Professional Documents
Culture Documents
Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDF
Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDF
Uploaded by
Julio Cesar Guillen MoralesOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDF
Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDF
Uploaded by
Julio Cesar Guillen MoralesCopyright:
Available Formats
Review Article
Pelvic Fractures: Part 2.
Contemporary Indications and
Techniques for Definitive Surgical
Management
Abstract
Joshua R. Langford, MD Once the patient with pelvic fracture is resuscitated and stabilized,
Andrew R. Burgess, MD definitive surgical management and anatomic restoration of the
pelvic ring become the goal. Understanding injury pattern by stress
Frank A. Liporace, MD
examination with the patient under anesthesia helps elucidate the
George J. Haidukewych, MD instability. Early fixation of the unstable pelvis is important for
mobilization, pain control, and prevention of chronic instability or
deformity. Current pelvic fracture management employs a
substantial amount of percutaneous reduction and fixation, with
less emphasis placed on pelvic reconstruction proceeding from
posterior to anterior, and most reduction and fixation of unstable
pelvic fractures done with the patient supine. Compared with
control subjects with acetabular fracture or pelvic fracture alone,
patients with combined injury have a significantly higher Injury
Severity Score, lower systolic blood pressure, and higher mortality
rates; they are also transfused more packed red blood cells. Even
with anatomic restoration of the pelvis, long-term outcomes after
severe pelvic trauma are below population norms. The most
common chronic problems relate to sexual dysfunction and pain.
Regardless of fracture type, neurologic injury is a universal
harbinger of poor outcome.
S urgical decision making with pel-
vic injuries is a complex process.
After temporizing measures (eg, pel-
sion (APC) type I injuries (see part 1
of this series), in which the symphy-
sis is widened <2.5 cm and there is
vic binders) have been addressed and no widening of the sacroiliac (SI)
the patient resuscitated, definitive joint; however, confirmation is some-
fixation is undertaken. Specific surgi- times needed to rule out an occult
cal indications for pelvic injuries are APC type II injury.1,2 If there is any
as varied as the injuries themselves. doubt of the stability of the injury,
From the Orlando Regional Medical
Center, Orlando, FL. an examination under anesthesia will
help delineate the entirety of the in-
J Am Acad Orthop Surg 2013;21: Indications
458-468 jury.2,3 For patients presenting to the
outpatient clinic with a notable
http://dx.doi.org/10.5435/ Anteroposterior
JAAOS-21-08-458 amount of pain after an APC type I
Compression Injuries injury, a single-leg stance view can
Copyright 2013 by the American
Academy of Orthopaedic Surgeons.
Nonsurgical management is pre- provide the dynamic stress needed to
ferred for anteroposterior compres- rule out rotational instability.4
458 Journal of the American Academy of Orthopaedic Surgeons
Joshua R. Langford, MD, et al
Figure 1 an iliosacral screw is preferable.
For APC type III injuries, anterior
and posterior fixation is required be-
cause of the complete instability of
the hemipelvis. Often, these patients
are managed with temporizing mea-
sures (ie, antishock sheet/binder, ex-
ternal fixation) during resuscitation
and then later are converted to defin-
itive fixation with an anterior plate
and iliosacral fixation. This conver-
sion is usually performed during the
first week.
Lateral Compression
Injuries
A, Pre-stress AP pelvic radiograph. B, AP radiograph with internal rotation
stress being applied to the pelvis (arrows), demonstrating complete collapse The lateral compression (LC) injury
of the right hemipelvis (superior ramus almost across the midline). is also graded from I to III. One of
the most common pelvic injuries is
the LC type I, which is an injury to
For APC type II injuries, surgical fixation is a point of debate. To as- the superior and inferior pubic rami
stabilization is generally indicated.5 sist in decision making, a recent as well as impaction to the sacrum.
The literature on indications for this study introduces a modification to The great majority of patients are
injury is scant at best, largely consist- the Young-Burgess classification and treated nonsurgically with weight
ing of studies without control attempts to subclassify APC injuries bearing to tolerance on the affected
groups. No study (prospective or ret- based on the amount of sagittal side and have a low risk of displace-
rospective) in the literature compares plane rotation.3 In an APC type IIa ment.9 Considerable controversy sur-
APC type II injuries managed surgi- injury, the posterior SI ligaments are rounds the optimal management of
cally versus nonsurgically. Despite intact and anterior fixation alone this injury mostly because of the ex-
the lack of papers on indications, the will likely be sufficient for manage- treme variability in fracture stability.
long-term outcomes following fixa- ment. In an APC type IIb injury, the For a given static displacement on
tion of these unstable injuries often posterior SI ligaments are attenuated, an AP radiograph, great variability
leads to excellent results.6,7 In con- which may contribute to more sagit- on dynamic stress views can be
trast, the sequelae of a missed unsta- tal plane rotational instability of the noted. For an LC type I injury, no
ble pelvic injury can be devastating hemipelvis. On dynamic stress views, consensus exists regarding how
to the patient. The surgical options this sagittal plane instability mani- much dynamic instability can be tol-
for management of chronic instabil- fests with vertical changes at the erated. In general, if a patient has
ity and pain related to a missed in- pubis and should be considered un- too much pain to move out of bed,
jury are complex and associated with stable if there is >1 cm of displace- then performing an examination un-
more unpredictable outcomes when ment.3 If this instability is present, der anesthesia may be warranted
treated in a delayed setting.8 supplementing the anterior fixation (Figure 1).
Determining the need for posterior with posterior ring stabilization via In addition to compression testing,
Dr. Langford or an immediate family member serves as a paid consultant to Stryker and has stock or stock options held in the
Institute for Better Bone Health, LLC. Dr. Burgess or an immediate family member is a member of a speakers’ bureau or has made
paid presentations on behalf of, and has stock or stock options held in, Stryker. Dr. Liporace or an immediate family member has
received royalties from Biomet; is a member of a speakers’ bureau or has made paid presentations on behalf of Biomet, Synthes,
Stryker, and Medtronic; serves as a paid consultant to Biomet, Medtronic, Synthes, and Stryker; and serves as an unpaid consultant
to AO. Dr. Haidukewych or an immediate family member has received royalties from DePuy and Biomet; serves as a paid consultant
to Smith & Nephew, Synthes, and DePuy; has stock or stock options held in Orthopediatrics and the Institute for Better Bone Health;
has received nonincome support (such as equipment or services), commercially derived honoraria, or other non–research-related
funding (such as paid travel) from Synthes; and serves as a board member, owner, officer, or committee member of the American
Academy of Orthopaedic Surgeons.
