You might also like
- Carr and Latham's Technology of Clothing ManufactureFrom EverandCarr and Latham's Technology of Clothing ManufactureDavid J. TylerRating: 4 out of 5 stars4/5 (1)
- Medical TextilesDocument32 pagesMedical TextilesBabar Ramzan0% (1)
- Medical Textiles Final Merge PDFDocument48 pagesMedical Textiles Final Merge PDFMK ChemistNo ratings yet
- Designed, Tested and Trusted by Operating Theatre ProfessionalsDocument5 pagesDesigned, Tested and Trusted by Operating Theatre ProfessionalsYusuf Selim ErkenNo ratings yet
- E Hakko General PDFDocument97 pagesE Hakko General PDFSilver SelwayneNo ratings yet
- Stability Data Package for Climatic Zones III and IVDocument5 pagesStability Data Package for Climatic Zones III and IVSailaja Chirravuri100% (1)
- Brucella IgG ELISA detects antibodiesDocument32 pagesBrucella IgG ELISA detects antibodiesIvanNo ratings yet
- Sample Collection VMCDocument11 pagesSample Collection VMCAnuj TewariNo ratings yet
- Product Catalogue: Eastern Europe, Middle East and AfricaDocument130 pagesProduct Catalogue: Eastern Europe, Middle East and AfricaRABAH BOUCHELAGHEMNo ratings yet
- An4364 PDFDocument34 pagesAn4364 PDFjoseluisblanco69No ratings yet
- QA Standards for Domestics & TextilesDocument34 pagesQA Standards for Domestics & TextilesDeepak ThakkerNo ratings yet
- Appointment Letter of MRDocument1 pageAppointment Letter of MRshalinmishraNo ratings yet
- SOP ELISA Edinburgh PDFDocument3 pagesSOP ELISA Edinburgh PDFmofak haesNo ratings yet
- Agappe Chitra Magna IFU 14 May PDFDocument2 pagesAgappe Chitra Magna IFU 14 May PDFDharmesh PatelNo ratings yet
- 3m Sterigage PDFDocument4 pages3m Sterigage PDFARIKANo ratings yet
- Surgical Drapes, Gowns and Clean Air Suits, Used As Medical Devices For Patients, Clinical Staff and Equipment - Part 3: Performance RequirementsDocument7 pagesSurgical Drapes, Gowns and Clean Air Suits, Used As Medical Devices For Patients, Clinical Staff and Equipment - Part 3: Performance RequirementsÖzer KöseNo ratings yet
- P146 Cord Lug A 1XDocument0 pagesP146 Cord Lug A 1XAnish KumarNo ratings yet
- Guidance Document For Regulatory Approvals of Stem Cell and Cell Based Products (SCCPS)Document108 pagesGuidance Document For Regulatory Approvals of Stem Cell and Cell Based Products (SCCPS)Shashank Tiwari100% (2)
- Importance of Quality Control in Textile and Apparel IndustryDocument6 pagesImportance of Quality Control in Textile and Apparel IndustryMasudul Alam SajibNo ratings yet
- Surgeine Disposable Gown Drape CatalogueDocument8 pagesSurgeine Disposable Gown Drape CataloguebhawneshNo ratings yet
- Format BondDocument2 pagesFormat BondSagar GuptaNo ratings yet
- Meditech Textiles Mid-Term AssignmentDocument10 pagesMeditech Textiles Mid-Term AssignmentarushiparasharNo ratings yet
- EN 455-2 - 2015 - Medical Gloves For Single Use - Part 2 Requirements and TestingDocument11 pagesEN 455-2 - 2015 - Medical Gloves For Single Use - Part 2 Requirements and Testingmargarida100% (2)
- Healthcare Laundry and Textiles in The United States: Review and Commentary On Contemporary Infection Prevention IssuesDocument16 pagesHealthcare Laundry and Textiles in The United States: Review and Commentary On Contemporary Infection Prevention IssuesMoriaNo ratings yet
- Medical Coating Innovations - NEW PDFDocument2 pagesMedical Coating Innovations - NEW PDFleonardq1No ratings yet
- Iso Astm 51205-17Document11 pagesIso Astm 51205-17Oh No PotatoNo ratings yet
- Unit 1 Functional GarmentsDocument60 pagesUnit 1 Functional GarmentsSivakumar KNo ratings yet
