Professional Documents
Culture Documents
Publication PDF
Uploaded by
Roisin McdonnellOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Publication PDF
Uploaded by
Roisin McdonnellCopyright:
Available Formats
Speech
Pathology
in Schools
A resource to support engagement and participation
of students with speech, language and
communication needs in schools.
Speech Pathology Australia: Speech Pathology in Schools Project 1
Acknowledgements
Acknowledgment is given to the members of the profession who contributed their knowledge and current literature
to this project.
Speech Pathology Australia Reference Group
Gaenor Dixon, National President, Speech Pathology Australia/ Eleanor McMillan, Speech Pathologist in Private Practice/
Principal Advisor, Therapies School Leader in the ACT Education Direcorate
Tim Kittel, Director, Speech Pathology Australia Dr Natalie Munro, Course Director BAppSc(SpPath) and Senior
Lecturer Speech Pathology, Faculty of Health Sciences, The
Alison Smith, Queensland Branch Chair/ Director Strategy and
University of Sydney, and University Associate, Curtin University
Performance, Metropolitan Region, Department of Education
and Training (Queensland) Dr Tanya Serry, Senior Lecturer, Discipline of Speech Pathology;
Chair, Human Research Ethics Sub-Committee; Honorary
Gail Mulcair, Chief Executive Officer, Speech Pathology
Research Fellow, Murdoch Childrens Research Institute, Policy
Australia
Equity and Transition Group
Candice Brady, Speech Pathologist at Children’s Hospital
Dr Julia Starling, Certified Practicing Speech-Language
at Westmead (SCHN), Leader for Advocacy and Influence –
Pathologist Adjunct Lecturer, The University of Sydney;
Speech Pathology Australia (NSW Branch)
President, Learning Difficulties Coalition of NSW
Felicity Burke, Practice Leader Speech Pathology, Clinical
Kathryn Thorburn, Speech Pathologist/Teacher Language and
Innovation and Governance, Ageing Disability and Home Care,
Learning: K-12 Speech Pathology and Learning Support
Department of Family and Community Services
Pamela Thuan, Speech Pathologist and Speech and Language
Associate Professor Patricia Eadie, Melbourne Graduate
Specialist Consultant
School of Education
Sue Wilks, Speech Pathologists/Managing Director One Stop:
Dr Charlotte Forwood, Leader of Advanced Learning –
Allied Health & Medical Centre
Strathcona Girls Grammar School
Christine Lyons, Senior Advisor – Professional Practice, Speech
Associate Professor Suze Leitao, Life Member SPA, School of
Pathology Australia
Psychology and Speech Pathology, Faculty of Health Sciences,
Curtin University Cathy Olsson, National Advisor – Disability, Speech Pathology
Australia.
Professor Sharynne McLeod, Life Member SPA, ASHA Fellow,
Professor of Speech and Language Acquisition, School of
Teacher Education, Charles Sturt University
The reference group was supported by Mary Gornik, SPA National Advisor - Education, Early Childhood and Projects.
A special thanks to Hayley Tancredi for her contribution to the section on inclusive education.
www.speechpathologyaustralia.org.au >What’s On > Schools Project Resource
For more information on the Speech Pathology Australia: Speech Pathology
in Schools Project contact Speech Pathology Australia National Advisor –
Education, Early Childhood and Projects, Mary Gornik at
mgornik@speechpathologyaustralia.org.au
Copyright: © (2017) The Speech Pathology Association of Australia Limited. Speech Pathology Australia
All rights reserved. Level 1 / 114 William Street
Disclaimer: To the best of The Speech Pathology of Australia Limited’s (‘the Melbourne Victoria 3000
Association’) knowledge, this information is valid at the time of publication. Australia
The Association makes no warranty or representation in relation to the content
or accuracy of the material in this publication. The Association expressly 1300 368 835
disclaims any and all liability (including liability for negligence) in respect of use P: +61 3 9642 4899
of information provided. The Association recommends you seek independent office@speechpathologyaustralia.org.au
professional advice prior to making any decision involving matters outlined in
this publication.
2 Speech Pathology Australia: Speech Pathology in Schools Project
Introduction
Speech Pathology Australia has produced this resource to promote a whole school
approach to support engagement and participation of students with speech,
language and communication needs in schools. We acknowledge collaboration
with the NSW Department of Education and its stakeholders to produce the
components for principals, teachers and families which will be available on their
website.
Sections of this resource may be useful to you when you are presenting
professional development forums and advocating for your role in schools, and to
educate school staff on the benefits of a whole school approach and what speech
pathologists can offer schools.
A link to the principal, teacher and parent
components will be available once they are
adapted on the NSW DoE website
Speech Pathology Australia: Speech Pathology in Schools Project 3
Contents
Context 6
The United Nations Convention on the Rights of Persons with Disabilities
The Salamanca Statement and Framework for Action on Special Needs Education
Disability Discrimination Act
Disability Standards for Education, 2005
Overview of the National Disability Strategy 2010–2020
Melbourne Declaration on Educational Goals for Young Australians (December 2008)
Prevalence of speech, language and communication needs 9
Aboriginal and Torres Strait Islanders
References
Typical speech, language and communication development 12
Common speech, language and communication needs (SLCN) 13
Markers of potential concern
Other speech, language and communication markers of needs
Complex communication needs and augmentative and alternative communication 14
References
The impact of speech, language and communication needs 18
Identifying students with speech, language and communication needs 19
Best practice models and support for students with speech, language and 20
communication needs
Why we are promoting inclusive education?
The features of inclusive education
References
Response to intervention 22
The RtI approach
Response to intervention and literacy difficulties 25
Useful references
The positive impact of providing best practice support to students 27
with speech, language and communication needs
Ensuring communication is embedded at a universal level
Skilled and confident staff can make a positive impact
Links with the curriculum
A functional approach
A strategy-focused approach
Support at transition times
Involving young people
Opportunities for specialist intervention where difficulties are severe and complex
4 Speech Pathology Australia: Speech Pathology in Schools Project
Contents
Role of teachers and speech pathologists in the educational setting 29
Collaborative partnerships
Reference
What you need to consider when working in schools 31
Workload management
Service delivery options
Employment arrangements
Employee vs. independent contractor
Clinical supervision and mentoring
Resource requirements
Ownership of files and student information
Administrative and program delivery support
Children from culturally and linguistically diverse backgrounds 34
Free resources for speech pathologists
References
The different needs of rural and regional schools 37
Telepractice considerations
Working with other speech pathologists (dual servicing)
Terminology 39
Resources 40
References 42
Prevalence and background information
Whole school approach/ response to intervention
Speech pathology evidence-based practice
Speech Pathology Australia documents
Appendix 47
Speech Pathology Australia: Speech Pathology in Schools Project 5
Context
There are several international and national The convention is international legislation and
imperatives that provide context to this resource. Australia reports on its actions towards meeting the
The most relevant ones are: The United Nations requirements regularly to the UN.
Convention on the Rights of Persons with
Disabilities, The Salamanca Statement and For you as a speech pathologist working in schools,
Framework for Action on Special Needs Education, this legislation frames your work around ensuring
the Disability Discrimination Act, Disability equal access to education for students with
Standards for Education, 2005, National Disability disability to support schools to use appropriate
Strategy 2010–2020, Melbourne Declaration on materials, techniques and forms of communication
Educational Goals for Young Australians (December for the students you support, and to provide
2008). support measures for students with speech,
language and communication needs.
The United Nations Convention on the Rights of
Persons with Disabilities The Salamanca Statement and Framework for
Action on Special Needs Education
Declaration:
“Australia recognizes that persons with disability These documents are informed by the principle
enjoy legal capacity on an equal basis with of inclusion, by recognition of the need to work
others in all aspects of life. Australia declares its towards “schools for all” – institutions which include
understanding that the Convention allows for everybody, celebrate differences, support learning,
fully supported or substituted decision-making and respond to individual needs. As such, they
arrangements, which provide for decisions to be constitute an important contribution to the agenda
made on behalf of a person, only where such for achieving education for all and for making
arrangements are necessary, as a last resort and schools educationally more effective.
subject to safeguards;
The guiding principle that informs this framework
Australia recognizes that every person with is that schools should accommodate all children
disability has a right to respect for his or her regardless of their physical, intellectual, social,
physical and mental integrity on an equal basis with emotional, linguistic or other conditions. These
others. Australia further declares its understanding conditions create a range of different challenges
that the Convention allows for compulsory to school systems. Schools have to find ways of
assistance or treatment of persons, including successfully educating all children, including those
measures taken for the treatment of mental who have serious disadvantages and disabilities.
disability, where such treatment is necessary, as a There is an emerging consensus that children and
last resort and subject to safeguards; youth with special educational needs should be
included in the educational arrangements made for
Australia recognizes the rights of persons with the majority of children. This has led to the concept
disability to liberty of movement, to freedom to of the inclusive school. The challenge confronting
choose their residence and to a nationality, on an the inclusive school is that of developing a
equal basis with others. Australia further declares its child-centred pedagogy capable of successfully
understanding that the Convention does not create educating all children, including those who have
a right for a person to enter or remain in a country serious disadvantages and disabilities. The merit
of which he or she is not a national, nor impact on of such schools is not only that they are capable
Australia’s health requirements for non-nationals of providing quality education to all children; their
seeking to enter or remain in Australia, where these establishment is a crucial step in helping to change
requirements are based on legitimate, objective and discriminatory attitudes, in creating welcoming
reasonable criteria.” communities and in developing an inclusive society.