August 2013, Vol 21, No 8 459
Pelvic Fractures: Part 2. Contemporary Indications and Techniques for Definitive Surgical Management
performing a push-pull test of the complete vertical sacral injury. Occa- Alternatively, a Farabeuf or Jung-
hemipelvis will help demonstrate sionally the injury may occur bluth clamp (Figure 2) may be used
sagittal plane instability. Much like through the posterior ilium, leaving a to hold the reduction. For anterior
an APC injury, the posterior LC in- crescent attached to the sacrum, ring patterns that involve ramus frac-
jury may be more complex than a which initially resembles the LC type tures as well as symphysis involve-
pure coronal plane internal rotation II injury. Surgical fixation is indi- ment, the surgeon can extend the ex-
injury. Sagittal plane deformity cated in all VS injuries. posure up the pelvic brim to gain
(flexion/extension of the hemipelvis) fixation above the acetabulum
may occur though an unstable sacral Combined Injuries through the midline incision. Famil-
injury. Therefore, if there is evidence Although uncommon, unstable pel- iarization with the anterior intrapel-
vic injuries may be associated with vic (modified Rives-Stoppa) ap-
of sagittal plane instability (ie, >1 cm
displaced acetabular fractures. Le- proach is necessary to safely perform
of displacement), then posterior fixa-
tournel et al12 reported that unstable this fixation.15
tion, in addition to anterior fixation,
SI injury or symphysis disruption re- Another method of anterior fixa-
will help avoid further displacement.
quiring fixation was present in 6.7% tion is with percutaneous anterior
Although rare, a unique LC injury
of patients with displaced acetabular plating.16 Three incisions are created,
that requires intervention is the so-
fractures in their study. In a more re- one placed over each anterior supe-
called locked symphysis. During se- rior iliac spine (exposing the iliac
cent series, 5.1% of patients had the
vere lateral compression, the sym- crest) and then a central Pfan-
so-called devastating dyad of com-
physis can tear, and the intact pubic nenstiel-type incision, which is used
bined unstable pelvic injury and dis-
body may cross over the uninjured to visualize the anterior pelvis. The
placed acetabular fractures.13 Com-
side and get locked into the obtura- pubis is not exposed in this approach
pared to control subjects with
tor ring. Occasionally, grasping the because the plate is completely extra-
acetabular fracture or pelvic fracture
iliac crests and using the figure-of-4 fascial. A plate is then tunneled
alone, patients with a combined in-
position of the legs reduces this dis- across the front of the pelvis anterior
jury have a statistically significantly
location by closed means. If reduc- to the neurovascular structures and
higher Injury Severity Score, lower
tion is possible and if the pelvis is is connected to each hemipelvis as
systolic blood pressure, and higher
stable, no further treatment is neces- well as in the midline to the pubic
mortality rates, and they are trans-
sary. If closed reduction fails, then body. This type of fixation is useful
fused more packed red blood
open treatment is required. Often, for a multifocal anterior ring injury
cells.13,14 Combined injuries are al-
there is an associated bladder or ure- (ie, bilateral ramus fractures with
most universally indicated for fixa-
thral injury.10,11 symphyseal disruption).
tion because of their inherent insta-
Another LC variant is the “tilt” In addition to plating techniques,
bility.
fracture, in which the superior ramus fixation with a subcutaneous fixator
rotates through the symphysis and is was recently described and may be
pushed posteriorly and inferiorly Fixation of the Anterior useful in both gaining a better me-
into the perineum. In female pa- Ring chanical advantage and minimizing
tients, this injury may lead to dys- pin tract infection associated with
pareunia (pain with intercourse). To Internal Fixation external fixation.17 In this technique,
help avoid later dyspareunia, surgi- The surgical approach for anterior pedicle screws (6 to 8 mm diameter)
cal management is often undertaken fixation is through a Pfannenstiel- are placed from the anteroinferior il-
to reduce the fracture. type incision. In the deep dissection, iac spine in the interosseous path to-
a vertical split in the linea alba will ward the posteroinferior iliac spine.
Vertical Shear Injuries help preserve any remaining inser- The method for inserting these pedi-
A vertical shear (VS) injury is one tion of the rectus abdominus muscle cle screws follows most of the same
that involves a complete injury to the that was not affected by the initial steps as those for insertion of pins
ligamentous structures on one side of trauma. Exposure of the pubis to the for a low anterior external fixator
the pelvis, typically resulting in ceph- pubic tubercle is usually adequate for (see below). A bar is then passed
alad displacement of the hemipelvis. symphysis disruptions. A pointed subcutaneously across the front of
The injury usually involves the ra- clamp with its points on each pubic the pelvis (above the fascia), and the
mus or pubic symphysis, in addition tubercle is used for final manipula- screws are connected to maintain re-
to either a complete SI dislocation or tion of the reduction before plating. duction (Figure 3). Special attention
460 Journal of the American Academy of Orthopaedic Surgeons
Joshua R. Langford, MD, et al
Figure 2
A, Photograph of a Farabeuf clamp. Its jaws are good for grasping the pelvic wing, while the nose can grasp screw
heads to perform reductions. B, Screws are temporarily inserted into the bone and left proud so that the Farabeuf can
clamp onto the screw heads. A reduction can then be fine-tuned and compressed. C, Photograph of a Jungbluth
clamp. Temporary screws are also used for this clamp. Unlike a Farabeuf, the Jungbluth can also be used to distract a
fracture because the clamp circles the entire screw head.
must be directed to keeping the pedi- tained (Figure 4). Using a metal in-
Figure 3
cle screw heads above the fascia and strument and fluoroscopy will help
not pushing the rod down to meet identify an adequate starting point in
the screw heads as this may cause the supra-acetabular bone. The ana-
compression and subsequent injury tomic structures at greatest risk dur-
to the neurovascular bundles. ing this procedure are the hip capsule
and the lateral femoral cutaneous
External Fixation nerve. The hip capsule reflection
Alternatively, the anterior injury may ends, on average, 16 mm above the
be stabilized with external fixation. joint but may be as high as 20 mm.20
The pins start at the anterior inferior The mean distance from the pin in-
iliac spine and are directed toward sertion site to the lateral femoral cu-
the posterior ilium just superior to taneous nerve is 10 mm but can be
AP pelvic radiograph demonstrating
the greater sciatic notch. The use of as close as 2 mm.20 Once the trochar
an internal fixator for the
hydroxyapatite pins provides im- is on the pelvis, an iliac oblique inlet management of multiple ramus
proved long-term fixation for frames view will demonstrate that the pin is fractures.
that are used for definitive care.18,19 proximal to the hip joint and di-
The technique for insertion of an- rected toward the sciatic buttress, between the inner and outer tables of
terior pelvic pins uses special radio- proximal to the greater sciatic fora- the pelvis (Figure 6). This view will
graphic views. To identify the corri- men (Figure 5). Next, the obturator help prevent early exit of the pin and
dor of bone in the pelvis, an oblique inlet view is obtained to can allow passage to the most poste-
obturator oblique outlet view is ob- demonstrate the interosseous path rior aspect of the ilium.
August 2013, Vol 21, No 8 461
Pelvic Fractures: Part 2. Contemporary Indications and Techniques for Definitive Surgical Management
Figure 4 Figure 5 Figure 6
An obturator oblique outlet Iliac oblique inlet radiograph
radiograph is used to identify the demonstrating the starting point Obturator oblique inlet radiograph
starting position to insert anterior out of the hip capsule and the demonstrating the interosseous
pelvic pins. pin trajectory above the sciatic path to the posterior ileum.
notch.
