You might also like
- Online FirstDocument8 pagesOnline FirstFranciscoNo ratings yet
- Relationship of Movement Screens With PastDocument7 pagesRelationship of Movement Screens With PastYoh ChenNo ratings yet
- Jeong 2021 Core Strength Training Can Alter NeDocument10 pagesJeong 2021 Core Strength Training Can Alter Nefrancosala2012No ratings yet
- Posterior Shoulder Tightness and Rotator Cuff Strength Assessments in Painful Shoulders of Amateur Tennis Players RBF 2013Document10 pagesPosterior Shoulder Tightness and Rotator Cuff Strength Assessments in Painful Shoulders of Amateur Tennis Players RBF 2013Michele GonçalvesNo ratings yet
- Relationships Between Functional Movement Tests and Performance Tests in Young Elite Male Basketball Players PDFDocument11 pagesRelationships Between Functional Movement Tests and Performance Tests in Young Elite Male Basketball Players PDFOriol Ruiz PujolNo ratings yet
- International Journal of Chemtech Research: Nabil .A. Mohamed and Maha. M. MohamedDocument11 pagesInternational Journal of Chemtech Research: Nabil .A. Mohamed and Maha. M. MohamedHari25885No ratings yet
- Newton2006 PDFDocument7 pagesNewton2006 PDFAlexandre FerreiraNo ratings yet
- Do Lower Limb Previous Injuries Affect Balance Performance - Sarto2019Document5 pagesDo Lower Limb Previous Injuries Affect Balance Performance - Sarto2019Jaime Fernandez FernandezNo ratings yet
- Kenya Luiz Artigo1- CorexombroDocument6 pagesKenya Luiz Artigo1- CorexombrolaurinhadeandradeNo ratings yet
- PM R - 2022 - Evidence For Isokinetic and Functional Testing in Return To Sport Decisions Following ACLDocument13 pagesPM R - 2022 - Evidence For Isokinetic and Functional Testing in Return To Sport Decisions Following ACLMu RakimNo ratings yet
- Biomechanical Comparison of Three Perceived Effort.10Document8 pagesBiomechanical Comparison of Three Perceived Effort.10Martiniano Vera EnriqueNo ratings yet
- 1 s2.0 S1440244021000554 Main PDFDocument9 pages1 s2.0 S1440244021000554 Main PDFEvelyn MalaguttiNo ratings yet
- A98 3 FullDocument2 pagesA98 3 FullHugo MaisNo ratings yet
- Neuromuscular Training Improves Single-Limb Stability in Young Female AthletesDocument12 pagesNeuromuscular Training Improves Single-Limb Stability in Young Female AthletesyarnlarbizimdirNo ratings yet
- 2008-Croisier-Strength Imbalances and Prevention of Hamstring Injury in Professional Soccer Players - Isokinetic HQ RatioDocument7 pages2008-Croisier-Strength Imbalances and Prevention of Hamstring Injury in Professional Soccer Players - Isokinetic HQ RatioFederico BristotNo ratings yet
- Prevention of Shoulder Injuries in Overhead AthletesDocument26 pagesPrevention of Shoulder Injuries in Overhead AthletesAmeerah KhraisatNo ratings yet
- 2021 Influence of invertor and evertor muscle fatigue on functional jump tests andDocument4 pages2021 Influence of invertor and evertor muscle fatigue on functional jump tests andktan.lboroNo ratings yet
- Jer 15 5 657 PDFDocument6 pagesJer 15 5 657 PDFÉomer LanNo ratings yet
- Jer 13 1 62Document6 pagesJer 13 1 62ceydaalyazhotamisNo ratings yet
- Back To Sports After Arthroscopic Revision Bankart Repair: Original ResearchDocument7 pagesBack To Sports After Arthroscopic Revision Bankart Repair: Original ResearchMiftahul IlmiNo ratings yet
- Assessments For Medical Discharge in Athlete Patients Undergoing Anterior Cruciate Ligament ReconstructionDocument4 pagesAssessments For Medical Discharge in Athlete Patients Undergoing Anterior Cruciate Ligament ReconstructionJhojan CARDONA PATIÑONo ratings yet
- Interesting Pilot StudyDocument11 pagesInteresting Pilot StudyjavierNo ratings yet
- SynopsisDocument28 pagesSynopsisTirumala RaoNo ratings yet
- Frequency+of+Shoulder+Pain+and+Functional+Level+Among+Overhead+Throwing+Athletes+at+Qayyum+Sports+Complex+Peshawar,+Pakistan+a+Descriptive+Cross Sectional+StudyDocument6 pagesFrequency+of+Shoulder+Pain+and+Functional+Level+Among+Overhead+Throwing+Athletes+at+Qayyum+Sports+Complex+Peshawar,+Pakistan+a+Descriptive+Cross Sectional+StudytahirahaniyaNo ratings yet