The United Nations Convention on the Salamanca Statement 1994
Rights of Persons with Disabilities
This statement calls on schools to ensure that
they respond to the needs of all students through
the use of adjusted curriculum, organisational
6 Speech Pathology Australia: Speech Pathology in Schools Project
Context
strategies, good teaching and partnerships. The teaching that supports the learning of all students,
statement calls for schools to provide a continuum education providers make adjustments to enable
of support to meet the needs of students. every student to participate in learning.
This provides the context in which we describe the Many students, including students with disability,
Response to Intervention Strategy – the provision of need adjustments to support their learning.
a continuum of increasing frequency and intensity of
support to meet the needs of students. Under the Disability Standards for Education 2005,
students with disability are entitled to reasonable
Disability Discrimination Act adjustments to enable them to participate in
Disability is broadly defined within the Disability education on the same basis as other students.
Discrimination Act (DDA) to include physical,
intellectual, sensory, neurological and psychiatric The Education Institute > disability our
disabilities as well as including people who may rights
have a disease and people with an imputed
disability, (i.e. being treated as if you have a Overview of the National Disability Strategy
disability). People like relatives, friends, and carers 2010–2020
are also protected if they are discriminated against The National Disability Strategy 2010-2020 is
because of their association with a person with Australia’s whole of government plan for the
disability. progressive implementation of the United Nations
Convention on the Rights of Persons with
Overview Disability Discrimination Disabilities. The Australian Government undertook
Act significant consultation with people with disability,
their families and carers to inform the strategy. This
The definition of disability in the DDA is very broad process reflected the fact that people with disability
and covers a wide range of cognitive, physical, are their own experts and are best-placed to provide
sensory and social/emotional disabilities. This input on issues that affect them. Most importantly, it
includes speech language and communication ensured that the strategy was truly reflective of the
needs. priorities of people with disability across Australia.
Disability Standards for Education, 2005 The final strategy includes six core outcome areas.
The Disability Standards for Education Each of these outcome areas then includes a
are subordinate legislation to the Disability number of policy directives to help guide the work
Discrimination Act. In effect, it sets out the of governments in meeting that particular outcome.
standards that schools and education facilities must Outcome area 5 focuses on learning and skills.
adhere to in order to meet their obligations under
the Disability Discrimination Act, 1996. Outcome area 5 – learning and skills
• Strengthen the capability of all education
Children and young people in Australian education providers to deliver inclusive high quality
settings have differing needs, abilities and interests. educational programs for people with all abilities
Learning happens when teaching responds to these from early childhood through adulthood.
individual qualities. As there is no single method of
Speech Pathology Australia: Speech Pathology in Schools Project 7
Context
• Focus on reducing the disparity in educational Educational goals
outcomes for people with a disability and Goal 1
others.
Australian schooling promotes equity and
• Ensure that government reforms and initiatives excellence
for early childhood, education, training and skill
development are responsive to the needs of Goal 2
people with disability. All young Australians become:
• Improve pathways for students with disability • successful learners;
from school to further education, employment
• confident and creative individuals; and
and lifelong learning.
• active and informed citizens.
Human Rights National Disability
Strategy
Melbourne Declaration on Educational
Goals for Young Australians
Each state or territory will have its own disability
plan that guides the work that each government
agency needs to complete to meet the strategy
goals. Education departments will have contributed The Melbourne Declaration provided the basis for
to the development of the state or territory disability the development of the Australian Curriculum. The
plan, and will have their own actions arising out Australian Curriculum, Assessment and Reporting
of that plan. Being aware of the priorities for Authority (ACARA) was set up to be responsible
the department and schools can assist you in for the development of a high-quality curriculum
discussing how your work contributes to the bigger for all Australian students, one that promotes
picture. excellence and equity in education. All students are
entitled to rigorous, relevant and engaging learning
Melbourne Declaration on Educational Goals for programs drawn from a challenging curriculum that
Young Australians (December 2008) addresses their individual learning needs. The F-10
As signatories to the Melbourne Declaration, Australian Curriculum sets out the core knowledge,
Australian education ministers seek to achieve understanding, skills and general capabilities
the highest possible level of collaboration with the important for all Australian students. It describes
government, Catholic and independent school the learning entitlement of students as a foundation
sectors and across and between all levels of for successful, lifelong learning and participation in
government. Australian education ministers also the Australian community. It acknowledges that the
seek to achieve new levels of engagement with all needs and interests of students will vary, and that
stakeholders in the education of young Australians. schools and teachers will plan from the curriculum
The Melbourne Declaration acknowledges major in ways that respond to those needs and interests.
changes in the world that are placing new demands
on Australian education:
• global integration and international mobility
• globalisation and technological change
• complex environmental, social and economic
pressures
• rapid and continuing advances in information
and communication technologies.
8 Speech Pathology Australia: Speech Pathology in Schools Project
Prevalence of speech, language and
communication needs1
The following evidence will be valuable to speech general knowledge as measured by the
pathologists when performing an advocacy Australian Early Development Census at
role in schools to highlight the need for speech school entry.
pathology in the education sector.
• Children living in the most socioeconomically
• Australian estimates (from the Longitudinal disadvantaged locations were four times as
Study of Australian Children) indicate that likely to be developmentally vulnerable (falling
between 22.3 and 24.5 per cent of children below the 10th percentile) than those from
have a speech, language or communication the least disadvantaged areas in the language
disorder at school entry McLeod & Harrison, and cognitive skills domain (AECD, 2015).
2009).
• Children living in very remote Australia
• One large study based on NSW students were nearly five times more likely to be
estimated that 11 per cent of students in developmentally vulnerable in the language
secondary school have a communication and cognitive skills domain than children
disorder (McLeod & McKinnon, 2010). There living in major cities (AECD, 2015).
is no evidence to indicate that the prevalence
of communication disorders in secondary • Boys were 1.7 times more likely to be
school students would be significantly developmentally vulnerable than girls in the
different from this in other states and language and cognitive skills domain (AECD,
territories. 2015).
• Forty six percent of young offenders have a • Speech, language and communication
language impairment (Snow, 2014). difficulties are closely linked to behaviour
(Lindsay & Dockrell, 2012), social skills, self-
• There is very good evidence to indicate a esteem, health and well-being, family and
negative trajectory for these young people social relationships.
with increased incidence of disengagement
from school, poor educational outcomes, • Adolescents with speech, language and
mental ill-health, problematic behaviour, communication difficulties have been
anti-social problems and interaction shown to be at a greater risk of developing
with the juvenile justice system (Conti- emotional, social and behavioural difficulties,
Ramsden,Durking, Simkin, & Knox, 2009). mental health issues (anxiety and depression),
emotional difficulties2, early school leaving
• Over 17 per cent of children start school and poor school engagement.
with scores of “developmentally at risk” or
“vulnerable” in the language and cognitive • There is strong evidence that many students
domain (which includes pre-literacy skills), with language and learning difficulties
and over 25 per cent are at risk or vulnerable struggle enormously with the transition to
in relation to their communication skills and secondary school and may develop mental
health problems.3
1
Speech, language and communication needs (SLCN) is the umbrella term most commonly used to describe these
difficulties.
2
There is now substantial research evidence that children and young people with speech, language and
communication needs (SLCN) are more likely to develop behavioural, emotional and social difficulties (BESD) than
typically developing young people (Beitchman et al., 1996 Fujiki, Brinton, & Clarke, 2003; Tomblin et al., 2000.
Studies have shown prevalence rates as high as 35–50 per cent.
3
Communication disorders frequently co-occur with mental health issues. Bryan and Roach (2001) reported the
incidence of speech and language problems in individuals receiving mental health services to be higher than that
in the general population. Longitudinal studies have indicated an increased likelihood of mental health problems in
those who initially presented with significant speech/language impairments as a child. Developmental Language
Disorders have been found to contribute to the development pf personality disorders in adulthood.
Speech Pathology Australia: Speech Pathology in Schools Project 9
Prevalence of speech, language and
communication needs
• Students with communication problems are and 20 years compared to non-indigenous
at greater risk of bullying4 and report less children who experience 3 months of otitis
school enjoyment than their peers. media within the same period.
• Young people with communication needs • Indigenous children in 2015 were nearly
are overrepresented in juvenile justice5 four times more likely to be developmentally
settings. vulnerable than non-indigenous children in
the language and cognitive skills domain
Aboriginal and Torres Strait Islanders (AECD, 2015).
• Among Aboriginal and Torres Strait Islander
children (Williams & Jacobs, 2009), rates of • Indigenous children in 2015 were 2.4
otitis media are high, the disease manifests times more likely to be developmentally
early in life, and it may continue to occur in vulnerable than non-Indigenous children
adolescence and beyond. Australian data on the communication skills and general
indicates that Indigenous Australian children knowledge domain (19.3 and 7.9 per cent
experience otitis media for a cumulative respectively) (AECD, 2015).
total of 32 months between the ages of 2
A general pattern seen in the literature is that children with SLCN are reported to be particularly vulnerable to
4
bullying (McLaughlin et al., 2012). Given the negative links between bullying and children’s mental health (Gini
and Pozzoli, 2009), there is clearly a particular need to establish mechanisms for children with SLCN to voice their
perspectives and concerns.
5
In a 2011 study in Victoria (Snow & Powell, 2014), approximately 50 per cent of young offenders were found to
have an oral language impairment. Those with more severe types of offences performed more poorly on language
assessments.