SI joint. This proximity of the L5
Fixation of the Posterior For standard SI dislocations, the wire nerve root usually allows only one
Ring is inserted to the midpoint of the sa- hole of a plate to cross onto the sa-
cral body or just beyond. cral ala. Therefore, if SI plating is to
Percutaneous Iliosacral be used, two plates are necessary to
Screws Open Reduction of the gain control of the injured SI joint.23
Sacroiliac Joint An alternative technique is to use an-
Percutaneous iliosacral insertion that
Reduction may be achieved from ei- terior SI plates in addition to ilio-
relies on radiographic landmarks has
ther a posterior or an anterior ap- sacral screws, which has been shown
been described and is highly repro-
proach. For a posterior approach, to be one of the most stable con-
ducible.21,22 It is important to identify
the patient is placed in the prone po- structs.23
and line up the iliac cortical densi-
sition and the SI joint is exposed. Be-
ties, which parallel the sacral ala and cause the most posterior aspect of
represent the anterior margin of the the ilium is dorsal and medial to the Techniques for Specific
safe zone for iliosacral screw inser- SI joint, direct visualization of the fi- Injury Patterns
tion. Respecting the anterior margin nal reduction is not possible. After
protects the L5 nerve root and the il- reduction, a percutaneous iliosacral Anteroposterior
iac vessels. The posterior safe zone screw is placed. Alternatively, poste- Compression Injuries
on the lateral side is the identifica- rior tension band plating or iliac bars External fixation still has a place in
tion of the upper sacral nerve root may be employed for fixation. These the treatment of APC injury. Often,
tunnel. The trajectory of the guide- devices are used in special circum- external fixation is a temporizing
wire insertion depends on the desired stances (ie, severe sacral dysmor- measure taken before conversion to
compressive vector. For SI disloca- phism) in which safe iliosacral screw definitive internal fixation. The half
tions, a more posterior-to-anterior passage may not be possible. pins are not reduction devices in an
vector is desired, whereas for sacral An anterior approach using the lat- APC injury. For a low anterior
fractures, a more transverse trajec- eral window of the ilioinguinal ap- frame, the pins are inserted to the
tory is desired. proach may be used. This allows a appropriate depth, and then two as-
The depth of wire insertion de- direct view of the cephalad joint. sistants push on the greater trochan-
pends on the requirements of the Fixation can be accomplished with ters (providing a reduction force
screw. For comminuted sacral frac- SI plating, percutaneous iliosacral from posterolateral to the midline),
tures, the wire may be inserted screws, or a combination of the two. followed by final tightening of the
across the sacral body to the contra- The danger in this approach is the external fixator components. If iliac
lateral SI joint (transsacral screw). proximity of the L5 nerve root to the wing pins are chosen, two or three
462 Journal of the American Academy of Orthopaedic Surgeons
Joshua R. Langford, MD, et al
pins per side should be used in an at- Figure 7
tempt to ensure that at least one pin
has adequate purchase between the
inner and outer tables of the ilium.
Our current indications for definitive
external fixation with APC type inju-
ries are for unstable pelvic injuries in
the face of extraperitoneal bladder
rupture as well as for management of
the anterior injury in open pelvic
fractures with contamination. This is
often combined with percutaneous
posterior iliosacral fixation.
When open treatment is under-
taken, fixation is most often non-
locked plating of the pubic symphy-
sis. Only one clinical study compares
different internal fixation constructs Clinical photograph demonstrating the binder positioned farther down the
thighs to maintain reduction in a patient with pelvic fracture.
for anterior pubis plating. Compared
to a multi-hole construct, a two-hole
plate has a higher rate of malunion Figure 8
and device failure.24 Currently, the
role of locked plating across the pu-
bis is controversial and not thought
to be beneficial.25,26 Therefore, the
choice of anterior fixation is often a
multi-hole plate with at least two
points of nonlocked fixation on ei-
ther side of the symphysis. For an
APC type IIb injury, the preferred
management is to supplement this
anterior fixation with posterior ring
stabilization via an iliosacral screw.
The classic teaching for an APC
type III injury is to begin reconstruc- A, Outlet radiograph of iliosacral guidewires in place with the sacroiliac (SI)
joint still wide before placement of partially threaded screws. B, Outlet
tion and stabilization at the SI joint radiograph demonstrating that the iliosacral screws have “closed down” the
and progress anteriorly. With newer gap.
methods of percutaneous reduction,
open reduction of the dislocation is
not always needed. Multiple authors mizing these closed reduction ma- ure 9). Alternatively, the anterior
have reported favorable outcomes neuvers facilitates the procedure. It is ring may be temporarily clamped,
with a “front first” approach to then possible to perform anterior fix- followed by percutaneous iliosacral
management of these injuries.7,27 A ation with symphysis plating and screw placement, and then definitive
CT scan with the patient in the then proceed to percutaneous ilio- anterior plating.
binder often reveals a closed anterior sacral fixation using a partially For SI dislocations that are com-
ring with a gapped, but aligned, SI threaded screw with a washer to pletely displaced even in a binder, di-
joint. In this case, the binder may be “close down” the dislocation (Figure rect reduction must be performed.
left in place to assist in maintaining 8). If there is mild rotational defor- This is achieved by either an open re-
the reduction during anterior stabili- mity of the hemipelvis in the binder, duction or a percutaneously guided
zation (Figure 7). In addition, then performing anterior fixation reduction. For percutaneous reduc-
internal-rotation taping of the feet first may assist in achieving control tion, one may use a frame attached
will further assist reduction.28 Maxi- of a posterior rotational injury (Fig- to the bed and/or external fixation
August 2013, Vol 21, No 8 463
Pelvic Fractures: Part 2. Contemporary Indications and Techniques for Definitive Surgical Management
Figure 9 Figure 10
AP radiograph of anteroposterior
compression type IIb injury after A, Three-dimensional CT reconstruction image of a lateral compression type
binder placement, demonstrating II injury with iliac piece large enough for fixation. B, AP pelvic radiograph of
sagittal plane rotational instability in fixation extending across to the uninjured hemipelvis to help anchor the
addition to coronal instability. fixation and resist displacement.
pins to provide enough force to com- useful in resisting the instability asso- ued instability (Figure 10). This pat-
plete and hold the reduction.29 This ciated with this injury.33 This tech- tern is often amenable to an “LC
method can achieve excellent reduc- nique uses a traditional crest gluteus type II” screw, that is, one that uses
tions even in severely displaced dis- medius pillar pin (from iliac crest be- the same corridor as low anterior
locations.30,31 When percutaneous tween the inner and outer table) on half pins from the anterior inferior il-
methods of reduction are unsuccess- the unaffected hemipelvis and a low iac spine back to the posterior ilium.
ful, open reduction is needed. anterior pin on the affected side. For This intramedullary fixation across
Our preference for open reduction an LC type I injury with concomitant the iliac fracture often yields a very
is the anterior approach. The ratio- sagittal plane instability (ie, >1 cm of stable construct.