- Report On KnitwearDocument5 pagesReport On KnitwearHSNo ratings yet
- Textile and Apparel Quality EvaluationDocument65 pagesTextile and Apparel Quality EvaluationvasineyNo ratings yet
- Dry Cleaning Fastness TestDocument5 pagesDry Cleaning Fastness TestAkriti Dixit0% (1)
- SWOT Analysis of Indian Apparel & Textile Industry: Raw Material BaseDocument3 pagesSWOT Analysis of Indian Apparel & Textile Industry: Raw Material BaseAnonymous UoRu4sNo ratings yet
- YETI - Product Manual (00000002)Document35 pagesYETI - Product Manual (00000002)vesalocalbusNo ratings yet
- Textile Industry Internship ReportDocument6 pagesTextile Industry Internship ReportPiyush PatelNo ratings yet
- Presentation by MR Shishir Jaipuria On MeditechDocument20 pagesPresentation by MR Shishir Jaipuria On Meditechsathish_20102010No ratings yet
- Publications: Fibre & YarnDocument14 pagesPublications: Fibre & YarnvigneshbalajirsNo ratings yet
- Medica L Textile S: Click To Edit Master Subtitle StyleDocument24 pagesMedica L Textile S: Click To Edit Master Subtitle StyleShazzad HossaIn100% (1)
- SwotDocument3 pagesSwotSushila SahaniNo ratings yet
- Resume SockDocument5 pagesResume Sockrhinorame6801No ratings yet
- Point System For Evaluating Quality in TextilesDocument115 pagesPoint System For Evaluating Quality in TextilesBenjamin OchoaNo ratings yet
- Sewn Products Machinery and Equipment - II (Pre & Post Production Machines & Equipment)Document14 pagesSewn Products Machinery and Equipment - II (Pre & Post Production Machines & Equipment)Suganya ArumugamNo ratings yet
- SMEDA Absorbent CottonDocument22 pagesSMEDA Absorbent CottonManohar Waghela100% (2)
- Formal Trouser: Feasibility Report PresentationDocument64 pagesFormal Trouser: Feasibility Report Presentationbolaaajiii100% (1)
- Garments LabelDocument7 pagesGarments LabelDeluar HossainNo ratings yet
- Medical Face Masks - Requirements and Test Methods: BSI Standards PublicationDocument24 pagesMedical Face Masks - Requirements and Test Methods: BSI Standards PublicationCindy Fonseca100% (1)
- Cardiac Puncture Blood Collection TerminalDocument1 pageCardiac Puncture Blood Collection TerminalSuzana VoiculescuNo ratings yet
- Research ProposalDocument5 pagesResearch ProposalRonak RajpurohitNo ratings yet
- Vastram ExportsDocument40 pagesVastram ExportsHarsha DuraiNo ratings yet
- Stree MGMT of T.C Terrytex Ltd.Document55 pagesStree MGMT of T.C Terrytex Ltd.Mahfooz IlahiNo ratings yet
- 1-Day Awareness Course On Co$T of Quality: Presented by Neville-Clarke InternationalDocument85 pages1-Day Awareness Course On Co$T of Quality: Presented by Neville-Clarke Internationaldyogasara2No ratings yet
- 2 1 6 Defect ListDocument7 pages2 1 6 Defect Listvivek jangraNo ratings yet
- MATERIAL Mig ExplanationDocument86 pagesMATERIAL Mig ExplanationGeorgia KyriakidouNo ratings yet
- Qualification Pack - Sewing Machine Operator - Level 4-1Document38 pagesQualification Pack - Sewing Machine Operator - Level 4-1sp1955No ratings yet
- Final Report - Expedite The Laboratory Investigation of Covid19 Ravi KumudeshDocument33 pagesFinal Report - Expedite The Laboratory Investigation of Covid19 Ravi KumudeshRavi KumudeshNo ratings yet
- Features and benefits of modular production systemsDocument2 pagesFeatures and benefits of modular production systemsDrBollapu SudarshanNo ratings yet
- Textile industry checklistDocument112 pagesTextile industry checklistNarender Mehra SethNo ratings yet
- Quality Control in WeavingDocument10 pagesQuality Control in WeavingnayeemNo ratings yet