References
Beitchman, J. H., Wilson, B., Brownlie, E. B., Walters, H., Inglis, A., Lancee, W. (1996)
Long-term consistency in speech/language profiles: 11. Behavioral, emotional and social outcomes.
Journal of the American Academy of Child & Adolescent Psychiatry, 35 (6), 815-825.
Bryan K, & Roach J. (2001) Assessment of speech and language in mental health. In: J. France &
S.Kramer (eds). Communication and mental illness. Jessica Kingsley Publishers: London. pp 110-
122.
Conti-Ramsden, G., Durkin, K., Simkin, Z. & Knoz, E., (2009). Specific language impairment and
school outcomes. 1. Identifying and explaining variability at the end of compulsory education.
International Journal of Language and Communication Disorders, 44, 15–35.
Fujiki, M., Brinton, B., and Clarke, D. (2002) Emotional regulation in children with specific language
impairment. Language, Speech, and Hearing Services in Schools. (33) 102-111.
Gini, G. and Pozzoli, T. (2009). Association between bullying and psychosomatic problems: a meta-
analysis. American Academy of Pediatrics. 123 (3).
Law, J., Rush, R., Schoon, I., & and Parsons, S. (2009). Modeling developmental language
difficulties from school entry into adulthood: literacy, mental health and employment outcomes.
Journal of Speech, Language and Hearing Research, 52, 1401–-1416.
10 Speech Pathology Australia: Speech Pathology in Schools Project
Lindsay, Geoff, and Julie E. Dockrell. (2012).The relationship between speech, language and
communication needs and behavioural, emotional and social difficulties. London, UK: Department for
Education. (Better Communication Research Programme).
McLaughlin, C., Byers, R., Oliver, C. (Eds.) (2012). Perspectives on bullying and difference:
supporting young people with special educational needs and/or disabilities in schools. (1st Ed.)
London, National Children’s Bureau.
McLeod, S., & Harrison, L. J. (2009). Epidemiology of speech and language impairment in a
nationally representative sample of 4- to 5-year-old children. Journal of Speech, Language, and
Hearing Research, 52(5), 1213–1229.
McLeod, S., and & McKinnon (2010) Support required for primary and secondary students with
communication disorders and/or other learning needs. Child Language Teacher and Therapy, 26(2),
123–143.
Snow, P. (2014). Submission to the Senate Committee Report, Community Affairs References
Committee: Prevalence of different types of speech, language and communication disorders and
speech pathology services in Australia. September, 24–25.
Snowling, M., Adams, J., Bishop, D., and & Stothard, S., (2001). Educational attainments of school
leavers with a preschool history of speech-language impairments. International Journal of Language
and Communication Disorders, 36, 173-–183.
Tomblin, J. B., Zhang, X., Buckwalter, P. and Catts, H. (2000). The association of reading disability,
behavioural disorders, and language impairment among second-grade children. The Journal of Child
Psychology and Psychiatry and Allied Disciplines, 41 (4), 473-482.
Williams, C. J. & Jacobs, M. A. (2009). The impact of otitis media on cognitive and educational
outcomes. Medical Journal of Australia, 2 Nov, 191(9 Suppl), S69–72. Retrieved October 2017, from
mja.com.au
Speech Pathology Australia: Speech Pathology in Schools Project 11
Typical speech, language and
communication development
This section is provided as a resource for increasingly sophisticated social communication
speech pathologists to use when you are skills.
required to present information to principals,
teachers and parents. Links to websites outlining All of these skills are needed to access both
developmental milestones are included below. the academic and social curriculum of school,
to cope with the demands of adolescence and
Level of educational attainment is one of the to ensure a successful onward transition to the
strongest single determinants of health on workplace.
a population basis and is heavily reliant on
language and literacy skills. As learning becomes more reliant on
independent study, language enables students
All children and young people need to have to make contact with others; to organise,
acquired well-developed speech, language manage and evaluate experiences; and to
and communication skills to reach their full influence and inform. Adolescents spend more
potential; academically, socially, vocationally, time than younger children talking to others, so
and economically. As well as being vital for becoming adept at switching between styles of
learning, speech, language and communication language. Socially, interactions become more
skills are essential across the school day – for complex and sophisticated and interaction
students to make friends, sort out problems becomes increasingly reliant on competent
and share experiences. Speech, language and communication skills; being able to hold a
communication underpin literacy and numeracy conversation and to put together sentences into
– skills which are necessary for students to a story or report (narrative) is integral to creating
understand and achieve in all key learning areas. and maintaining social relationships.
In turn, having adequate literacy skills also
contributes to children’s language skills. Speech, A focus on speech, language, and
language and communication are closely linked communication is seen by some as the key for
to behaviour, educational outcomes, social skills young people to fit into society, and language
and self-esteem. difficulties are identified as a significant risk
factor in adult outcomes (e.g., participation in
Language skills are innate and do not directly education and training, and employment). Many
need to be taught when children are developing employers place communication skills above
typically. However, literacy skills, in particular qualifications and value young people with
reading, must be explicitly taught. Children good communication, literacy and interaction
must master the basics of decoding and skills, which is why we need to support those
comprehension in the first three years of school with SLCN. Some schools have an increasing
in order to progress from “learning to read”, to emphasis on the development of functional skills
“reading to learn”. for life and work and on personal learning and
thinking skills. None of these can be achieved
Speech, language and communication needs without effective communication skills.
that are evident in a child during early to mid-
primary school do not resolve on transition For information on milestones of primary and
to secondary school without appropriate secondary school-aged students, see:
intervention. Many young people with speech,
language and communication needs struggle www.raisingchildren.net.au > language
enormously with the transition to secondary development
school and it has been shown that many
www.talkingpoint.org.uk > ages and
develop mental health problems such as anxiety
stages
and depression as a result. More sophisticated
aspects of language develop during secondary I CAN, the children’s communication
school years: complex verbal reasoning, charity (UK Registered charity 21003)
understanding and using figurative language, www.icancharity.org.uk
telling more involved stories, and using
12 Speech Pathology Australia: Speech Pathology in Schools Project
Common speech, language and
communication needs (SLCN)
The following information is included to provide Children who start school with oral language
speech pathologists with the latest advice regarding difficulties are at risk of experiencing challenges
“red flags”. when learning to read and spell.
A useful resource: Visser-Bochane, Margot I., Some children have problems with language
Gerrits, E., Van der Schans, C. P., Reijneveld, development that creates significant barriers
S. A. and Luinge, M. R. (2016). Atypical speech within everyday life or educational progress.
and language development: a consensus study Developmental language disorder (DLD) has
on clinical signs in the Netherlands. International recently emerged in the literature as the preferred
Journal of Language & Communication Disorders, term for language problems that are severe enough
52 (1), 10–20. to interfere with daily life.
Markers of potential concern
The following features are markers of potential Speech, language and communication needs
concern (red flags) for language development of can also include the following:
children. • limited eye contact;
4–5 years of age: • poor turn taking and difficulty with starting and
• At most, three-word sentences ending conversations;
• No simple sentences • problems getting the conversation back on
track after two people have talked at once, or
• Not intelligible for strangers
if there has been a misunderstanding between
• Not 50–75% intelligible for parents them;
• Disturbed interaction • difficulty understanding or responding to
• Does not understand spoken language/cannot feedback from the listener, (e.g., not noticing
process spoken language quickly enough when someone is bored or doesn’t understand
something);
5–6 years of age:
• difficulty staying on topic in conversation;
• Poorly intelligible for teacher/grandparents
• difficulty using language to negotiate in
• No adequate reaction to questions or discussions or arguments;
commands
• word finding difficulties and basic use of
• Does not understand composite commands vocabulary;
• At most, simple sentences • difficulty understanding and/or using meta
• Poor intelligibility linguistic skills such as interpreting abstract
• Does not ask questions information, inferring meaning from non-literal
language, understanding and using linguistic
6–7 years of age: devices such as cohesive devices, ellipsis and
• Does not understand composite commands humour.
• Disturbed communication
• Incomplete sentences
• No adequate reaction to questions or
commands
• Poor understanding of language
• Poor intelligibility
• Poor vocabulary
• Does not produce compound sentences
• Poor story telling
• Cluster reduction
Speech Pathology Australia: Speech Pathology in Schools Project 13
Complex communication needs and
augmentative and alternative communication
Complex communication needs (CCN) is the
term used to describe SLCN in association “The focus is not on
with cognitive, physical, perceptual, or sensory
impairments. Students with CCN may have teaching students
difficulties with understanding or using speech
and language for communication, and may use to use symbols
different modes to add to, or as an alternative
to their speech. Examples include using signs or devices, but
and gestures, a communication book or board
with symbols, or a speech output device. to support them
These are called augmentative and alternative
communication (AAC). to share meaning
CCN may lead to communication partners,
including teachers, having reduced expectations,
and involvement
and providing reduced opportunities for
communication participation and learning for
in everyday life
students with CCN (Pennington & McConchie,
1999). Attempts to communicate may not be
activities.”
recognised or acknowledged. They may have
fewer interactions and these may be shorter.