nale for this preference also has to displacement on push/pull), an ilio- Much like standard LC type II in-
do with convenience and safety. By sacral screw is added to stabilize the juries, the method of fixation for
keeping the patient in a supine posi- posterior injury. crescent fractures is dependent on
tion, the entire injury may be man- An LC type II injury is a posterior the remaining size of ilium attached
aged with one draping while still giv- fracture either through the entire il- to the sacrum. For fractures with
ing anesthesia full access to the ium or through the ilium and tra- large portions of ilium still attached,
patient. When using the anterior ap- versing a portion of the inferior SI the lateral window of an ilioinguinal
proach, careful evaluation of the en- joint (ie, crescent fracture) with asso- approach may be used. For inter-
tire SI joint must be done to ensure ciated ipsilateral rami fractures. In a mediate-sized pieces, a prone ap-
that overcompression of the superior crescent fracture, the fracture goes proach with fixation along the iliac
aspect of the joint has not occurred, through the iliac wing and into the SI wing will permit stable fixation.34
thereby resulting in an abduction de- joint, yielding a rotationally unstable When the crescent leaves only a
formity of the hemipelvis. hemipelvis but with maintained sta- small piece of ilium, the injury may
bility to vertical forces.34 be managed with an iliosacral
Lateral Compression If open reduction is needed, the ap- screw.35,36 As with SI dislocations in
Injuries proach is dependent on the size and an APC injury, a low anterior half
For an LC type I fracture, if the rami position of the iliac fragment. For an pin may be used as a percutaneous
on the affected side cross the midline iliac wing injury that does not in- reduction aid (Figure 11).
with compressive stress, then inter- volve the SI joint, a posterior ap- LC type III injuries generally result
vention with an anterior two-pin fix- proach usually provides the best ac- from severe crush-type mechanisms
ator held in distraction or an in- cess for fixation. At times, even after and are often referred to as a “wind-
tramedullary superior ramus screw fixation of the posterior pelvis, an- swept pelvis.” Surgical treatment of
will reliably control the instability.32 choring the construct to the opposite LC type III injuries follows the same
Recent reports have indicated that an hemipelvis is needed to prevent post- methods as those for LC and APC
oblique plane distraction may also be operative displacement from contin- injuries, but in combination. Often,
464 Journal of the American Academy of Orthopaedic Surgeons
Joshua R. Langford, MD, et al
the externally rotated hemipelvis will Figure 11
need iliosacral fixation with a percu-
taneous screw. The anterior injury is
varied, and management is according
to the injury. Ramus fractures and
pubis dislocations may both be man-
aged with anterior plating or with
external fixation. Often the compres-
sion side has a stable sacral injury
that may need no surgical interven-
tion. However, if there is an unstable
posterior injury on the compression
side, then our preference is to fix the
posterior injury to build a stable
platform for reconstruction of the A, Three-dimensional CT reconstruction demonstrating that a half pin may be
contralateral externally rotated used to reduce this lateral compression type III crescent fracture (arrow).
B, Three-dimensional CT reconstruction of the same patient after percutane-
hemipelvis. Also, if one hemipelvis
ous reduction, iliosacral screw placement, and anterior external fixation.
exhibits excessive internal rotation
with a significant sacral crush, then
it may need to be externally rotated
tion and fixation of the posterior pel- possibility for transsacral fixation is
and held with a fully threaded SI
vic injury with iliosacral screws is a locked construct in which the
screw to allow for reduction and sta-
performed. Every effort is made for screw is threaded with a nut on the
bilization of the traumatically exter-
an anatomic reduction because this is contralateral ilium. Early biome-
nally rotated hemipelvis.
a predictor of better outcome for chanical and clinical experience has
these injuries.27 To assist in the neu- been encouraging at controlling ver-
Locked Symphysis
tralization of displacement forces, tical sacral fractures with this con-
To aid in reduction of this disloca- anterior fixation should be per- struct.38,39
tion, a universal distractor may be formed. More than one iliosacral In addition to transsacral fixation,
employed with one pin in each screw for these severe injuries may there have been many other attempts
hemipelvis. If this fails, an open ap- be useful. This may be accomplished to solve the problem of vertical dis-
proach for direct manual reduction is with either two screws in the S1 placement in transforaminal sacral
used.10 If open reduction fails, an os- body, or one screw in the S1 body fractures, including iliac bars, trans-
teotomy of the superior ramus on the and one screw in the S2 body. sacral plating, and spinopelvic fixa-
uninjured side will release the ten- VS injuries with transforaminal sa- tion. “Connecting” the spine to the
sion and allow for reduction.11 If no cral injury are difficult to manage pelvis with instrumentation that en-
bladder injury is present and instabil- with traditional iliosacral screw tech- gages both structures is referred to as
ity persists after reduction, anterior niques.37 Iliosacral screws depend on spinopelvic fixation; the addition of
plating is performed. For instability purchase on the dense cortical bone an iliosacral screw to this construct
with concomitant bladder injury, a of the SI joint. In a vertical sacral is referred to as triangular osteosyn-
two-pin anterior fixator is used. Oc- fracture, purchase is limited to a thesis40 (Figure 12). These constructs
casionally, the pelvis will be stable to short segment of cancellous bone have demonstrated biomechanical
stress after open reduction. In that from the fracture to the sacral body. superiority to traditional iliosacral
situation, no further internal fixation To help mitigate this, some have ad- screws.41,42 In one study, triangular
is necessary. vocated for transsacral fixation. osteosynthesis was able to hold a re-
These screws can be a combination duction to healing in 95% of pa-
Vertical Shear of fully threaded and partially tients but was associated with a high
Surgical management of VS injuries threaded screws, depending on their complication rate, including wound
can be very challenging because of desired effect. While overcompres- problems, nerve injury, scoliosis, and
the extreme forces that require neu- sion of a sacral nerve root is a theo- delayed union.43 Longer-term out-
tralization. If the vertical component retic possibility, no literature exists come studies of this technique are
is a pure SI dislocation, then reduc- to support this concern. Another currently lacking and will be impor-
August 2013, Vol 21, No 8 465
Pelvic Fractures: Part 2. Contemporary Indications and Techniques for Definitive Surgical Management
Figure 12 the symphysis, and final symphysis
alignment >5 mm from anatomic are
all associated with dyspareunia.44 In
addition, all of the patients with as-
sociated bladder rupture reported
dyspareunia.44 In another study,
women with symphyseal disruption
were at increased risk for sexual and
excretory dysfunction, independent
of overt pelvic organ injury, at 1 year
after trauma.45 With regard to child-
birth, normal vaginal delivery is pos-
sible; however, the rate of cesarean
A, Axial CT scan demonstrating comminuted transforaminal sacral injury. section is higher than in the standard
B, AP pelvic radiograph after spinopelvic fixation (triangular osteosynthesis
on the right). population (largely because of pa-
tient and obstetrician preference).46
Men are also prone to sexual dys-
tant to determining its place in the day after surgery, in addition to me- function, with 61% of patients re-
management of this fracture. In our chanical prophylaxis with sequential porting limitation in sexual function
practice, spinopelvic fixation is used compression devices and stockings.
and 19% continuing on to persistent
for comminuted transforaminal sa- After an unstable injury to the
erectile dysfunction.47 Specifically,
cral fractures from a VS mechanism hemipelvis (ie, APC type III), full
APC-type injuries and increasing age
that cannot be controlled with trans- weight bearing on the affected side
in men appear to be significant risk
sacral fixation. should not commence until at least 8
factors for erectile dysfunction, with
weeks, with many surgeons waiting
some studies reporting rates as high
Combined Injuries until 12 weeks.23 For an injury that
has only rotational instability (ie, LC as 90%.48 However, fixation of an
Surgical management of these inju-
type I), immediate weight bearing af- unstable pelvis does not change the
ries is complex, and consensus is lim-
ter stabilization with a low anterior results of impotence or neurologic
ited on the order of reconstruction.
