549100% (1)
- ShoulderDocument51 pagesShoulderIts LaraNo ratings yet
- Deep Tendon Reflex Examination GuideDocument4 pagesDeep Tendon Reflex Examination GuideDan Ali100% (1)
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (2)
- Examination of Peripheral Nerves - RajaduraiDocument105 pagesExamination of Peripheral Nerves - RajadurairajaeasNo ratings yet
- Spine Examination: Mario Johan Heryputra 11.2012.208Document29 pagesSpine Examination: Mario Johan Heryputra 11.2012.208Mario Johan Heryputra100% (1)
- PCP Week 4 Workbook QuestionsDocument4 pagesPCP Week 4 Workbook Questionsapi-479717740No ratings yet
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Histology Final ExamDocument33 pagesHistology Final ExamAlok Kumar100% (3)
- Spine Fractures and Spinal Cord InjuryDocument54 pagesSpine Fractures and Spinal Cord InjuryAloy PudeNo ratings yet
- Splinting For Peripheral Nerve Injuries-PPT (2023)Document49 pagesSplinting For Peripheral Nerve Injuries-PPT (2023)KarisiNo ratings yet
- Low BackDocument7 pagesLow BackMuhammad FahmyNo ratings yet
- AP41 MDocument3 pagesAP41 Monix2000No ratings yet
- Elbow Special TestDocument4 pagesElbow Special TestEllaiza Astacaan100% (1)
- NERVE INJURIES: DIAGNOSIS, EVALUATION AND MANAGEMENTDocument80 pagesNERVE INJURIES: DIAGNOSIS, EVALUATION AND MANAGEMENTjothiNo ratings yet
- Soft tissue injury treatmentDocument2 pagesSoft tissue injury treatmentThiruNo ratings yet
- Cerebral Palsy Revalida FormatDocument10 pagesCerebral Palsy Revalida FormatChelsea CalanoNo ratings yet
- TANK Magazine #1Document146 pagesTANK Magazine #1stacarec100% (1)
- Activity No. 7 The Frog EmbryoDocument13 pagesActivity No. 7 The Frog EmbryoFerhaeeza KalayakanNo ratings yet
- Adult Reflexes GuideDocument4 pagesAdult Reflexes GuideChris Deinielle Marcoleta SumaoangNo ratings yet
- What Is PolymyositisDocument24 pagesWhat Is PolymyositisAshraf MobyNo ratings yet
- Peripheral Nerve Injury: Anatomy, Assessment, and Clinical FeaturesDocument54 pagesPeripheral Nerve Injury: Anatomy, Assessment, and Clinical FeaturesKarolle AlyssaNo ratings yet
- Peripheral Nerve Injury and Repair: Adam Osbourne, 5th Year MedicineDocument5 pagesPeripheral Nerve Injury and Repair: Adam Osbourne, 5th Year Medicineayrahma29No ratings yet
- Fracture Colles Rehabilitation Advice Following WristDocument4 pagesFracture Colles Rehabilitation Advice Following WristfaprilisaNo ratings yet
- Review of Literature PivdDocument5 pagesReview of Literature PivdPankaj VatsaNo ratings yet
- A Patient's Guide To Radial Tunnel SyndromeDocument4 pagesA Patient's Guide To Radial Tunnel SyndromeKarunya Vk100% (1)
- Referred PainDocument3 pagesReferred PainaspalavistaNo ratings yet
- Anatomy and Pathoanatomic of Lumbosacral PlexusDocument33 pagesAnatomy and Pathoanatomic of Lumbosacral PlexusRachmad FaisalNo ratings yet
- F - Proximal Ulnar Nerve Injury Correct AnswerDocument26 pagesF - Proximal Ulnar Nerve Injury Correct AnswerMehdi Hasan MazumderNo ratings yet
- MusculoskeletalDocument119 pagesMusculoskeletalEdissa PangilinanNo ratings yet
- Why Every Spine Fusion Can Be A Deformity?Document88 pagesWhy Every Spine Fusion Can Be A Deformity?PaulMcAfeeNo ratings yet
- Ultrasound of The Ankle: IndicationsDocument6 pagesUltrasound of The Ankle: IndicationsElloide PajutanNo ratings yet
- Amputation - Gait Deviations: Analysis of Transtibial (Below-Knee) Amputee GaitDocument9 pagesAmputation - Gait Deviations: Analysis of Transtibial (Below-Knee) Amputee GaitArchana MohantyNo ratings yet