Their needs may be anticipated and they may
not be asked or expected to take their turn in
interactions or within learning activities (Harris,
Definition of AAC
An area of clinical and educational
1982; Light, Collier, & Parnes, 1985). These
practice that provides communication
reduced expectations and opportunities impact
strategies, techniques, and
on opportunities for learning and using language.
interventions for people with a range
There is a broad scope of the desired outcomes of communication limitations. The
of AAC interventions. The focus is not on term “augmentative” in this context
teaching students to use symbols or devices, means supplemental or additional to
but to support them to share meaning and speech. Augmentative techniques (e.g.,
involvement in everyday life activities. Teachers gestures, facial expressions, and items
may have trouble understanding how to of reference) are commonly used when
integrate use of AAC - Augmentative and communicating and interacting with
Alternative Communication into the learning others. The use of the term “alternative”
environment. As well as working directly with the acknowledges that there are some
student to develop their communication skills, individuals whose speech is sufficiently
the speech pathologist plays an important role impaired that they must rely completely
in supporting communication partners, both on strategies, systems, and techniques
educators and other students, to understand which do not augment speech but are
how the student communicates, and the alternatives to speech (SPA, 2013).
strategies to ensure that the student can
Purpose of AAC
participate in all activities at school, in the same
To enable the person to meet all of his/
way as other students.
her varied communication requirements
The Participation Model (Beukelman & Mirenda, as intelligibly, specifically, efficiently,
2014) provides a great framework to help identify independently and in as socially valued a
goals for classroom participation, as well as the manner as possible; and to understand
opportunity and skills based barriers which may others and to be understood (Porter,
need to be addressed to achieve these. Speech 2004).
pathologists typically play an important role in
14 Speech Pathology Australia: Speech Pathology in Schools Project
supporting those who are in the educational Research focusing on students with CCN
as well as care environment of children to who use AAC has highlighted the discrepancy
understand and use AAC modelling, including between their cognitive abilities and predicted
using aided AAC as they are speaking with the literacy skills (Sandberg, 2006). Therefore,
student, as part of naturalistic communication it is critical that professionals who work
interactions (ASHA). with students with CCN identify appropriate
AAC to promote literacy and to develop
Along with all the skills that typically developing effective strategies that foster acquisition of
children are acquiring, students with CCN skills necessary for literacy development. As
need to learn different and additional skills. For professionals with expertise in communication
example, they may need to learn to recognise and AAC, you as speech pathologists can play
symbols and understand what they represent, an important and unique role in working with
or how to “repair” interactions when the person teachers and other educational staff (as well
they are talking with misinterprets their meaning, as the student and their family) to help embed
or how and when to increase and decrease the the use of AAC to support a student’s literacy
volume of their communication device, or when development (Sturm & Clendon, 2004; Hetzroni,
to use gesture to greet someone, rather than 2004; Erickson, Koppenhaver, & Cunningham,
taking the time to generate speech output on a 2006; Porter, 1997).
device. Light’s Communication competencies
provide a useful framework to identify goals for AAC users, who may not have the ability to
intervention to support children to participate produce speech, face unique challenges in
using AAC in the educational context. (Light & the development of phonological awareness
McNaughton, 2014.) skills. The development of literacy skills for
students who are AAC users can be even
If there is a language disorder, it is likely that the more important, not only because it supports
development of literacy will also be affected. their ability to generate novel and spontaneous
Language and literacy skills do not develop utterances using text, but also because it can
in isolation but over time and are dependent provide for access to new experiences, and may
on students’ skills as well as environmental be a critical skill to enable them to enter the job
exposure and demands. Students with CCN market (Smith & Blischak, 1997).
will often need or benefit from the same
interventions as children with speech sound
disorders or developmental language disorder,
as well as requiring specific and additional
supports due to the specific and additional
barriers they face to developing literacy. For
example, children who have limited or no speech
do not have the same ability to “sound out”
words, or even to match a letter with the motor
pattern associated with that sound. (Hetzroni,
2004: Millar, Light, & McNaughton, 2004).
Children with CCN may also have changed and
reduced experiences of shared book reading,
which can impact on their opportunities to
develop literacy. For example, it may be difficult
for them to request that a favourite book is read
repeatedly. They may not have been able to ask
questions, or make comments, or “pretend” to
read a book that they have memorised, have
limited opportunities to ask questions or practice
with books (Light & Kelford-Smith, 1993).
Speech Pathology Australia: Speech Pathology in Schools Project 15
Complex communication needs and
augmentative and alternative communication
References
Beukelman, D. R., & Mirenda, P. (2013). Augmentative and alternative communication: Supporting
children and adults with complex communication needs. Baltimore, MD: Brookes
Erickson, K. A., Koppenhaver, D. A., & Cunningham, J. W. (2006). Balanced reading intervention
and assessment in augmentative communication. In R. J. McCauley, M. E. Fey, & R. Gillam (Eds.),
Treatment of language disorders in children (pp. 309–346). Baltimore, MD: Brookes).
Harris, D. (1982). Communicative interaction processes involving non-vocal physically handicapped
children, Topics in Language Disorders, 2 (2), 21-38.
Hetzroni, O. E. (2004). AAC and literacy. Disability and Rehabilitation, 26, 1305–1312.
Lund, S. K., & Light, J. (2007). Long-term outcomes for individuals who use augmentative
and alternative communication: Part III – Contributing factors. Augmentative and Alternative
Communication, 23, 323–335.
Light, J., Collier, B., & Parnes, P. (1985). Communicative interaction between young nonspeaking
physically disabled children and their primary caregivers: Part I: Discourse patterns. Augmentative
and Alternative Communication, 1(3),98-107
Light, J., & Kelford Smith, A. (1993). Home literacy experiences of pre-schoolers who use AAC
systems and of their nondisabled peers. Augmentative and Alternative Communication, 9(1), 10–25.
doi:10.1080/07434619312331276371
Light, J. C., &, McNaughton, D. (2014). Communicative competence for individuals who require
augmentative and alternative communication: A new definition for a new era of communication?
Augmentative and Alternative Communication, 30, 1–18.
Millar, D. C., Light, J. C., & McNaughton, D. B. (2004). The effect of direct instruction and
writer’s workshop on the early writing skills of children who use augmentative and alternative
communication. Augmentative and Alternative Communication, 20, 164–178.
Pennington, L. & McConachie, H. (1999). Mother–child interaction revisited: Communication with
non-speaking physically disabled children. International Journal of Language and Communication
Disorders, 34(4), 391–416.
Porter, G. (1997). Integrating AAC into programmes applying the principles of conductive education.
Conductive Education News, 12(3), 2–8.
Porter, G. (2004). AGOSCI National Tour, Adelaide.
Sandberg, A. (2006). Reading and spelling abilities in children with severe speech impairments and
cerebral palsy at 6, 9, and 12 years of age in relation to cognitive development: A longitudinal study.
Developmental Medicine & Child Neurology, 48(8), 629-634. doi:10.1017/S0012162206001344
Sennott, S.C., Light, J.C. and McNaughton, D. 2016) Research and practice for persons with severe
disabilities. Sage Journals, AAC Modeling Inervention Research Review 41, (2), 101-115.
Smith, M. M., & Blischak, D. M. (1997). Literacy. In L. L. Lloyd, D. R., Fuller, & H. H. Arvedson (Eds.),
Augmentative and alternative communication: Handbook of principles and practices (pp. 414–444).
Needham Heights, MA: Allyn and Bacon.
Speech Pathology Australia (SPA). (2012). Augmentative and alternative clinical guideline. 2012
Sturm, J. M., & Clendon, S. A. (2004). Augmentative and alternative communication, language, and
literacy: Fostering the relationship. Topics in Language Disorders, 24(1), 76–91.
16 Speech Pathology Australia: Speech Pathology in Schools Project
AAC resources
ADHC Augmentative and Alternative Communication (AAC): Guidelines for speech pathologists
who support people with disability http://www.adhc.nsw.gov.au/__data/assets/file/0011/302402/
Augmentative_and_Alternative_Communication_Practice_Guide.pdf
American Speech and Hearing Association AAC Resources https://www.asha.org/PRPSpecificTopic.
aspx?folderid=8589942773§ion=Resources
Augmentative and Alternative Communication Newsletter: Archived copies are available at http://
www.augcominc.com/newsletters/?fuseaction=newsletters&C=ACN
The focus on outcomes of communication under six (FOCUS) is a freely available resource
developed by the Bloorview McMillan Center, which can be used to measure changes in
communicative participation of pre-school children. http://www.research.hollandbloorview.ca/
outcomemeasures/focus
PrAACtical AAC School and Education related posts http://www.praacticalaac.org
The WA Independent Living Centre has a number of resources focused on supporting students
using AAC in education settings. http://www.ilc.com.au/ilc-tech-resources-communication
Commercially available AAC assessment tools
AAC Evaluation Genie App https://www.itunes.apple.com/au/app/aac-evaluation-genie/
id541418407
Augmentative and Alternative Communication Profile http://www.linguisystems.com/products/
product/display-itemid=10547
Communication Matrix http://www.communicationmatrix.org
The Pragmatics Profile of Everyday Communication Skills (Adults/Children) http://www.edit.wmin.