two-pin external fixator is possible.32 injury incurred at the time of the
In general, it is important to recon-
For a bilaterally unstable pelvic in- trauma.
struct a stable posterior base from
jury, mobilization of bed to chair for Compared to a reference popula-
which to build. With an anatomi-
at least 8 weeks is necessary. Again, tion 2 years after surgically treated
cally reduced posterior ring, recon-
one must individualize to the injury pelvic injuries, patients reported sub-
struction of the acetabular columns
pattern and quality of fixation and stantially lower quality of life in both
may be easier. The most important
take into account other injuries that physical and mental domains, even
aspect of the reconstruction is an an-
may affect weight bearing (ie, ipsilat- when radiologic and clinical out-
atomic reduction of the acetabulum.
eral pilon fracture). It is intuitive to comes were considered favorable.49
We generally prefer to anatomically
protect fixation of a joint with a liga- Prevalence of chronic posttraumatic
reduce and stabilize the posterior
mentous injury for a period of time pelvic pain after AO class A, B, and
pelvic injury, then proceed anteriorly
to allow for soft-tissue healing, but C fractures is 38%, 67%, and 90%,
to the acetabulum, and finally to the
the exact time necessary to achieve a respectively.50 Regardless of fracture
anterior pelvic ring injury.
critical level of healing is unclear. type or location, neurologic injury
appears to be a universally accepted
Postoperative harbinger of poor outcome.51 All pa-
Management Long-term Sequelae tients should be counseled about
these sequelae so that reversible defi-
Postoperative protocols are as varied Long-term deficits after pelvic frac- cits may be managed appropriately
as the injuries themselves. Our pref- ture are common. Fifty-six percent of to help maximize outcome. It is im-
erence is to initiate chemoprophy- women report dyspareunia after pel- portant to counsel patients that pel-
laxis for prevention of venous vic fracture.44 Initial symphysis dis- vic pain is common and expected af-
thrombolic embolism beginning the ruption, need for plate fixation of ter almost all severe pelvic fractures.
466 Journal of the American Academy of Orthopaedic Surgeons
Joshua R. Langford, MD, et al
studies. References 10, 11, and 40 are 13. Suzuki T, Smith WR, Hak DJ, et al:
Summary level V expert opinion.
Combined injuries of the pelvis and
acetabulum: Nature of a devastating
References printed in bold type are dyad. J Orthop Trauma 2010;24(5):303-
Most reduction and fixation of un-
308.
stable pelvic fractures is performed those published within the past 5
14. Osgood GM, Manson TT, O’Toole RV,
with the patient in the supine posi- years.
Turen CH: Combined pelvic ring
tion. Nonsurgical management is 1. Gardner MJ, Krieg JC, Simpson TS, disruption and acetabular fracture:
Associated injury patterns in 40 patients.
preferred for APC type I injuries. In Bottlang M: Displacement after
simulated pelvic ring injuries: A J Orthop Trauma 2013;27(5):243-247.
an APC type IIa injury, the posterior cadaveric model of recoil. J Trauma 15. Sagi HC, Afsari A, Dziadosz D: The
SI ligaments are intact, and anterior 2010;68(1):159-165. anterior intra-pelvic (modified rives-
fixation alone is typically sufficient. 2. Suzuki T, Morgan SJ, Smith WR, Stahel stoppa) approach for fixation of
In an APC type IIb injury, the poste- PF, Flierl MA, Hak DJ: Stress radiograph acetabular fractures. J Orthop Trauma
to detect true extent of symphyseal 2010;24(5):263-270.
rior SI ligaments are attenuated,
disruption in presumed anteroposterior 16. Cole PA, Gauger EM, Anavian J, Ly TV,
which may contribute to more sagit- compression type I pelvic injuries. Morgan RA, Heddings AA: Anterior
tal plane rotational instability of the J Trauma 2010;69(4):880-885. pelvic external fixator versus
subcutaneous internal fixator in the
hemipelvis. With >1 cm of displace- 3. Sagi HC, Coniglione FM, Stanford JH:
treatment of anterior ring pelvic
Examination under anesthetic for occult
ment, supplementing the anterior fix- pelvic ring instability. J Orthop Trauma fractures. J Orthop Trauma 2012;26(5):
269-277.
ation with posterior ring stabiliza- 2011;25(9):529-536.
tion via an iliosacral screw is 4. Siegel J, Templeman DC, Tornetta P III: 17. Vaidya R, Colen R, Vigdorchik J,
Single-leg-stance radiographs in the Tonnos F, Sethi A: Treatment of unstable
preferable. For APC type III injuries, pelvic ring injuries with an internal
diagnosis of pelvic instability. J Bone
anterior and posterior fixation is re- Joint Surg Am 2008;90(10):2119-2125. anterior fixator and posterior fixation:
Initial clinical series. J Orthop Trauma
quired as well as temporizing mea- 5. Matta JM: Indications for anterior 2012;26(1):1-8.
sures during resuscitation. Most pa- fixation of pelvic fractures. Clin Orthop
Relat Res 1996;329:88-96. 18. Placzek R, Ruffer M, Deuretzbacher G,
tients with LC type I injury are Heijens E, Meiss AL: The fixation
treated nonsurgically. If open reduc- 6. Tornetta P III, Dickson K, Matta JM: strength of hydroxyapatite-coated
Outcome of rotationally unstable pelvic Schanz screws and standard stainless
tion is needed for an LC type II in- ring injuries treated operatively. Clin steel Schanz screws in lower extremity
jury, the approach is governed by the Orthop Relat Res 1996;329:147-151. lengthening: A comparison based on a
new torque value index. The fixation
size and position of the iliac frag- 7. Van Loon P, Kuhn S, Hofmann A, index. Arch Orthop Trauma Surg 2006;
ment. Surgical treatment of LC type Hessmann MH, Rommens PM: 126(6):369-373.
Radiological analysis, operative
III injuries follows the same methods management and functional outcome of 19. Moroni A, Cadossi M, Romagnoli M,
as those for LC and APC injuries. open book pelvic lesions: A 13-year Faldini C, Giannini S: A biomechanical
cohort study. Injury 2011;42(10):1012- and histological analysis of standard
Surgical fixation is indicated in all 1019. versus hydroxyapatite-coated pins for
VS injuries. Patients with unstable external fixation. J Biomed Mater Res B
8. Kanakaris NK, Angoules AG, Nikolaou Appl Biomater 2008;86(2):417-421.
pelvic injuries combined with dis- VS, Kontakis G, Giannoudis PV:
placed acetabular fractures are al- Treatment and outcomes of pelvic 20. Haidukewych GJ, Kumar S, Prpa B:
malunions and nonunions: A systematic Placement of half-pins for supra-
most always indicated for fixation review. Clin Orthop Relat Res 2009; acetabular external fixation: An
because of inherent instability. Long- 467(8):2112-2124. anatomic study. Clin Orthop Relat Res
2003;411:269-273.
term deficits after pelvic fracture are 9. Bruce B, Reilly M, Sims S: OTA
common; the most common chronic highlight paper predicting future 21. Carlson DA, Scheid DK, Maar DC, Baele
displacement of nonoperatively managed JR, Kaehr DM: Safe placement of S1 and
problems relate to sexual dysfunc- lateral compression sacral fractures: Can S2 iliosacral screws: The “vestibule”
tion and pain. it be done? J Orthop Trauma 2011; concept. J Orthop Trauma 2000;14(4):
25(9):523-527. 264-269.