- J PTSP 2015 02 003Document26 pagesJ PTSP 2015 02 003Paula Pérez EspinosaNo ratings yet
- 233-Article Text-355-1-10-20200213Document17 pages233-Article Text-355-1-10-20200213Kristina ParasNo ratings yet
- The Effects of Neuromuscular Training On Knee Joint MOTOR ControlDocument9 pagesThe Effects of Neuromuscular Training On Knee Joint MOTOR ControlalmaformaNo ratings yet
- Soccer Fuerza en PiernasDocument10 pagesSoccer Fuerza en PiernasArturo Osorio GtzNo ratings yet
- Balance-And Strength-Training Protocols To Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome MeasuresDocument10 pagesBalance-And Strength-Training Protocols To Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome MeasuresGorkaBuesaNo ratings yet
- Orthop J Sports Med 2021 9 7 23259671211013394Document6 pagesOrthop J Sports Med 2021 9 7 23259671211013394Fernando SousaNo ratings yet
- Role of Neuromuscular Control of Postural and Core Stability in Functional MVTDocument21 pagesRole of Neuromuscular Control of Postural and Core Stability in Functional MVTmaryroy7No ratings yet
- An Electromyographical Analysis of Sumo and Conventional Style DeadliftsDocument8 pagesAn Electromyographical Analysis of Sumo and Conventional Style DeadliftsRafael EscamillaNo ratings yet
- Regional Interdependence of The Hip andDocument12 pagesRegional Interdependence of The Hip andYoh ChenNo ratings yet
- Andrade Et Al., 2014Document7 pagesAndrade Et Al., 2014Lívia PogettiNo ratings yet
- Apiv1articles27975 The Neuromuscular Effects of The Copenhagen Adductor Exercise A SystematicDocument12 pagesApiv1articles27975 The Neuromuscular Effects of The Copenhagen Adductor Exercise A SystematicItamar CarvalhoNo ratings yet
- Sports 11 00218Document12 pagesSports 11 00218Than TsafNo ratings yet
- Scholes 2021Document10 pagesScholes 2021Jayne PereiraNo ratings yet
- Analysis of Joint Injuries and Movement Skills in College Basketballrevista Brasileira de Medicina Do EsporteDocument4 pagesAnalysis of Joint Injuries and Movement Skills in College Basketballrevista Brasileira de Medicina Do EsporteMafer GarcíaNo ratings yet
- Kelompok 01Document7 pagesKelompok 01KharisulNo ratings yet
- Preventing shoulder injuries in overhead athletesDocument9 pagesPreventing shoulder injuries in overhead athletesLeonardiniNo ratings yet
- A Clinical Review of Return-to-Play Considerations After Anterior Shoulder DislocationDocument6 pagesA Clinical Review of Return-to-Play Considerations After Anterior Shoulder DislocationThyago AraujoNo ratings yet
- Prediction of Knee Injuries in Soccer Using Core StrengthDocument8 pagesPrediction of Knee Injuries in Soccer Using Core StrengthQuenton CompasNo ratings yet
- Physical Therapy in Sport: Margie Olds, Cade Coulter, Dan Marant, Tim UhlDocument7 pagesPhysical Therapy in Sport: Margie Olds, Cade Coulter, Dan Marant, Tim UhlNicol SandovalNo ratings yet
- Stress Relaxation and Targeted Nutrition To Treat Patellar TendinopathyDocument5 pagesStress Relaxation and Targeted Nutrition To Treat Patellar TendinopathyhectorNo ratings yet
- 36 Physiological and Performance TestingDocument2 pages36 Physiological and Performance TestingWhooper GamestorNo ratings yet
- Physical Therapy in Sport: Suzi Edwards, Hiram C. Brooke, Jill L. CookDocument9 pagesPhysical Therapy in Sport: Suzi Edwards, Hiram C. Brooke, Jill L. CookLing Pong HungNo ratings yet
- Lca PDFDocument6 pagesLca PDFPedro CespedesNo ratings yet
- Artigo 5Document5 pagesArtigo 5Jailson CamposNo ratings yet
- An Electromyographic Analysis of Sumo And.19Document7 pagesAn Electromyographic Analysis of Sumo And.19JulianoEscudeiroNo ratings yet
- Colomaretal.2022.DeterminantPhysicalFactorsofTennisServeVelocity ABriefReviewDocument12 pagesColomaretal.2022.DeterminantPhysicalFactorsofTennisServeVelocity ABriefReviewValerio PolidoriNo ratings yet