ac.uk/psychology/pp/children.htm
Social Networks Tool http://www.spectronicsinoz.com/product/social?networks
The Source for Augmentative Alternative Communication http://www.linguisystems.com/products/
product/display-itemid=10184
Triple C Checklist of Communication Competencies http://www.spectronicsinoz.com/product/
thetriple-c-checklist-of-communication-competencies
AAC and literacy resources
Centre for Literacy and Disability Studies https://www.med.unc.edu/ahs/clds
Caroline Musselwhite: Literacy for All http://www.engagingalllearners.ca/ip/conversation-with-
caroline-musselwhite/index.php
David Koppenhaver’s Literacy and Disability site http://www.litdis.com
Everyone Communicates - Literacy and AAC http://www.everyonecommunicates.org/resources/
literacy.html
Literacy Instruction for individuals with Autism, Cerebral Palsy, Down Syndrome and other disabilities
http://www.aacliteracy.psu.edu
PrAACtical AAC Literacy related posts http://www.praacticalaac.org
Tar Heel Reader – provides access to a wide range of books at different levels and on a range of
topics https://www.tarheelreader.org
Speech Pathology Australia: Speech Pathology in Schools Project 17
The impact of speech, language and
communication needs (SLCN)
Speech, language and communication skills Children’s social communication skills may
such as knowledge of the sounds of language, also be compromised, so that they have
phonological awareness, vocabulary, and difficulty interacting appropriately to make
the ability to understand sentence and story friends, participate in conversations, and to
structure underpin learning. Communication is negotiate and make choices, all of which are
the means by which learning is facilitated and an important part of school life. Their problems
assessed. The curriculum is heavily reliant on include use of inappropriate strategies for
oral language skills; without strong foundational negotiation and conflict resolution and difficulty
communication skills children are at risk of falling in understanding non-verbal social cues such as
behind in many areas. When children have facial expressions and gestures. These problems
ongoing difficulties in language-learning the impact on their ability to interact socially and
gap is compounded between typical language problems increase as children grow.
learners and those with speech language and
Children with speech, language and
communication needs.
communication needs are at greater risk of
Children’s communication abilities strongly bullying and report less school enjoyment than
predict their later reading skills, with a sixfold peers. Over half of children with poor speech,
increased chance of reading problems for language and communication skills also have a
children with poor language skills. Children behavioural disorder, further reducing learning
with developmental language disorders have opportunities, options and effectiveness, and
demonstrably weaker skills in areas (such as leading to disengagement from school.
their ability to remember, discriminate and
Research into the outcomes for children with
identify sounds in words, or to understand the
language impairment in early childhood identified
structure of stories) that are crucial for reading
that these children were twice as likely to show
development. In addition, their speech, language
internalising and externalising behavioural
and communication needs may impact on their
problems in later childhood and adolescence.
vocabulary, verbal reasoning skills, and their
Further, children with a history of language
ability to analyse the structure or meaning of
impairment were over 1.5 times more likely to
words and sentences, so that even if they can
meet the criteria for ADHD in later childhood
decode words while reading, they may not
or adolescence than their typically developing
understand.
peers.
18 Speech Pathology Australia: Speech Pathology in Schools Project
Identifying students with speech, language
and communication needs (SLCN)
It is often the impact of the SLCN that is most difficulties might outwardly appear to understand
evident at school – poor literacy, behaviour as they will often learn the daily classroom
problems, difficulties with peer–peer interaction, routine by watching and copying their peers, and
withdrawal from activities – rather than the readily respond to any non-verbal cues when
underlying needs, which can remain “hidden”. available. These children will tend to be very
good at “making themselves invisible” and can
The first step in the identification of a student
easily slip under the radar.
who has SLCN is noticing that they are
struggling with their communication. Teachers It is common for the language basis of academic
have a crucial role observing these difficulties. problems to go unrecognised in mid-primary and
Some students may already have been picked secondary school students. Identification by you
up by allied health practitioners, preschool as the speech pathologist should include:
teachers, or their parents may have raised
• a review of achievement tests to find
concerns. However, there are many children
students scoring poorly in the areas
and young people whose needs have not been
requiring the most complex language
identified.
demands;
If a student has a speech sound disorder or
• requesting referrals from classroom
difficulty with their spoken language, teachers
teachers;
may be able to identify it as soon they meet
them. Conversely, the issue that is hardest • a review of school reports and assessments
to detect will be difficulty in understanding for students experiencing academic failure.
language. Children with comprehension
Speech Pathology Australia: Speech Pathology in Schools Project 19
Best practice models and support for SLCN
in schools
Inclusive education is a principle that: recently clarified in General Comment No. 4
• values the well-being and unique (UN CRPD, 2016). In Australia, these rights are
contribution of every student; operationalised within the Disability Standards
• acknowledges individual requirements for Education (Australian Government, 2005).
to access and participate in an equitable Each person’s unique characteristics, interests,
education; strengths and needs in learning give rise to the
• recognises the ability of every person to need for education systems and schools to
be included both at school and in society respond to diversity in such a way that enable
more generally (UN CRPD, 2016); and access and opportunities for all students. A
is central to the achievement of high- commitment to inclusive education supports the
quality education, equity and excellence development of inclusive societies.
for all (Ministerial Council on Education, The features of inclusive education
Employment, Training and Youth Affairs,
2008). General Comment No. 4 (UN CRPD, 2016, p. 3)
outlines nine core features of inclusive education:
The international evidence indicates that 1. A “whole systems” approach to changes in
evidence-based practice in inclusive education institutional culture, policies and practices.
involves consideration support for the individual
student as well as external/environmental 2. A “whole educational environment”
modifications. commitment where educational leaders
introduce and embed inclusive culture,
Inclusive education is an ongoing process and policies and practices that will facilitate
proactive commitment to responding to the inclusive education within all areas of the
needs of all students by eliminating barriers school and school community.
to a students’ presence, access to and
achievement in education (UN CRPD, 2016; 3. A “whole person” approach, where high
UNESCO, 2017). Inclusion is not integration, expectations are the norm for all students
nor mainstreaming, where groups of diverse and flexibility within pedagogy and
students (including students with disability) curriculum is responsive to student needs.
are simply present in “regular” classrooms 4. Teacher and all other staff are supported
(Carrington & Elkins, 2002). Furthermore, it is in receiving the education and training they
not segregation, where students with diverse need to support the core values of inclusive
needs (including students with disability) are education and to work collaboratively with
educated in separate environments designed or others.
used to respond to their impairments. Effective
inclusion for all students requires a cultural, 5. Valuing and respect for diversity, as well as
policy and practice shift for both school systems listening to and responding to the needs of
and school communities. Inclusion is a process students.
of responding to diversity, where educators and 6. Building positive school communities and
school communities strive to identify and remove inclusive school environments.
all barriers to access, and optimise learning
opportunities for all (Ainscow, 2004; Ballard, 7. Implementing reasonable adjustments to
1999). learning and assessment to ensure equity.
Also, facilitating effective transitions beyond
Why we are promoting inclusive education? school into work or further study
Inclusive education is a fundamental human 8. Recognition of partnerships external
right, as has been described in Article 24 of organisations, parents/caregivers and the
The Convention on the Rights of Persons broader community.
with Disabilities (United Nations, 2006), and
20 Speech Pathology Australia: Speech Pathology in Schools Project
9. A constant process of monitoring and and learning and is adaptable to the needs of
evaluation to reflect on and continue to students in that environment.
ensure that inclusive education is being
• A range of specialist, well evidenced
upheld.
interventions (tiered interventions) to be
A best practice approach to supporting students planned and delivered by experienced
with speech, language and communication needs professionals.
is through a whole school collaborative approach
• Explicit monitoring by teachers of student
which is multi-tiered. This approach is defined as
learning so that they can be making regular
cohesive, collective and collaborative action in and
judgements about student movement
by a school community that has been strategically
between the whole school approach tiers.
constructed to improve student learning,
behaviour and well-being, and the conditions that Response to intervention (RTI) is an example
support these. of this approach that has substantial empirical
evidence. This model provides evidence-based
Key features:
classroom instruction for all children and by using
• Professionals work together with parents, a dynamic and ongoing monitoring approach,
sharing knowledge and skills to effectively the RTI model supports the identification of
support all students with an integrated students who are not responding to this “tier”.
approach. These students will need increasingly personalised
and intensive instruction, while measuring and
• Professionals know about speech, language
monitoring progress in order to make decisions
and communication, learning, curriculum and
about the need for further intervention.
the interaction between all of these elements,
with an appreciation of the wider social The focus for a response to intervention approach
context for students and their families. is enhancing the performance of all students,
including those with communication needs in the
• Professionals work together to create an
school.
environment that facilitates communication
References
Ainscow, M. (2004). Developing inclusive education systems: what are the levers for change? Journal
of Educational Change, 6(2), 109–124. doi:10.1007/s10833-005-1298-4
Australian Government. (2005). Disability Standards for Education 2005. Plus Guidance Notes. Barton,
ACT: Australian Government Publishing Service. Retrieved from October 2017, from https://www.docs.
education.gov.au/system/files/doc/other/disability_standards_for_education_2005_plus_guidance_
notes.pdf
Ballard, K. (1999). International voices: An introduction. In K. Ballard (Ed.). Inclusive education:
International voices on disability and justice. London: Falmer Press.