- Hip Dislocation Reduction ManueverDocument6 pagesHip Dislocation Reduction ManueverAdam IrsyaddyraNo ratings yet
- Epidemiology: Phalanges and Interphalangeal JointsDocument4 pagesEpidemiology: Phalanges and Interphalangeal JointsHafidah RakhmatinaNo ratings yet
- Shoulder Knee WristDocument110 pagesShoulder Knee Wriststevebravo81100% (1)
- PNS Examination 15Document17 pagesPNS Examination 15NolanNo ratings yet
- My Fracture NotesDocument20 pagesMy Fracture NotesZai AkmaNo ratings yet
- Quadrilateral Space SyndromeDocument23 pagesQuadrilateral Space Syndromekashmala afzalNo ratings yet
- Shoulder ExamDocument24 pagesShoulder ExamMuhammad FahmyNo ratings yet
- Summary MRI Knee ImagingDocument17 pagesSummary MRI Knee ImagingSoban DaudNo ratings yet
- President's Address: Trick MovementsDocument3 pagesPresident's Address: Trick MovementsDr. Rushikesh K. Joshi100% (1)
- Knee ExaminationDocument17 pagesKnee ExaminationHaider GhazanfarNo ratings yet
- Entrapments CadDocument3 pagesEntrapments Cadapi-467743065100% (1)
- Thoracic and Lumbar Spine Anatomy: DR .S.NizamudeenDocument57 pagesThoracic and Lumbar Spine Anatomy: DR .S.NizamudeenPogo LocoNo ratings yet
- Fractures of Spine and Pelvis2007Document70 pagesFractures of Spine and Pelvis2007api-19916399No ratings yet
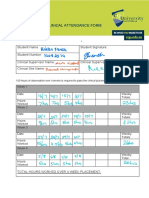
- Chir20002 Attendance Log Book - 1Document2 pagesChir20002 Attendance Log Book - 1api-479717740No ratings yet
- PCP ReflectionDocument3 pagesPCP Reflectionapi-479717740No ratings yet
- CASE STUDY AND QUESTIONS: To Be Completed by The 13 September Week 8 Case Study 8 AllanDocument11 pagesCASE STUDY AND QUESTIONS: To Be Completed by The 13 September Week 8 Case Study 8 Allanapi-479717740No ratings yet
- RofDocument2 pagesRofapi-479717740No ratings yet
- Case SummaryDocument4 pagesCase Summaryapi-479717740No ratings yet
- Rubric Reflective Portfolio 2020Document3 pagesRubric Reflective Portfolio 2020api-479717740No ratings yet
- PCP Reflection 2Document3 pagesPCP Reflection 2api-479717740No ratings yet
- Case Study 6 Chir13009Document12 pagesCase Study 6 Chir13009api-479717740No ratings yet
- Week 2 Case 2 Chir13009Document14 pagesWeek 2 Case 2 Chir13009api-479717740No ratings yet
- Week 5 Case Study Chir13009 Tutors NotesDocument8 pagesWeek 5 Case Study Chir13009 Tutors Notesapi-512652362No ratings yet
- Case Study 1 Chir13009Document6 pagesCase Study 1 Chir13009api-479717740No ratings yet
- Week 3 Case 3 Chir13009Document4 pagesWeek 3 Case 3 Chir13009api-479717740No ratings yet
- Week 9 Case Study 9 Chir13009Document8 pagesWeek 9 Case Study 9 Chir13009api-479717740No ratings yet
- Week 7 Case Study 7 Chir13009 Tutors NotesDocument11 pagesWeek 7 Case Study 7 Chir13009 Tutors Notesapi-477982644No ratings yet
- ReferencesDocument2 pagesReferencesapi-479717740No ratings yet
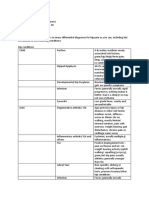
- Exercise 1 Differential ChartDocument6 pagesExercise 1 Differential Chartapi-479717740No ratings yet
- Week 5 Case Study Chir13009 Tutors NotesDocument8 pagesWeek 5 Case Study Chir13009 Tutors Notesapi-512652362No ratings yet
- Cluster SummaryDocument1 pageCluster Summaryapi-479717740No ratings yet
- Self-Directed Learning:: Holt-Oram SyndromeDocument3 pagesSelf-Directed Learning:: Holt-Oram Syndromeapi-479717740No ratings yet
- Week 8 PCP Workbook QuestionsDocument4 pagesWeek 8 PCP Workbook Questionsapi-479717740No ratings yet