- Comparing Shoulder Joint Functional Range of Motion in Overhead Athletes With and Without Shoulder Impingement Syndrome: A Cross-Sectional StudyDocument5 pagesComparing Shoulder Joint Functional Range of Motion in Overhead Athletes With and Without Shoulder Impingement Syndrome: A Cross-Sectional Studypedrovsky702No ratings yet
- Effects of Inter Limb AsymmetriesDocument24 pagesEffects of Inter Limb AsymmetriesTadija TrajkovićNo ratings yet
- Six Weeks of Core Stability Training Improves Landing KineticsDocument11 pagesSix Weeks of Core Stability Training Improves Landing KineticsDANILO CARVALHO X-TRAINERNo ratings yet
- The Association Among Trunk Rotation Ball Velocity and The Elbow Varus Moment in Collegiate Level Baseball PitchersDocument5 pagesThe Association Among Trunk Rotation Ball Velocity and The Elbow Varus Moment in Collegiate Level Baseball PitcherservoNo ratings yet
- Improving Single-Legged-Squat Performance: Comparing 2 Training Methods With Potential Implications For Injury PreventionDocument9 pagesImproving Single-Legged-Squat Performance: Comparing 2 Training Methods With Potential Implications For Injury PreventionSamuelNo ratings yet
- Alterations in Peak Ground-Reaction Force During 60-cm Drop Landings Caused by A Single Session of Repeated Wingate Anaerobic TestsDocument7 pagesAlterations in Peak Ground-Reaction Force During 60-cm Drop Landings Caused by A Single Session of Repeated Wingate Anaerobic TestsIlham MaulanaNo ratings yet
- Dynamic TrunkDocument19 pagesDynamic TrunkSwissjust ADNo ratings yet
- Assessing The Effectiveness of Neuromuscular Training Programs in Reducing The Incidence of Anterior Cruciate Ligament Injuries in Female AthletesDocument9 pagesAssessing The Effectiveness of Neuromuscular Training Programs in Reducing The Incidence of Anterior Cruciate Ligament Injuries in Female AthletesCamila GuevaraNo ratings yet
- SEBT As A Predictor of Lower Extremity Injury in High School Basketball PlayersDocument9 pagesSEBT As A Predictor of Lower Extremity Injury in High School Basketball PlayersFebryLasantiNo ratings yet
- Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990-2019 - A Systematic Analysis For The Global Burden of Disease Study 2019Document27 pagesGlobal Burden of 87 Risk Factors in 204 Countries and Territories, 1990-2019 - A Systematic Analysis For The Global Burden of Disease Study 2019GoranMarkovicNo ratings yet
- Death by Effectiveness: Exercise As Medicine Caught in The Ef Ficacy Trap!Document2 pagesDeath by Effectiveness: Exercise As Medicine Caught in The Ef Ficacy Trap!Martijn JohanNo ratings yet
- UEFA Expert Group Statement On Nutrition in Elite Football. Current Evidence To Inform Practical Recommendations and Guide Future ResearchDocument27 pagesUEFA Expert Group Statement On Nutrition in Elite Football. Current Evidence To Inform Practical Recommendations and Guide Future ResearchGoranMarkovicNo ratings yet
- The Dominant Leg Is More Likely To Get Injured in Soccer Players - Systematic Review and Meta-AnalysisDocument39 pagesThe Dominant Leg Is More Likely To Get Injured in Soccer Players - Systematic Review and Meta-AnalysisGoranMarkovicNo ratings yet
- The Australian Institute of Sport (AIS) and National Eating Disorders Collaboration (NEDC) Position Statement On Disordered Eating in High Performance Sport PDFDocument13 pagesThe Australian Institute of Sport (AIS) and National Eating Disorders Collaboration (NEDC) Position Statement On Disordered Eating in High Performance Sport PDFGoranMarkovicNo ratings yet
- Training The Antifragile Athlete - A Preliminary Analysis of Neuromuscular Training Effects On Muscle Activation DynamicsDocument22 pagesTraining The Antifragile Athlete - A Preliminary Analysis of Neuromuscular Training Effects On Muscle Activation DynamicsGoranMarkovicNo ratings yet
- Resistance Training and Health in Adults - An Overview of Systematic ReviewsDocument15 pagesResistance Training and Health in Adults - An Overview of Systematic ReviewsGoranMarkovicNo ratings yet