Carrington, C., & Elkins, J. (2002). Bridging the gap between inclusive policy and inclusive culture in
secondary schools. Support for Learning, 17(2), 51-57. doi:10.1111/1467-9604.00236
Ministerial Council on Education, Employment, Training and Youth Affairs. (2008). Melbourne
declaration on educational goals for young Australians. Canberra: Author. Retrieved October 2017,
from http://www.apo.org.au/node/29859
UN Committee on the Rights of Persons with Disabilities (CRPD). (2016). General comment No. 4
(2016), Article 24: Right to inclusive education, 2 September 2016, CRPD/C/GC/4. Retrieved October
2017, from http://www.ohchr.org/EN/HRBodies/CRPD/Pages/GC.aspx
United Nations Educational, Scientific and Cultural Organisation (UNESCO). (2017). A guide for
ensuring inclusion and equity in education. Paris: Author. Retrieved October 2017, from http://www.
allmeansall.org.au/unesco-guide-inclusion-education-including-special-school-resources-general-
system
Speech Pathology Australia: Speech Pathology in Schools Project 21
Response to Intervention (RtI)
Response (RtI) to intervention integrates • decreases the number of students
assessment and intervention within a multi- inappropriately referred for specialised
level prevention system to maximise student assessment and intervention.
achievement and to reduce behavioural
The general RtI model begins with a tiered
problems. With RtI, schools use data to identify
approach to quality evidence-based instruction
students at risk for poor learning outcomes,
that is effective for the majority of students.
monitor student progress, provide evidence-
General education and intervention specialists
based interventions and adjust the intensity and
provide evidence-based interventions and
nature of those interventions depending on a
differentiated instruction to those students
student’s responsiveness, and identify students
who are performing below expected levels of
with speech, language and communication
achievement. The RtI approach to intervention
needs.
requires teachers and specialists to work
Successful RtI programs rely on the integration together as a team to analyse data and design
of systems, data and practices. There needs a customised plan for each student who is
to be clear systems for collection of data, struggling to learn. It provides opportunities for
identification and implementation of support different professionals to learn from one another
needs; there needs to be clear data-based and to take that learning into the whole class,
decisions so data collection occurs that is small group, and individualised instruction.
purposeful and that practices are evidence
The RtI approach
based and have fidelity.
An RTI service delivery approach focuses on:
Leadership of a principal is required and the
• identifying and supporting the educational
ability to bring all educators to the same table
support requirements of all students;
to share professional development, time, space,
money, curriculum and human resources. • regular monitoring and evaluation of
processes;
RtI offers other benefits as well. It:
• matching evidence-based teaching
• helps identify the contributing factors to a
practices/interventions to student
student’s poor performance;
educational support requirements.
• promotes improved instruction through the
Tier 1
use of multiple assessments and progress
Support and train teaching staff to deliver high-
monitoring;
quality inclusive teaching that helps all students
• provides instructionally relevant data and access and participate in the curriculum. It is
emphasises effective teaching approaches; supported by effective whole-school policies and
frameworks. Speech pathologists work across
• reduces the likelihood of students
a range of proactive supports. These supports
incorrectly classified as having specific
may take the form of collaboration, capability
learning disabilities because of difficulties
development, problem-solving, interpretation
arising from various types of social
of data and curriculum support. An example of
disadvantage such as social, cultural and/or
this could include the speech pathologist team
language differences;
teaching with the classroom teacher.
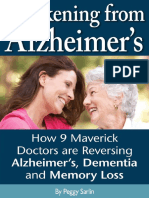
CH
Intensive Individual Intervention
OA
3
Tier
R
PP
IA
Targeted Small Group Instruction
RT
2
Tier
E
TH
Core Classroom Instruction
1
Tier
Source: Retrieved 2017 from https://www.rcps.info/departments/instruction-
al_department/virginia_tiered_systems_of_supports__rti_
22 Speech Pathology Australia: Speech Pathology in Schools Project
Tier 2 understanding of the impacts of those needs
Some students may require additional targeted on the students’ educational program, and
instruction in aspects of their learning program. support the school to develop and implement
This usually takes the form of a time-limited, appropriate individualised adjustments. The
evidence-based and structured intervention speech pathologist may, where appropriate,
programs in small groups. provide direct intervention and/or support the
provision of programs through a trained proxy
Tier 3
agent (teacher, education support staff).
Tier 3 is the provision of intensive, individualised
supports for students. This level of support It is important to understand that each tier builds
may be for only aspects of, or the whole of one on the previous one so that all students access
learning area, or may be required across many universal good teaching. Some students access
curriculum areas. targeted supports and some of those students
receive intensive supports. They are not mutually
To support the provision of effective supports
exclusive and nor are they set in stone as
for students, the speech pathologist may
students may move between tiers.
assess the students’ speech language
and communication needs, to develop an
Table 1
RTI tier Speech pathology roles
Tier 1 Professional development and coaching for teaching staff to increase
All students in the knowledge of the links between oral language, literacy and learning.
school access and Collaborating with teachers to develop and implement whole of class
participate in an or whole-of-school resources and activities that promote oral language
inclusive curriculum. competence. Working with teachers to implement and evaluate these.
For children with CCN; ensuring that there are whole-school approaches
in place for continuity of communication systems; that universal teaching
strategies are accessible; that skilled communication partners are available
throughout the school.
Collaborating with teachers to develop and implement pedagogical
strategies that support students with weak communication skills,
such as adapting lessons to reduce language complexity, marking
important information, or providing elaborations to enhance students’
comprehension; visual support, adjustments and accommodations to
access and participate in the curriculum.
Input into whole-of-school approaches to screening/identification of
children who are struggling and require Tier 2 support.
For children with CCN, collaborating with teachers and other school staff to
support access and participation for children, such as providing more time
for children to process and respond in class, ensuring that the child and
others know of and are able to access vocabulary to support participation
in their learning activity, understanding and providing aided language
stimulation6.
6
Aided language stimulation (ALS) is a communication strategy, where a communication partner teaches symbol
meaning and models language by combining his or her own verbal input with selection of vocabulary on the
augmentative and alternative communication (AAC) system. This is done by simultaneously selecting vocabulary on
the AAC system and speaking.
Comprehension and communication on the AAC system are promoted through modeled use of visual icons/graphic
symbol and providing the corresponding verbal label. Learners are prompted to use symbols to communicate within
context of motivating, frequently occurring routines by incorporation of time delays, sabotage of routines, and/or the
use of verbal cues. Prompts are faded as the AAC user gains proficiency.
Speech Pathology Australia: Speech Pathology in Schools Project 23
Response to Intervention (RtI)
RTI tier Speech pathology roles
Tier 2 Collaborative development of programs for classes or small groups
Focused support for of students to enhance skill development in specific areas, such as
students who need phonological awareness or narrative skills.
additional supports Support for evaluating the outcomes of the above, including monitoring
to access general students to determine if they are responding to this level of support and
instruction identifying students who need to move to Tier 3.
Tier 3 Comprehensive assessment, diagnosis, applications for funding (where
Individual intervention appropriate) to support educational programing for individual students.
and support Working with teachers and parents to individually plan and implement
programs to develop specific communication skills and competencies.
Delivery may be by the speech pathologist or through an aide, teacher, or
trained assistant.
Individual programing to support children to access curriculum in the
classroom. For example, developing activities that target specific skills or
allow children to use existing skills within age-appropriate curriculum.
Targeted feedback and training for teachers regarding strategies that will
support learning for an identified child.
Monitoring student outcomes to determine if more or less intensive
support is needed by using objective information to determine if students
are meeting goals.
24 Speech Pathology Australia: Speech Pathology in Schools Project
Response-to-Intervention and literacy difficulties
The RtI model offers an alternative to the provided must be of the highest quality/based
discrepancy7 model and takes an evidence- on the best available evidence. For the RtI to
based approach to determining who should be successfully implemented, a whole-school
qualify for intervention and when. It is also adoption is required.
predicated on the fact that any intervention
Table 2
RTI tier Speech pathology roles
Tier 1 Evidence-based classroom instruction in conventional literacy is provided
All students in the to all students. For students who are commencing formal reading
school access and instruction, systematic synthetic phonics instruction has consistently
participate in an been shown to be more effective compared to alternate methods
inclusive curriculum of teaching such as analytic phonics or the three cueing system. As
speech pathologists, it may be possible for you to engage in observation
of students, discussions with classroom teachers, implementation of
systematic synthetic phonics instruction with a teacher in a class, and
possibly screening, to identify children who are not responding adequately
at Tier 1. It is these students who would then be provided with Tier 2
intervention in the area or areas of need identified.
Tier 2 Involves additional targeted intervention, for example a focus on phonemic
Focused support for awareness, phonics, oral language competencies and/or speech
students who need sound errors which usually lasts for about 10-20 weeks, in addition
additional supports to mainstream classroom instruction for those students who have not
to access general responded adequately or completely to Tier 1. Tier 2 intervention is
instruction provided in small groups and may be delivered by classroom teachers,
specialists and even by well-trained volunteers (with substantial
coaching and support provided). The intervention should target specific
skill areas as needed, such as phonemic awareness, decoding, and
grapheme-phoneme correspondences. Intervention can also target oral
language competencies and comprehension-related reading skills. Tier 2
intervention is typically delivered in either the classroom or as a withdrawal
group.
As a speech pathologist, you are well-equipped to deliver this level of
intervention directly or using indirect consultative methods whereby
classroom teachers or others become the agents of the intervention. It is
critically important to collaborate with the classroom teacher rather than
working in isolation as the more co-constructed the intervention goals
are, the better for the student. Given the overwhelming evidence that
children who present with reading difficulty at an early age will not meet
year-level expectations without additional support, it is important that
Tier 2 intervention commences in a timely manner in order to maximise a
student’s literacy growth.
7
The IQ-achievement discrepancy model assesses whether there is a significant difference between a student’s
scores on a test of general intelligence and scores on an achievement test. If a student’s score on the IQ test is
at least two standard deviations higher than his or her scores on an achievement test, the student is described as
having a significant discrepancy between IQ and achievement and, therefore, as having a learning disability.