- Anti Treatment Knits PrintDocument22 pagesAnti Treatment Knits Printn.tNo ratings yet
- 1526967206H08TM08 QiDocument15 pages1526967206H08TM08 QiJhilik Dey100% (1)
- Technical Textile A Promising FutureDocument22 pagesTechnical Textile A Promising FutureDr Muhammad Mushtaq Mangat100% (1)
- A Dressing HistoryDocument17 pagesA Dressing HistoryEtn CentreNo ratings yet
- Al Kabir Plot WorkingDocument2 pagesAl Kabir Plot WorkingArslan ShaukatNo ratings yet
- 5s Final PPT For 10-10-14Document62 pages5s Final PPT For 10-10-14Arslan ShaukatNo ratings yet
- N95 NIOSH Moulded MaskDocument13 pagesN95 NIOSH Moulded MaskArslan ShaukatNo ratings yet
- Sampling Procedures and Tables For Inspection Ansi Asq z1 4 2008 PDFDocument96 pagesSampling Procedures and Tables For Inspection Ansi Asq z1 4 2008 PDFjmmfbeijos100% (4)
- N95 NIOSH Moulded MaskDocument13 pagesN95 NIOSH Moulded MaskArslan ShaukatNo ratings yet
- Munsell Color SystemDocument24 pagesMunsell Color SystemKate Mijares DalitNo ratings yet
- Wcms 228220Document166 pagesWcms 228220ranjann349No ratings yet
- MasksDocument4 pagesMasksArslan ShaukatNo ratings yet
- Quality MGT in Garments Industry of BangladeshDocument8 pagesQuality MGT in Garments Industry of BangladeshRefat Rasul ChowdhuryNo ratings yet
- 5 Nadeem AfrazDocument19 pages5 Nadeem AfrazArslan ShaukatNo ratings yet
- Minimizing Seam Slippage 2-12-10Document2 pagesMinimizing Seam Slippage 2-12-10Arslan ShaukatNo ratings yet
- Detailed Study On MangosDocument18 pagesDetailed Study On MangosArslan Shaukat100% (1)
- Fabcons1 4986-1Document1 pageFabcons1 4986-1Arslan ShaukatNo ratings yet
- Pak-USAID Merit and Needs Based Scholarship Program: Brief HistoryDocument2 pagesPak-USAID Merit and Needs Based Scholarship Program: Brief HistoryArslan ShaukatNo ratings yet
- Bleach Strength TestDocument8 pagesBleach Strength TestArslan ShaukatNo ratings yet
- Muhammad-Asif Process CapabilityDocument29 pagesMuhammad-Asif Process CapabilityJehan B KothariNo ratings yet
- 5 Nadeem AfrazDocument19 pages5 Nadeem AfrazArslan ShaukatNo ratings yet
- OLS ReportCTTGroupDocument7 pagesOLS ReportCTTGroupArslan ShaukatNo ratings yet
- Evaluative Criteria - Denim Design JournalDocument21 pagesEvaluative Criteria - Denim Design JournalArslan ShaukatNo ratings yet
- Denim Garment Processing TechniquesDocument14 pagesDenim Garment Processing TechniquesMudassar AliNo ratings yet
- Acid Wash:: First Step: Pretreatment/DesizingDocument14 pagesAcid Wash:: First Step: Pretreatment/DesizingArslan ShaukatNo ratings yet
- Breathless For Blue Jeans, 2013Document40 pagesBreathless For Blue Jeans, 2013Arslan ShaukatNo ratings yet
- Apparel Glossary 08Document3 pagesApparel Glossary 08Arslan ShaukatNo ratings yet
- Dirty Laundry - 全球服裝品牌的中國水污染調查 - EN - 11-07-13Document116 pagesDirty Laundry - 全球服裝品牌的中國水污染調查 - EN - 11-07-13xtrayangNo ratings yet
- National Institute of Fashion Technology Hyderabad Fabric and garment finishing : Basic washes in denim fabricDocument13 pagesNational Institute of Fashion Technology Hyderabad Fabric and garment finishing : Basic washes in denim fabricSundaramoorthy ManickamNo ratings yet
- CrochetBB Beans and Bobbles Chevron Afghan Pattern by Jeanne Steinhilber PDFDocument2 pagesCrochetBB Beans and Bobbles Chevron Afghan Pattern by Jeanne Steinhilber PDFMelodi OlsonNo ratings yet
- Alpine Bloom Final 1.0Document10 pagesAlpine Bloom Final 1.0Ale Jimenez100% (4)
- DLL - Tle-He 6 - Q3 - W6Document4 pagesDLL - Tle-He 6 - Q3 - W6Allyza Fae DavidNo ratings yet