10. Cannada LK, Reinert CM: Case report: 22. Routt ML Jr, Kregor PJ, Simonian PT,
References locked pubic symphysis: An open Mayo KA: Early results of percutaneous
reduction technique. Clin Orthop Relat iliosacral screws placed with the patient
Res 2009;467(8):2192-2195. in the supine position. J Orthop Trauma
Evidence-based Medicine: Levels of 1995;9(3):207-214.
11. O’Toole RV, Sagebien C, Andersen RC,
evidence are described in the table of Nascone JW: Superior pubic ramus 23. Tile M, Helfet DL, Kellam JF: Fractures
contents. In this article, references 3, osteotomy to treat locked pubic of the Pelvis and Acetabulum, ed 3.
symphysis: A case report. J Bone Joint Philadelphia, PA, Lippincott Williams &
18, 32, 45, and 46 are level II studies. Surg Am 2006;88(7):1609-1614. Wilkins, 2003.
References 4, 9, 13, 24, 37, 41, 47, 49,
12. Letournel E, Judet R, Elson R: Fractures 24. Sagi HC, Papp S: Comparative
and 50 are level III studies. References of the Acetabulum, ed 2. Berlin, radiographic and clinical outcome of
17, 22, 28, 33-36, and 43 are level IV Germany, Springer-Verlag, 1993. two-hole and multi-hole symphyseal
August 2013, Vol 21, No 8 467
Pelvic Fractures: Part 2. Contemporary Indications and Techniques for Definitive Surgical Management
plating. J Orthop Trauma 2008;22(6): 34. Borrelli J Jr, Koval KJ, Helfet DL: loads. J Orthop Trauma 2003;17(1):22-
373-378. Operative stabilization of fracture 31.
dislocations of the sacroiliac joint. Clin
25. Moed BR, Grimshaw CS, Segina DN: 43. Sagi HC, Militano U, Caron T, Lindvall
Orthop Relat Res 1996;329:141-146.
Failure of locked design-specific plate E: A comprehensive analysis with
fixation of the pubic symphysis: A report 35. Day AC, Kinmont C, Bircher MD, minimum 1-year follow-up of vertically
of six cases. J Orthop Trauma 2012; Kumar S: Crescent fracture-dislocation unstable transforaminal sacral fractures
26(7):e71-e75. of the sacroiliac joint: A functional treated with triangular osteosynthesis.
26. Grimshaw CS, Bledsoe JG, Moed BR: classification. J Bone Joint Surg Br 2007; J Orthop Trauma 2009;23(5):313-321.
Locked versus standard unlocked plating 89(5):651-658.
44. Vallier HA, Cureton BA, Schubeck D:
of the pubic symphysis: A cadaver
36. Osterhoff G, Ossendorf C, Wanner GA, Pelvic ring injury is associated with
biomechanical study. J Orthop Trauma
Simmen HP, Werner CM: Posterior sexual dysfunction in women. J Orthop
2012;26(7):402-406.
screw fixation in rotationally unstable Trauma 2012;26(5):308-313.
27. Mullis BH, Sagi HC: Minimum 1-year pelvic ring injuries. Injury 2011;42(10):
follow-up for patients with vertical shear 992-996. 45. Wright JL, Nathens AB, Rivara FP,
sacroiliac joint dislocations treated with MacKenzie EJ, Wessells H: Specific
iliosacral screws: Does joint ankylosis or 37. Griffin DR, Starr AJ, Reinert CM, Jones fracture configurations predict sexual
anatomic reduction contribute to AL, Whitlock S: Vertically unstable and excretory dysfunction in men and
functional outcome? J Orthop Trauma pelvic fractures fixed with percutaneous women 1 year after pelvic fracture.
2008;22(5):293-298. iliosacral screws: Does posterior injury J Urol 2006;176(4 pt 1):1540-1545.
pattern predict fixation failure? J Orthop
28. Gardner MJ, Parada S, Chip Routt ML Trauma 2003;17(6):399-405. 46. Vallier HA, Cureton BA, Schubeck D:
Jr: Internal rotation and taping of the Pregnancy outcomes after pelvic ring
lower extremities for closed pelvic 38. Tabaie SA, Bledsoe JG, Moed BR:
injury. J Orthop Trauma 2012;26(5):
reduction. J Orthop Trauma 2009;23(5): Biomechanical comparison of standard
302-307.
361-364. iliosacral screw fixation to transsacral
locked screw fixation in a Type C - Zone 47. Metze M, Tiemann AH, Josten C: Male
29. Matta JM, Yerasimides JG: Table- II pelvic fracture model. J Orthop sexual dysfunction after pelvic fracture.
skeletal fixation as an adjunct to pelvic Trauma 2012; Oct 30 [Epub ahead of J Trauma 2007;63(2):394-401.
ring reduction. J Orthop Trauma 2007; print].
21(9):647-656. 48. Collinge CA, Archdeacon MT, LeBus G:
39. Moed BR, Whiting DR: Locked
Saddle-horn injury of the pelvis: The
30. Ayvaz M, Cağlar O, Yılmaz G, transsacral screw fixation of bilateral
injury, its outcomes, and associated male
Güvendik GI, Acaroğlu RE: Long-term injuries of the posterior pelvic ring:
sexual dysfunction. J Bone Joint Surg
outcome and quality of life of patients Initial clinical series. J Orthop Trauma
with unstable pelvic fractures treated by 2010;24(10):616-621. Am 2009;91(7):1630-1636.
closed reduction and percutaneous 49. Borg T, Berg P, Fugl-Meyer K, Larsson
fixation. Ulus Travma Acil Cerrahi Derg 40. Sagi HC: Technical aspects and
recommended treatment algorithms in S: Health-related quality of life and life
2011;17(3):261-266.
triangular osteosynthesis and spinopelvic satisfaction in patients following
31. Gras F, Marintschev I, Wilharm A, Klos fixation for vertical shear transforaminal surgically treated pelvic ring fractures: A
K, Mückley T, Hofmann GO: 2D- sacral fractures. J Orthop Trauma 2009; prospective observational study with two
fluoroscopic navigated percutaneous 23(5):354-360. years follow-up. Injury 2010;41(4):400-
screw fixation of pelvic ring injuries: A 404.
case series. BMC Musculoskelet Disord 41. Schildhauer TA, Josten C, Muhr G:
2010;11:153. Triangular osteosynthesis of vertically 50. Gerbershagen HJ, Dagtekin O, Isenberg
unstable sacrum fractures: A new J, et al: Chronic pain and disability after
32. Bellabarba C, Ricci WM, Bolhofner BR: concept allowing early weight-bearing. pelvic and acetabular fractures:
Distraction external fixation in lateral J Orthop Trauma 1998;12(5):307-314. Assessment with the Mainz Pain Staging
compression pelvic fractures. J Orthop System. J Trauma 2010;69(1):128-136.
Trauma 2000;14(7):475-482. 42. Schildhauer TA, Ledoux WR, Chapman
JR, Henley MB, Tencer AF, Routt ML 51. Suzuki T, Shindo M, Soma K, et al:
33. Evans AR, Routt ML Jr, Nork SE, Krieg Jr: Triangular osteosynthesis and Long-term functional outcome after
JC: Oblique distraction external pelvic iliosacral screw fixation for unstable unstable pelvic ring fracture. J Trauma
fixation. J Orthop Trauma 2012;26(5): sacral fractures: A cadaveric and 2007;63(4):884-888.