- Portfolio Chir13008 - Assessment 1 Submission Addendum Form 2020 1 5Document2 pagesPortfolio Chir13008 - Assessment 1 Submission Addendum Form 2020 1 5api-512652362No ratings yet
- Exercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7Document4 pagesExercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7api-479717740No ratings yet
- Exercise 1: Problems)Document8 pagesExercise 1: Problems)api-479717740No ratings yet
- Exercise 1: Both Affect The Thoracolumbar Region Both Have Pain Felt Into The Top of The Sacrum and SijsDocument4 pagesExercise 1: Both Affect The Thoracolumbar Region Both Have Pain Felt Into The Top of The Sacrum and Sijsapi-479717740No ratings yet
- 4Document5 pages4api-479717740No ratings yet
- PCP Week 5 Workbook QuestionsDocument4 pagesPCP Week 5 Workbook Questionsapi-479717740No ratings yet
- Week 7 Workbook QuestionsDocument4 pagesWeek 7 Workbook Questionsapi-479717740No ratings yet
- 3Document3 pages3api-479717740No ratings yet
- PCP Week 3 Workbook QuestionsDocument5 pagesPCP Week 3 Workbook Questionsapi-479717740No ratings yet
- MCQS Developmental Biology QuestionsDocument4 pagesMCQS Developmental Biology QuestionsAima Iram BatoolNo ratings yet
- Embryology of EyeDocument28 pagesEmbryology of Eyesamuelpnrj25100% (2)
- Animal Developmental Biology Lecture Notes Lecture 1Document29 pagesAnimal Developmental Biology Lecture Notes Lecture 1Daniel MkenyaNo ratings yet
- Endoderm and DerivativesDocument3 pagesEndoderm and DerivativesCristian Giovanni Diaz PinoNo ratings yet
- Development of Head and NeckDocument5 pagesDevelopment of Head and NeckTobio KageyamaNo ratings yet
- Muscular SystemDocument18 pagesMuscular SystemAdan ImanNo ratings yet
- Essential Features of ProtochordatesDocument15 pagesEssential Features of ProtochordatesAriane DiongcoNo ratings yet
- Development of Embryo ChickDocument14 pagesDevelopment of Embryo ChickSafira Dwi OktavianiNo ratings yet
- Stem Cells ProjectDocument28 pagesStem Cells Projectshankar_demon hunterNo ratings yet
- Embryology - Science That Studies The Early Development and Formation of The OrganismDocument27 pagesEmbryology - Science That Studies The Early Development and Formation of The OrganismMeah PachecoNo ratings yet
- Prenatal Growth of Head and Face: Presented by Amritha. Vasudevan First Year PG Department of OrthodonticsDocument50 pagesPrenatal Growth of Head and Face: Presented by Amritha. Vasudevan First Year PG Department of OrthodonticsReenaChauhanNo ratings yet
- 1Document223 pages1Isaac Tan100% (2)
- Development of the GIT Part 1Document3 pagesDevelopment of the GIT Part 1Zade BawiNo ratings yet
- Esophagus - Anatomy and Development - GI Motility OnlineDocument21 pagesEsophagus - Anatomy and Development - GI Motility OnlineMaria Fernanda VargasNo ratings yet
- Ninja Nerd Embryology Notes CompleteDocument111 pagesNinja Nerd Embryology Notes Completezipporahwaithera404No ratings yet
- All Histology Semester 2 QuizzesDocument21 pagesAll Histology Semester 2 QuizzesBarwdi ZenNo ratings yet
- Ear Embryology: OtolaryngologyDocument8 pagesEar Embryology: OtolaryngologySuresh YadavNo ratings yet
- 4BBA1010 - Building A Human - 2022Document31 pages4BBA1010 - Building A Human - 2022Ritika ShresthaNo ratings yet
- Embriologie 2017Document100 pagesEmbriologie 2017Irina LutcanNo ratings yet
- IB Singh Human Embryology Part 2Document547 pagesIB Singh Human Embryology Part 2Rajeshwari RajiNo ratings yet
- REPRODocument48 pagesREPROARVIND KUMAR YADAVNo ratings yet
- Mnemonics Step 1Document4 pagesMnemonics Step 1Raji NaamaniNo ratings yet