- B.SC Hons in AMT Syllabus Pub Date 16022022Document60 pagesB.SC Hons in AMT Syllabus Pub Date 16022022Tonmoy PaulNo ratings yet
- Hummel 2022Document244 pagesHummel 2022Cris SuteraNo ratings yet
- Manual PT SPSD-BH6000-02Document62 pagesManual PT SPSD-BH6000-02ricardo assaf marchetiNo ratings yet
- Apparel CategoriesDocument52 pagesApparel CategoriesAneesha PandaNo ratings yet
- How To Use Greist AttachmentsDocument36 pagesHow To Use Greist Attachmentsfmaria64100% (9)
- Action Plan of Finishing SupervisorDocument2 pagesAction Plan of Finishing SupervisorSayed Aasim JawaidNo ratings yet
- Fabric IdentificationDocument26 pagesFabric IdentificationSmita PoojaryNo ratings yet
- Beximco Textile Ltd Project Description Chapter 1Document63 pagesBeximco Textile Ltd Project Description Chapter 1Ashraf ChowdhuryNo ratings yet
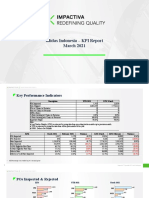
- Adidas Indonesia - KPI Report March 2021Document13 pagesAdidas Indonesia - KPI Report March 2021Manmohan KumarNo ratings yet
- Avy Doll Crochet PatternDocument45 pagesAvy Doll Crochet PatternLia Vágvölgyi73% (11)
- Apparel 10 PDFDocument253 pagesApparel 10 PDFRasheed AdewaleNo ratings yet
- Pallet ProposalDocument6 pagesPallet Proposalapi-540583277No ratings yet
- OverLock MachineDocument13 pagesOverLock MachineAhnaf ZahinNo ratings yet
- Surprise Egg With Little LambDocument11 pagesSurprise Egg With Little Lambmagy4alex4min4100% (4)
- Madeira PK EngDocument48 pagesMadeira PK EngRca Maquinas EngenhariaNo ratings yet
- Jury WorkDocument25 pagesJury WorkSatadeep DattaNo ratings yet
- Mechanical Finishing of NonwovensDocument23 pagesMechanical Finishing of Nonwovensmahes_tex100% (1)
- Manos Del Uruguay Thunder + Lightning HatDocument2 pagesManos Del Uruguay Thunder + Lightning HatÉrika BatistaNo ratings yet
- MDF248 Brando Pattern PDFDocument20 pagesMDF248 Brando Pattern PDFLUCERO VALERY CASTILLO VASQUEZNo ratings yet
- Group 8 - Balenciaga + Trend SpottingDocument69 pagesGroup 8 - Balenciaga + Trend SpottingShivam BhandariNo ratings yet
- Brother M945 Super Ace III Quick GuideDocument4 pagesBrother M945 Super Ace III Quick GuideAmiNo ratings yet
- Singer Professional 5: Overlock WorkbookDocument238 pagesSinger Professional 5: Overlock WorkbookTasheenaNo ratings yet
- Sad Presentation 1Document14 pagesSad Presentation 1nikhilbajpai_88No ratings yet
- 4 Arts and Crafts of Mindanao: ScoreDocument11 pages4 Arts and Crafts of Mindanao: ScoreCryzel MuniNo ratings yet
- STOLL1Document19 pagesSTOLL1Alex AnikNo ratings yet
- Macramé Group 1 Project DocumentDocument36 pagesMacramé Group 1 Project DocumentCarl Laura Climaco100% (1)
- EuniceTheUnicorn TLHdigital - Postar 2Document16 pagesEuniceTheUnicorn TLHdigital - Postar 2khuyên nguyễn100% (4)
- Self-Care for Men: How to Look Good and Feel GreatFrom EverandSelf-Care for Men: How to Look Good and Feel GreatRating: 4 out of 5 stars4/5 (4)
- Bulletproof Seduction: How to Be the Man That Women Really WantFrom EverandBulletproof Seduction: How to Be the Man That Women Really WantRating: 4.5 out of 5 stars4.5/5 (168)
- The Kingdom of Prep: The Inside Story of the Rise and (Near) Fall of J.CrewFrom EverandThe Kingdom of Prep: The Inside Story of the Rise and (Near) Fall of J.CrewRating: 4.5 out of 5 stars4.5/5 (25)
- A Healthy You: Boost Your Energy, Live Cleaner, and Look and Feel Younger Every DayFrom EverandA Healthy You: Boost Your Energy, Live Cleaner, and Look and Feel Younger Every DayRating: 3 out of 5 stars3/5 (1)
- How to Dress: Secret styling tips from a fashion insiderFrom EverandHow to Dress: Secret styling tips from a fashion insiderRating: 4 out of 5 stars4/5 (1)