- Staying Physically Active During The Quarantine and Self-Isolation Period For Controlling and Mitigating The COVID-19 Pandemic - A Systematic Overview of The LiteratureDocument11 pagesStaying Physically Active During The Quarantine and Self-Isolation Period For Controlling and Mitigating The COVID-19 Pandemic - A Systematic Overview of The LiteratureGoranMarkovicNo ratings yet
- Trajectories of Adolescent Life Satisfaction - PreprintDocument14 pagesTrajectories of Adolescent Life Satisfaction - PreprintGoranMarkovicNo ratings yet
- Passive Versus Active Recovery During High-Intensity Intermittent ExercisesDocument8 pagesPassive Versus Active Recovery During High-Intensity Intermittent ExercisesGoranMarkovicNo ratings yet
- The revolutionary technology that maximizes therapeutic effectiveness and speedDocument16 pagesThe revolutionary technology that maximizes therapeutic effectiveness and speedGoranMarkovicNo ratings yet
- History of Physical Activity Recommendations and Guidelines For AmericansDocument22 pagesHistory of Physical Activity Recommendations and Guidelines For AmericansGoranMarkovicNo ratings yet
- Digital Transformation Course BrochureDocument19 pagesDigital Transformation Course BrochureGoranMarkovicNo ratings yet
- Classification of Lumbopelvic-Hip Complex Instability On Kinematics Amongst Female Team Handball Athletes PDFDocument6 pagesClassification of Lumbopelvic-Hip Complex Instability On Kinematics Amongst Female Team Handball Athletes PDFGoranMarkovicNo ratings yet
- The Relationship Between Asymmetry and Athletic Performance - A Critical ReviewDocument15 pagesThe Relationship Between Asymmetry and Athletic Performance - A Critical ReviewGoranMarkovicNo ratings yet
- Classification of Lumbopelvic-Hip Complex Instability On Kinematics Amongst Female Team Handball Athletes PDFDocument6 pagesClassification of Lumbopelvic-Hip Complex Instability On Kinematics Amongst Female Team Handball Athletes PDFGoranMarkovicNo ratings yet
- BFR Systematic ReviewDocument7 pagesBFR Systematic ReviewGoranMarkovicNo ratings yet
- Tendinopathy CourseDocument3 pagesTendinopathy CourseGoranMarkovicNo ratings yet
- A Review of Research On The Mechanical Stiffness in Running and Jumping - Methodology and ImplicationsDocument10 pagesA Review of Research On The Mechanical Stiffness in Running and Jumping - Methodology and ImplicationsGoranMarkovicNo ratings yet
- A Profile of Sports Science Research (1983-2003)Document8 pagesA Profile of Sports Science Research (1983-2003)GoranMarkovicNo ratings yet
- 200th Anniversary of Lactate Research in Muscle PDFDocument7 pages200th Anniversary of Lactate Research in Muscle PDFGoranMarkovicNo ratings yet
- A Method To Evaluate Reflex Excitability of The Human Ankle Plantarflexors Despite Changes in Maximal Activation CapacitiesDocument11 pagesA Method To Evaluate Reflex Excitability of The Human Ankle Plantarflexors Despite Changes in Maximal Activation CapacitiesGoranMarkovicNo ratings yet
- Fundamental Concepts in StatisticsDocument12 pagesFundamental Concepts in StatisticsGoranMarkovicNo ratings yet
- 200th Anniversary of Lactate Research in Muscle PDFDocument7 pages200th Anniversary of Lactate Research in Muscle PDFGoranMarkovicNo ratings yet
- Water Immersion Recovery For Athletes - Effect On Exercise Performance and Practical RecommendationsDocument32 pagesWater Immersion Recovery For Athletes - Effect On Exercise Performance and Practical RecommendationsGoranMarkovicNo ratings yet
- Bland, J.M & Altman, D.G. (2002) Validating Scales and Indexes PDFDocument2 pagesBland, J.M & Altman, D.G. (2002) Validating Scales and Indexes PDFCésarAugustoSantanaNo ratings yet
- Core Control Vs Core Strengt Training - What Is The DifferenceDocument2 pagesCore Control Vs Core Strengt Training - What Is The DifferenceGoranMarkovicNo ratings yet