Speech Pathology Australia: Speech Pathology in Schools Project 25
Response-to-Intervention and literacy difficulties
RTI tier Speech pathology roles
Tier 3 A small proportion of students will inevitably have more severe difficulties
Individual intervention learning to read and spell. These students require Tier 3 intervention
and support which is more individualised and typically lasts for extended periods of
time. These students should receive evidence-based Tier 3 intervention
in order for optimal language and literacy gains to be realised. Tier 3
intervention is more individualised to the student’s needs and is delivered
one-to-one or perhaps in a smaller group with other students who have
similar intervention goals and importantly, should be provided with greater
intensity. For many students, the activities and strategies are similar to Tier
2 however there is:
• increased frequency of sessions per week,
• increased length of sessions,
• increased duration of the intervention from start to finish, and
• increased instructor expertise.
Useful references
Hempenstall, K. (2011). Sounding off about teaching children to read. Retrieved October 2017, from
https://www.theconversation.com/sounding-off-about-teaching-children-to-read-1012
Konza, D. (2014). Responding to the Evidence: Synthetic Phonics in Action. Retrieved October
2017, from https://www.ecu.edu.au/__data/assets/pdf_file/0006/647628/RESPONDING_TO_THE_
EVIDENCE.PDF
Moats[CT9], L. C. (1999). Teaching reading is rocket science: What expert teachers of reading
should know and be able to do.
Nation, K. (2017) Nurturing a lexical legacy: reading experience is critical for the development of
word reading skill. npj Science of Learning 2(3), 3.
Snow, P. C. (2016) Elizabeth Usher Memorial Lecture: Language is literacy is language – Positioning
speech-language pathology in education policy, practice, paradigms and polemics. International
Journal of Speech-Language Pathology 18(3), 216–228. http://www.tandfonline.com/doi/full/10.310
9/17549507.2015.1112837
Torgesen, J. K. (1998). Catch them before they fall. American Educator, 22, 32–41.
https://www.aft.org/sites/default/files/periodicals/torgesen.pdf
26 Speech Pathology Australia: Speech Pathology in Schools Project
The positive impact of providing best practice
support to students with SLCN
The features of effective practice in primary and for speech pathologists away from remediation
secondary schools, for all students, including to supporting access and participation in the
those with SLCN are numerous. The key ones curriculum thereby making language intervention
are discussed below. more meaningful for students. An approach
where specialists work closely together on
Ensuring communication is embedded aspects of the curriculum has reported benefits
at a universal level for both teachers and students. Working through
For all students, there is increasing evidence narratives is an example, through scaffolding
to show that a focus on students’ spoken story or report writing, but also through creating
(including the use of additional or alternative a communication-based curriculum or through
expressive modes, such as symbols, books focused discipline specific vocabulary teaching.
or boards) language in primary and secondary
schools can have an impact on achievement. A functional approach
Using speaking and listening activities to All students can continue to need support with
help students think for themselves has been aspects of language such as vocabulary and
highlighted as indicative of an effective school. grammar and the academic requirements of
The introduction of whole school level activities language. However, it is also important to focus
such as a consistent approach to reinforcing on associated emotional and social aspects
good listening in class leads to improved results such as friendship or independence. A focus on
in English. Support to develop communication- these functional aspects of communication is
friendly environments in primary and secondary useful for the development of all students.
schools is essential.
A strategy-focused approach
Skilled and confident staff can make a Successful learning occurs when students
positive impact reflect on their strengths and difficulties and
For all students, including those with SLCN, know what they are aiming for. The same
what adults do can have a huge impact on their applies to language – being able to reflect on
communication and educational outcomes. and analyse language is central to developing
Simple strategies such as allowing more language. Students need to know “how”, rather
processing time or directing positive feedback than just “what” to learn; strategies rather than
towards social as well as academic behaviours skills. Strategies such as listening to parents as
have been shown to increase engagement and models, practising words and asking for help
performance. Initiatives using guided learning have been identified as useful by young people.
through portfolio work and concept maps have Teaching strategies such as the use of visual
been successful in supporting the transfer of organisers, pause time for planning, and ways of
learning into practice. recognising feedback to support self-monitoring
can result in positive outcomes in both written
Links with the curriculum and spoken language.
For all students, building speech, language
and communication skills teaching into
Support at transition times
the curriculum has been shown to have The transition from preschool to primary school,
an impact both on the quality of teaching from one year level to the next, from primary to
and on social and academic outcomes for secondary school and from secondary school to
students. The curriculum used in Australian beyond school can be potentially difficult times
schools is the Australian Curriculum (www. for all students academically, organisationally
theaustraliancurriculum.edu.au). It is highly and socially. The amount of support given by the
recommended that speech pathologists have a secondary school in skills such as note taking,
look at the year level curriculum and analyse the learning how to read a timetable, understanding
language skills needed to access it. Consider what a subject area is, how to manage a diary/
student language strengths and needs, and student planner, managing assessments/
work with teachers to address the gaps. assignments and ‘how to write an essay’ are
crucial to ensuring a successful experience. Not
This represents a significant shift in approach
Speech Pathology Australia: Speech Pathology in Schools Project 27
The positive impact of providing best practice
support to students with SLCN
surprisingly, because of their difficulties in all Opportunities for specialist intervention
of these areas, students with SLCN and their where difficulties are severe and
families can find this a particularly stressful time. complex
Involving young people For students with significant and often specific
Listening to the voices of students has been SLCN there is a growing body of evidence
shown to have an impact on policy and to show the benefit of focused, specialist
practice, on learning, confidence – and also on intervention. Students with significant SLCN
communication skills. continue to need to be taught language skills
explicitly, but this needs to be planned within
Students value a focus on communication in the context of a school environment, which can
school and are very able to say what adults be challenging. The involvement of you as the
can do to support this. Students with SLCN speech pathologist is crucial – either through
can reflect on their language strengths and direct intervention or by training others. Groups
difficulties and develop good insight and run by trained teaching assistants, focusing on
awareness of the outcomes they want. Involving developing narrative or Tier 2 vocabulary8 and
young people in assessment or activities shows planned into a mainstream timetable schedule,
that they very often have different perspectives showed improved language skills. Likewise,
and priorities than adults, which can be valuable specialised and differentiated speech and
in planning support. While some young people language therapy programs, such as support
may feel support is unnecessary, others give for the use of aided AAC systems within the
insight into what is most helpful, such as learning environment or visual support for
collaborative goal setting, explicit teaching of learning grammar, integrated into the curriculum
vocabulary and visual support or use of colour can support young people to achieve a full
coding. Without this involvement, there is a risk range of academic and social outcomes.
of getting the focus of an intervention wrong.
With it, there is evidence that it can contribute to
improved engagement and behaviour.
8
Tier 2 vocabulary: high frequency words used in a variety of content domains that usually require explicit
instruction. Some examples include: complex, reasoned, contrast, hypothesise etc.
28 Speech Pathology Australia: Speech Pathology in Schools Project
Role of teachers and speech pathologists
in the educational setting
Speech pathologists can play many roles • providing collaborative in-service training
supporting the development of speech, and coaching; and
language, communication, literacy and
• collaboration when planning and
numeracy skills of primary and secondary
implementing lessons.
students. Their roles include screening,
assessing, advocating, and designing • It is important to note the speech
augmentative communication equipment in pathologist and teacher can co-teach the
addition to providing direct intervention with students in a classroom. Lessons can be
students and indirect roles of consulting, divided into teachable segments or the
coaching, collaborating, team teaching and class can be divided into groups with each
training teachers and families. In some areas, group receiving exposure to similar content
speech pathologists also function as case or one group led by the speech pathologist
managers, team leaders, and supervisors of receiving more support in the language
speech pathology assistants. area.
Speech Pathology Australia: Teacher-speech pathologist partnerships
are strengthened when both individuals
• endorses the critical role of speech
have attended professional development
pathologists in prevention, identification,
integrating communication knowledge, with
and management of speech, language,
knowledge about educational pedagogies and
fluency and literacy difficulties from infancy
the curriculum, and have the opportunities to
to adolescents;
discuss and apply this information in their own
• advocates that speech pathologists work professional settings.
collaboratively with the education team to
This approach requires collaboration at many
provide language and literacy services;
levels, including assessment, goal-setting,
• asserts speech pathologists should use planning, and implementation of intervention for
evidence-based approaches. students with communication needs as well as
for students who are at risk for language and
Those who have developed successful speech
learning problems.
pathology models in secondary schools and
have experience in using them emphasise the Importantly, no one person or profession
need for flexibility using a mixture of approaches. has sufficient expertise to execute all of the
functions associated with providing educational
It is essential that there are shared beliefs services to students with SLCN in the
between you as the speech pathologist and classroom. By working together, an effective
the school’s education team that Response- speech pathologist–teacher collaboration has
to-Intervention services support a prevention the potential to support more students more
model, provide systematic, intense, and effectively in the classroom and lead to better
evidence-based prevention/intervention, and student outcomes.
that all students can benefit from RTI. The teacher–speech pathologist team identifies
concerns regarding student performance for
Collaborative partnerships
both identified students and total classroom
The key components (McKean et al., 2016 for needs. By establishing collaborative concerns,
establishing collaborative partnerships with a the team can determine relevant curricular and
school in the delivery of services to students with speech-language goals for the whole class or
speech, language and communication needs with individual students and their families. It
are: is imperative that a collaborative team avoid
• establishing an interdisciplinary approach to planning activities before establishing the goals
working with teachers; they wish to achieve.