- Emily Post's Etiquette in Society, in Business, in Politics, and at HomeFrom EverandEmily Post's Etiquette in Society, in Business, in Politics, and at HomeRating: 4 out of 5 stars4/5 (59)
- The Basics of Corset Building: A Handbook for BeginnersFrom EverandThe Basics of Corset Building: A Handbook for BeginnersRating: 4.5 out of 5 stars4.5/5 (17)
- Metric Pattern Cutting for Women's WearFrom EverandMetric Pattern Cutting for Women's WearRating: 4.5 out of 5 stars4.5/5 (3)
- Soap Making Guide With Recipes: DIY Homemade Soapmaking Made Easy: DIY Homemade Soapmaking Made EasyFrom EverandSoap Making Guide With Recipes: DIY Homemade Soapmaking Made Easy: DIY Homemade Soapmaking Made EasyRating: 4.5 out of 5 stars4.5/5 (17)
- Women's Work: The First 20,000 Years: Women, Cloth, and Society in Early TimesFrom EverandWomen's Work: The First 20,000 Years: Women, Cloth, and Society in Early TimesRating: 4.5 out of 5 stars4.5/5 (190)
- Fabric Manipulation: 150 Creative Sewing TechniquesFrom EverandFabric Manipulation: 150 Creative Sewing TechniquesRating: 4.5 out of 5 stars4.5/5 (13)
- Famous Frocks: The Little Black Dress: Patterns for 20 Garment Inspired by Fashion IconsFrom EverandFamous Frocks: The Little Black Dress: Patterns for 20 Garment Inspired by Fashion IconsRating: 4 out of 5 stars4/5 (4)
- Knitting for Anarchists: The What, Why and How of KnittingFrom EverandKnitting for Anarchists: The What, Why and How of KnittingRating: 4 out of 5 stars4/5 (51)
- Crystal Basics: The Energetic, Healing, and Spiritual Power of 200 GemstonesFrom EverandCrystal Basics: The Energetic, Healing, and Spiritual Power of 200 GemstonesRating: 5 out of 5 stars5/5 (3)
- Glossy: Ambition, Beauty, and the Inside Story of Emily Weiss's GlossierFrom EverandGlossy: Ambition, Beauty, and the Inside Story of Emily Weiss's GlossierRating: 3.5 out of 5 stars3.5/5 (44)
- Strip Tees: A Memoir of Millennial Los AngelesFrom EverandStrip Tees: A Memoir of Millennial Los AngelesRating: 4 out of 5 stars4/5 (24)
- 250 Japanese Knitting Stitches: The Original Pattern Bible by Hitomi ShidaFrom Everand250 Japanese Knitting Stitches: The Original Pattern Bible by Hitomi ShidaRating: 5 out of 5 stars5/5 (7)
- The Skinny Confidential's Get the F*ck Out of the Sun: Routines, Products, Tips, and Insider Secrets from 100+ of the World's Best Skincare GurusFrom EverandThe Skinny Confidential's Get the F*ck Out of the Sun: Routines, Products, Tips, and Insider Secrets from 100+ of the World's Best Skincare GurusRating: 5 out of 5 stars5/5 (4)
- DIY Updos, Knots, & Twists: Easy, Step-by-Step Styling Instructions for 35 Hairstyles—from Inverted Fishtails to Polished Ponytails!From EverandDIY Updos, Knots, & Twists: Easy, Step-by-Step Styling Instructions for 35 Hairstyles—from Inverted Fishtails to Polished Ponytails!Rating: 3.5 out of 5 stars3.5/5 (7)
- Freehand Fashion: Learn to sew the perfect wardrobe – no patterns required!From EverandFreehand Fashion: Learn to sew the perfect wardrobe – no patterns required!Rating: 5 out of 5 stars5/5 (3)
- The Big Book Of Essential Oil Recipes For Beauty: Over 200 Homemade Aromatherapy Essential Oil Recipes For All-Round Natural Body CareFrom EverandThe Big Book Of Essential Oil Recipes For Beauty: Over 200 Homemade Aromatherapy Essential Oil Recipes For All-Round Natural Body CareRating: 5 out of 5 stars5/5 (4)
- 55 Fantastic Japanese Knitting Stitches: (Includes 25 Projects)From Everand55 Fantastic Japanese Knitting Stitches: (Includes 25 Projects)Rating: 3 out of 5 stars3/5 (2)