- Train Pelvic Floor MusclesDocument1 pageTrain Pelvic Floor MusclesGoranMarkovic100% (1)
- Multifidi TrainingDocument1 pageMultifidi TrainingGoranMarkovic100% (1)
- Potential of various fatty feeds to reduce methane release from rumen fermentation in vitroDocument14 pagesPotential of various fatty feeds to reduce methane release from rumen fermentation in vitroGabriela Casarotto DanielNo ratings yet
- Treatment of DepressionDocument350 pagesTreatment of DepressionoskarNewNo ratings yet
- NASKAH-PUBLIKASI (1) Nanot HalamanDocument13 pagesNASKAH-PUBLIKASI (1) Nanot HalamanNurul FitrianiNo ratings yet
- Quality Life Scale PDFDocument7 pagesQuality Life Scale PDFFayza RihastaraNo ratings yet
- Uts ReadingDocument7 pagesUts ReadingLaisah IdrNo ratings yet
- Effects of Child AbuseDocument38 pagesEffects of Child AbuseChristopher Baccay84% (19)
- Re-Opening Plan For The 2020-2021 School YearDocument18 pagesRe-Opening Plan For The 2020-2021 School YearNews 8 WROCNo ratings yet
- 2020 International Society of Hypertension Global Hypertension Practice GuidelinesDocument15 pages2020 International Society of Hypertension Global Hypertension Practice GuidelinesIntan PermatasariNo ratings yet
- VR Hackers - Risk Assesment Hacking-2Document3 pagesVR Hackers - Risk Assesment Hacking-2Vikas RameshNo ratings yet
- Passion Project Action PlanDocument3 pagesPassion Project Action PlanMeresa W. MartinNo ratings yet
- Best Body FitnessDocument3 pagesBest Body FitnessLavinia Chirila-StefanutNo ratings yet
- NGYouthSDGs PlaybookDocument50 pagesNGYouthSDGs PlaybookLaura noguesNo ratings yet
- 20 Đề tham khảo tuyển sinh vào lớp 10 2022Document87 pages20 Đề tham khảo tuyển sinh vào lớp 10 2022nguyethuhang.hnNo ratings yet
- Trainee's Record Book SWBLDocument12 pagesTrainee's Record Book SWBLaaronjules100% (2)
- Government Issues Relief Guidelines for Victims of AtrocitiesDocument4 pagesGovernment Issues Relief Guidelines for Victims of AtrocitiesDept . WD&CW Andhra PradeshNo ratings yet
- House Democratic Caucus Task Force On Aging and Families LTR To Biden Harris Transition - Geriatrician To COVID Advisory BoardDocument2 pagesHouse Democratic Caucus Task Force On Aging and Families LTR To Biden Harris Transition - Geriatrician To COVID Advisory BoardPeter SullivanNo ratings yet
- 10 Things I Would Do If I Were A CelebrityDocument3 pages10 Things I Would Do If I Were A CelebrityAnne Marian JosephNo ratings yet
- Prasnottara English For AmazonDocument127 pagesPrasnottara English For AmazonAnand PendyalaNo ratings yet
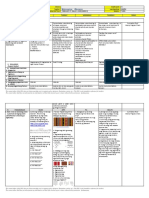
- MAPEH Daily Lesson LogDocument11 pagesMAPEH Daily Lesson LogMARTIN YUI LOPEZNo ratings yet
- The Best Lifts For Real World Strength & Strongman CompetitionDocument3 pagesThe Best Lifts For Real World Strength & Strongman CompetitionIlijaNo ratings yet
- Nursing Board Exam Answer Key and Test QuestionsDocument44 pagesNursing Board Exam Answer Key and Test Questionsrem_cen24100% (1)
- Decision MakingDocument19 pagesDecision MakingJeph ToholNo ratings yet
- Timeless Beauty - Over 100 Tips, Secrets, and Shortcuts To Looking Great (PDFDrive)Document488 pagesTimeless Beauty - Over 100 Tips, Secrets, and Shortcuts To Looking Great (PDFDrive)Isabel Matta100% (1)
- EDocument56 pagesEimee tan100% (3)
- 2022醫療急救 無線電醫療作業Document2 pages2022醫療急救 無線電醫療作業Yu-ting FengNo ratings yet
- Medication AdministrationDocument61 pagesMedication Administrationkerema BadasaNo ratings yet
- Healthlittoolkit2 Tool2aDocument7 pagesHealthlittoolkit2 Tool2aRenzz Irven PlotadoNo ratings yet
- Assessing Animal Housing and Management in a LaboratoryDocument22 pagesAssessing Animal Housing and Management in a Laboratoryrifky waskitoNo ratings yet
- ADEC - Al Murooj Scientific Private School 2015 2016Document16 pagesADEC - Al Murooj Scientific Private School 2015 2016Edarabia.comNo ratings yet
- End of Life Care GuideDocument79 pagesEnd of Life Care GuideAbcd TolibasNo ratings yet