322-326. biomechanical evaluation under cyclic
468 Journal of the American Academy of Orthopaedic Surgeons
You might also like
- Plastic Surgery For Trauma The Essential Survival Guide (Dorian Hobday, Ted Welman, Max Horwitz Etc.) (Z-Library)Document233 pagesPlastic Surgery For Trauma The Essential Survival Guide (Dorian Hobday, Ted Welman, Max Horwitz Etc.) (Z-Library)Cosa Catalin100% (1)
- Clinical Examination of The Wrist PDFDocument11 pagesClinical Examination of The Wrist PDFAdosotoNo ratings yet
- 01 PrestoDR 4143 and 3543 Manual MantenimientoDocument350 pages01 PrestoDR 4143 and 3543 Manual Mantenimientojeison100% (3)
- Diagnosis in OrthopaedicsDocument48 pagesDiagnosis in OrthopaedicsBakta Giri50% (2)
- Assignment 6 - Rapid Miner PDFDocument3 pagesAssignment 6 - Rapid Miner PDFAkriti JaiswalNo ratings yet
- Chapter Sixteen: Testing and Maintenance of RelaysDocument22 pagesChapter Sixteen: Testing and Maintenance of Relaysmuaz_aminu1422No ratings yet
- Advanced Endovascular Therapy of Aortic DiseaseFrom EverandAdvanced Endovascular Therapy of Aortic DiseaseAlan B. LumsdenNo ratings yet
- DR - O. K. A. SamuelsDocument76 pagesDR - O. K. A. Samuelsgdudex118811No ratings yet
- SJAMS 43B 750 754 Thesis Tibial PlateauDocument5 pagesSJAMS 43B 750 754 Thesis Tibial PlateauNisheshJainNo ratings yet
- Modified French OsteotomyDocument5 pagesModified French OsteotomyKaustubh KeskarNo ratings yet
- David Warwick (Editor), Ashley Blom (Editor), Michael Whitehouse (Editor) - Apley and Solomon - S Concise System of Orthopaedics and Trauma-CRC Press (2022)Document763 pagesDavid Warwick (Editor), Ashley Blom (Editor), Michael Whitehouse (Editor) - Apley and Solomon - S Concise System of Orthopaedics and Trauma-CRC Press (2022)filip100% (1)
- Approach To FractureDocument17 pagesApproach To FractureRebecca WongNo ratings yet
- Syllabus Ms OrthoDocument8 pagesSyllabus Ms OrthoMuthu KumarNo ratings yet
- Patellofemoral InstabilityDocument10 pagesPatellofemoral InstabilitysionforjanNo ratings yet
- Actures - In.adults.8e Booksmedicos - Org Parte4 PDFDocument1 pageActures - In.adults.8e Booksmedicos - Org Parte4 PDFeladioNo ratings yet
- Queens Orthopedic Inpatient Trauma PDFDocument27 pagesQueens Orthopedic Inpatient Trauma PDFRema AmerNo ratings yet
- Aaos Pediatric 2020Document57 pagesAaos Pediatric 2020ABUBAKER ZANBOUZINo ratings yet
- Campbell's - Open FracturesDocument7 pagesCampbell's - Open FracturesMeroly QPNo ratings yet
- Ao Final ProgramDocument16 pagesAo Final Programisprikitik3No ratings yet
- Clavo Expert LFN Diafisis FemurDocument84 pagesClavo Expert LFN Diafisis FemurC Martin TraumatoNo ratings yet
- Ficat and Arlet Staging of Avascular Necrosis of Femoral HeadDocument6 pagesFicat and Arlet Staging of Avascular Necrosis of Femoral HeadFernando Sugiarto0% (1)
- AdultHip Abstracts PDFDocument106 pagesAdultHip Abstracts PDFJafild Fild riverNo ratings yet
- Percutaneous Imaging-Guided Spinal Facet Joint InjectionsDocument6 pagesPercutaneous Imaging-Guided Spinal Facet Joint InjectionsAlvaro Perez HenriquezNo ratings yet
- 1.26 (Surgery) Orthopedic Pathology - OncologyDocument7 pages1.26 (Surgery) Orthopedic Pathology - OncologyLeo Mari Go LimNo ratings yet
- Distal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurDocument76 pagesDistal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurToàn Đặng Phan VĩnhNo ratings yet
- UKA: When Would I Do It?Document35 pagesUKA: When Would I Do It?neareastspineNo ratings yet
- Paediatric Elbow InjuriesDocument97 pagesPaediatric Elbow Injuriesrajul guptaNo ratings yet
- MPFL ReconstructionDocument16 pagesMPFL ReconstructiondrjorgewtorresNo ratings yet
- DRUJinstabilityreview - PDF 034407Document15 pagesDRUJinstabilityreview - PDF 034407Oscar Cayetano Herrera RodríguezNo ratings yet
- Orthopaedic Instruments ImagesDocument40 pagesOrthopaedic Instruments ImagesKannan KannanNo ratings yet
- Special Test KNEE UnaDocument25 pagesSpecial Test KNEE Unasingle_ladyNo ratings yet
- Workshop 1: Knots: Stage 1Document4 pagesWorkshop 1: Knots: Stage 1Noora jabeenNo ratings yet
- Orthopedics: Notes, 1/eDocument26 pagesOrthopedics: Notes, 1/evkNo ratings yet
- JB6 4 121 727Document3 pagesJB6 4 121 727Rhizka djitmauNo ratings yet
- Salter Harris Classification of Growth Plate FracturesDocument13 pagesSalter Harris Classification of Growth Plate FracturesAarón E. CaríasNo ratings yet
- Elbow WristDocument59 pagesElbow Wristdr_asalehNo ratings yet
- Charnley Ankle ArthrodesisDocument12 pagesCharnley Ankle Arthrodesisdr_s_ganeshNo ratings yet
- Flexor Tendon Surgery - 25 Years of Progress - Strickland - JHS 2000Document22 pagesFlexor Tendon Surgery - 25 Years of Progress - Strickland - JHS 2000Professeur Christian DumontierNo ratings yet
- New Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauDocument8 pagesNew Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauCosmina BribanNo ratings yet
- Avascular NecrosisDocument58 pagesAvascular Necrosischatree100% (4)
- Orthopedics Notes NeetpgDocument4 pagesOrthopedics Notes NeetpgGIST (Gujarat Institute of Science & Technology)No ratings yet
- Gopalan'S Evidence Based Orthopaedic Principles: Hitesh Gopalan U, Ms OrthDocument10 pagesGopalan'S Evidence Based Orthopaedic Principles: Hitesh Gopalan U, Ms OrthDebangshu Kumar0% (1)
- Approach To Fracture BoneDocument46 pagesApproach To Fracture BoneMuhaimin Noor AzharNo ratings yet
- Management of Segmental Bone DefectDocument11 pagesManagement of Segmental Bone DefectZin HtutNo ratings yet
- 1ry & 2ry Lesions DermatologyDocument9 pages1ry & 2ry Lesions DermatologyHassan.shehriNo ratings yet
- Paid Orthobullet MCQs - SportsDocument144 pagesPaid Orthobullet MCQs - SportsShiKid COMIX-GAMENo ratings yet
- Management of Patellofemoral Chondral InjuriesDocument24 pagesManagement of Patellofemoral Chondral InjuriesBenalNo ratings yet
- Resource Unit Wound Care EnglishDocument5 pagesResource Unit Wound Care EnglishPeterOrlinoNo ratings yet
- Why Every Spine Fusion Can Be A Deformity?Document88 pagesWhy Every Spine Fusion Can Be A Deformity?PaulMcAfeeNo ratings yet
- BooksDocument1 pageBooksAnonymous atS3ugNo ratings yet
- Tamai Zone 1 Fingertip Amputation: Reconstruction Using A Digital Artery Flap Compared With Microsurgical ReplantationDocument7 pagesTamai Zone 1 Fingertip Amputation: Reconstruction Using A Digital Artery Flap Compared With Microsurgical ReplantationFeliciaDewiNo ratings yet
- Hip Fractures-Orthoinfo - AaosDocument9 pagesHip Fractures-Orthoinfo - Aaosapi-228773845No ratings yet
- Elbow Fractures in PediatricsDocument57 pagesElbow Fractures in PediatricsKalaichelviRegunathan100% (1)
- Basic Principles of Tendon TransferDocument10 pagesBasic Principles of Tendon TransferyeapdshengNo ratings yet
- Orthopedic InjuriesDocument27 pagesOrthopedic InjuriesvikramNo ratings yet
- Traumatology Orthopaedic EXAMDocument219 pagesTraumatology Orthopaedic EXAMElo GonçalvesNo ratings yet
- Hip Dislocation: Evaluation and Management: Review ArticleDocument11 pagesHip Dislocation: Evaluation and Management: Review ArticleFadhli Aufar KasyfiNo ratings yet
- Ankle Arthrodesis - Screw FixationDocument26 pagesAnkle Arthrodesis - Screw FixationChristopher HoodNo ratings yet
- Shoulder ExamDocument12 pagesShoulder Examckyew64No ratings yet
- OITE - 2007 Hand PDFDocument35 pagesOITE - 2007 Hand PDFICH KhuyNo ratings yet
- Classification AO PediatricDocument36 pagesClassification AO PediatricdvcmartinsNo ratings yet
- Abdominal Organ Transplantation: State of the ArtFrom EverandAbdominal Organ Transplantation: State of the ArtNizam MamodeNo ratings yet
- Meniscus Root Repair Vs Meniscectomy orDocument8 pagesMeniscus Root Repair Vs Meniscectomy orJulio Cesar Guillen MoralesNo ratings yet
- Revision Lca 2 Stage 2019Document6 pagesRevision Lca 2 Stage 2019Julio Cesar Guillen MoralesNo ratings yet
- Menisco Current ConceptDocument7 pagesMenisco Current ConceptJulio Cesar Guillen MoralesNo ratings yet
- Billies Bounce EbDocument2 pagesBillies Bounce EbJulio Cesar Guillen MoralesNo ratings yet
- Fractura e FalangsDocument16 pagesFractura e FalangsJulio Cesar Guillen MoralesNo ratings yet
- Hallux RigidusDocument66 pagesHallux RigidusJulio Cesar Guillen Morales100% (1)
- Programme: P D C DDocument6 pagesProgramme: P D C DJulio Cesar Guillen MoralesNo ratings yet
- Phil. Bank Communications Vs Basic PolyprintersDocument1 pagePhil. Bank Communications Vs Basic PolyprintersNivra Lyn EmpialesNo ratings yet
- Kindergarten - Science Life CyclesDocument3 pagesKindergarten - Science Life Cyclesapi-241283264No ratings yet
- Sap S4hana FicaDocument23 pagesSap S4hana FicaSurani shaiNo ratings yet
- Saravanan MDocument4 pagesSaravanan Msaravanan007No ratings yet
- AutoCAD 1Document37 pagesAutoCAD 1first digosNo ratings yet
- Josh Moulin - Covert Entry TacticsDocument5 pagesJosh Moulin - Covert Entry TacticsJosh MoulinNo ratings yet
- Heart of SloveniaDocument51 pagesHeart of SloveniaVincenzo TorracaNo ratings yet
- S1 Data Presentation & Interpretation 1 QPDocument2 pagesS1 Data Presentation & Interpretation 1 QPAnoop SreedharNo ratings yet
- Stone VesselsDocument42 pagesStone VesselsVesna MatićNo ratings yet
- Use of Various Agricultural and Industrial Waste Materials in Road ConstructionDocument10 pagesUse of Various Agricultural and Industrial Waste Materials in Road ConstructionTime PassNo ratings yet
- Road Traffic SafetyDocument11 pagesRoad Traffic SafetySakthivel ShanmugamNo ratings yet
- LaGuardia Flight Path MapDocument1 pageLaGuardia Flight Path MaprebeccafishbeinNo ratings yet
- Circulatory SystemDocument3 pagesCirculatory Systemapi-521781723No ratings yet
- ZOO 103 Lecture 09 19 ProteinsDocument12 pagesZOO 103 Lecture 09 19 ProteinsKaelyn MontefalconNo ratings yet
- Chapter 4 Capacitance PDFDocument12 pagesChapter 4 Capacitance PDFRessyl Mae PantiloNo ratings yet
- English Workshop TIME & DATEDocument28 pagesEnglish Workshop TIME & DATEyezt0826No ratings yet
- Test Bank For Investments Analysis and Management 12th Edition JonesDocument10 pagesTest Bank For Investments Analysis and Management 12th Edition Jonesverityfelixl6e40No ratings yet
- Ipr-2018-Group A OfficersDocument73 pagesIpr-2018-Group A OfficersSneha AdepuNo ratings yet
- Singapore Tax System and Tax RatesDocument10 pagesSingapore Tax System and Tax RatesshafirasrjNo ratings yet
- Icici PoDocument5 pagesIcici Potanujchopra1No ratings yet
- Property Cases No. 10Document41 pagesProperty Cases No. 10MarinelMarquezNo ratings yet
- Class 11 Final MTSSDocument7 pagesClass 11 Final MTSSPranshu AgarwalNo ratings yet
- Syllabus of Machinery Fault Diagnosis and Signal ProcessingDocument2 pagesSyllabus of Machinery Fault Diagnosis and Signal ProcessingshreyaNo ratings yet
- Rockwell and Brinell Hardness of Metallic Materials by Portable Hardness TestersDocument5 pagesRockwell and Brinell Hardness of Metallic Materials by Portable Hardness TestersJones Pereira NetoNo ratings yet
- BFX89 BFY90: - ConductorDocument2 pagesBFX89 BFY90: - ConductorAcesNo ratings yet
- EBCR Refreshing For ResidentsDocument47 pagesEBCR Refreshing For ResidentsJohn Patria Maruli SinagaNo ratings yet
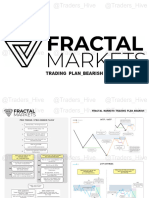
- FRACTAL MARKET Trading Plan Bearish-@Trades HiveDocument6 pagesFRACTAL MARKET Trading Plan Bearish-@Trades Hivetony nguyenNo ratings yet