• demonstrating that a collaborative working There are challenges to establishing speech
relationship between yourself and the pathology–teacher collaborations as well.
school will be of value to student outcomes; Ideally we need to assist teachers to achieve a
shared understanding of your respective roles
• ensuring that the service delivery model is and expertise as a necessary and first step to
supported by teacher engagement; building a collaborative relationship. Teachers
Speech Pathology Australia: Speech Pathology in Schools Project 29
Role of teachers and speech pathologists
in the educational setting
need to be assisted to acknowledge the added Your roles as the speech pathologist in schools
value you as a speech pathologist can bring to may include one or more of the following:
their educational context, and you as a speech
• Practitioner: undertaking assessment and
pathologist must be able to maintain your
management of students’ learning needs;
intervention focus. A mutual acknowledgement
of each professions skills and knowledge base • Consultant: providing information,
and a shared language is also really important. resources and advice on supporting the
learning of students with speech, language
Teachers can take the opportunity to observe
and communication needs, to other
and reinforce strategies being taught, and you
educators and families;
as a speech pathologist will gain a greater
understanding of the skills the student needs to • Advocate and capacity builder: advocate
succeed in the classroom, curriculum and social for changes to address policy or practice
context. For students receiving intervention barriers to involvement in activities
services, in class intervention means that and participation, faced by children in
valuable instructional time from their teacher is educational settings;
not missed and promotes greater opportunities
• Educational team member: working
for generalisation. As well, “at-risk” children who
collaboratively with a range of personnel;
would not otherwise receive speech pathology
services directly, may benefit from the enhanced • Coach/mentor: supporting educational
language environment achieved through your staff to develop their ability to provide
collaboration with their teacher. appropriate supports for students;\
Communication regarding the whole service • Educator: providing theoretical and
with the principal of the school is also essential. practical information about how SLCN and
After a plan has been developed with a specific language communication needs impact on
teacher, you may need to inform the principal education outcomes across all curriculum
about the plans you have put in place together. areas;
Then check-in frequently and measure your
• Clinical supervisor of tertiary level
impact. Plans need to be well detailed and
students: disseminating expertise regarding
include the consent of the teacher(s). When
the impact of communication, mealtime
you speak with the principal, it is essential you
support needs on educational outcomes
use current terminology to describe how your
and the student’s well-being;
new approach fits into the way in which the
school provides their educational programs. • Researcher: addressing professional and
You and your teaching colleagues might also service issues.
invite the principal to visit during your time in the
classroom.
View videos of interviews
with principals, teachers,
speech pathologists and
parents.
Reference
McKean, C., Law, J., Laing, K., Cockerill, M., Allon-Smith, J., McCartney, E., & Forbes, J. (2016). A
qualitative case study in the social capital of co-professional collaborative co-practice for children
with speech, language and communication needs. International Journal of Language Communication
Disorders, 52(4), 389–539. doi:10.1111/1460-6984.12296
30 Speech Pathology Australia: Speech Pathology in Schools Project
What you need to consider when working
in schools
Before you begin work and while you are Service delivery options
working in schools, you need to consider a Changing the way service is delivered to
number of issues. Some of the key ones include students may result in a varied workload even
workload management, service delivery options, though the caseload number remains the same.
employment arrangements, clinical supervisions Consider “Who is your client?” Is the client the
and mentoring, resource requirements, school, the parent, the student, the teacher, the
ownership of files and student information, and class? This helps to frame expectations and
andministrative and program delivery support. negotiations with the Principal and teaching staff
Workload management as well as workload management. Being clear
on what your role is within the school and what
Your workload in your school needs to be
you and the school hope to achieve through the
carefully managed, especially in the situation
speech pathology service is critical to help you
where you are the only or first speech
manage your workload. The potential priorities
pathologist the school has had. The following
of a speech pathologist in any school are literally
issues need to be addressed.
endless so it is important you keep a clear line of
• How you schedule workload responsibilities sight on your role and goals.
which include direct and indirect services
(and administrative tasks) across your time
Employment arrangements
in a school is vital. It is recommended that Speech Pathology Australia recommends to
you negotiate your service and include all schools who are employing or contracting
regular points of review. a speech pathologist that they meet minimum
requirements for regulation of their practice. You,
• Determine whether there is a match or the speech pathologist must:
mismatch between your time and workload.
If there is a mismatch it is essential to • be a current financial practising member
document your concerns and to raise these of SPA with Certified Practising Speech
with the school. Pathologist CPSP status;
• Determine what activities you think are • have current (and an adequate level of)
necessary to provide appropriate support professional indemnity insurance; and
services for each student on the caseload. • have a current working with children check.
Consideration must be given to best
practice interventions, (e.g. RtI). Members of Speech Pathology Australia are
strongly encouraged to make a commitment
• Start filling available slots and supportable to read, understand and then apply SPA’s
time estimates (additional time for all of the Code of Ethics (2010) within all professional
support activities must be accounted for). interactions. It can be useful for you to explain
• Strive for a balance among the three tiers to a potential employer (school principal) how
of the RTI model and include a fourth CPSP membership ensures that you are meeting
component, administrative/management the code. You can explain that it is similar to a
tasks. teacher being registered with a teaching board.
More information is available about Professional
• When all the timeslots are filled, your Self-Regulation (PSR) on the SPA website.
caseload maximum has been reached.
When the workload responsibilities do not fit Employee vs. independent contractor
into the time slots available, you may need Principals have been advised in this resource
to discuss with the principal (or whomever that they will need to consider if they wish
you are reporting to in the management of to employ a speech pathologist directly (as
the school) to explore possible options for a school employee) or as an independent
change. Flexibility becomes an important contractor.
consideration at this step.
Speech Pathology Australia: Speech Pathology in Schools Project 31
What you need to consider when working
in schools
There may be several options such as: the health professionals and Support Services
Award (2010) at FairWork Ombudsman: Award
• sharing a speech pathologist between
Finder. FairWork have produced a pay calculator
schools (e.g., same speech pathologist for
to determine base pay rates, allowances and
primary schools who feed students to the
penalty rates for the Health Professionals and
secondary school); or
Support Services Award 2010. They also
• the school employing their own speech provide information about pay obligations, pay
pathologist; or slips and superannuation. For advice about the
award, contracts and other employment issues,
• contracting a private practitioner to work in
Speech Pathology Australia members can
their school as an independent contractor.
contact Anna Pannuzzo at Workplace Plus or on
You as a speech pathologist may be employed 0419 533 433 for free initial advice. Other useful
as a private practitioner to work with a school SPA documents which address awards, wages
as an independent contractor. You may be and employment conditions; and employment/
engaged on a contractor’s agreement, engaged contractor contracts for private practice are all
to perform a specific task or you may be available under Professional Resources on the
engaged to provide a service under a contract of SPA website:
indefinite duration.
In the latter case, it is important that you have SPA Professional Resources
a well-planned written contract with the school.
This allows you and the school to identify the Clinical supervision and mentoring
working relationship, rights and responsibilities, It is common practice in health professions for
and expected outcomes before commencing practitioners to have formal requirements for
work at the school. clinical supervision and mentoring to ensure their
Alternatively, you may be engaged as an practice is contemporary and evidence based.
employee. In this instance, like any other Speech Pathology Australia advocates minimum
employee, it is important that you receive a standards of professional support and clinical
position description with key selection criteria supervision for speech pathologists including
(KSC). It has been recommended to school newly graduated speech pathologists.
principals that another speech pathologist It is reasonable for the principal to ask you
be a part of the interview panel and that your what arrangements you have in place regarding
references are substantiated. clinical supervision and mentoring. In an
If you are employed as a school employee, employment situation, it is expected that you
then your employment conditions will need to would negotiate a need for supervision with the
abide by the industrial agreement that covers principal as part of your employment conditions.
your employment. The Health Professional Speech Pathology Australia has information on
and Support Services Award (2010) covers the role of professional support and supervision
employees (including speech pathologists) standards for members.
working in employment arrangements whether
it be private practice, private health industry Resource requirements
and the public health sector. Awards and/ The cost of speech pathology services in
or terms can vary between states so you will a school includes more than your salary or
need to check the appropriate one. Some contract costs. Consideration must be given
organisations or individuals negotiate above to the nature of the service, the number of
this award or provide additional benefits or students requiring support, the wide range of
alternative working arrangements. This award support needs within the local area, the number
is seen as the basic entitlement. Search for of schools receiving service and any specialist
32 Speech Pathology Australia: Speech Pathology in Schools Project
materials required. Speech pathology services Ownership of files and student
within a school require a budget including the information
following:
It is recommended that you formally clarify the
• salaries and on-costs; situation regarding ownership and responsibility
of files in every school that you work in (either
• administrative costs, (e.g. travel, postage, as an employee or as a contractor) and have
telephone); this written into the contract. Generally, when
• professional development; you as a health service provider creates a file,
you are the owner of that record. However, the
• educational materials for students, (e.g. ownership of records can also be affected by the
photocopying); contractual arrangements between you and the
• purchasing and maintaining specialist school. Parents need to know where their child’s
materials, (e.g. original assessments and information is being stored and who has access
forms, software/ on-line resources); and to it.
• operational costs, (e.g. utilities, cleaning). Retention of Files
Some of these resources will need to be
provided directly by a school and some by Administrative and program delivery
yourself (if you are sub-contracting into the support
school) or they may all be provided by the
school if you are employed directly. This will Like other educational staff, you will require
need to be discussed before you begin work. support for administrative duties including
answering phone calls, taking messages,
In each school where speech pathology services recordkeeping, data collection and the
are provided, you will require an appropriate preparation of materials for programs and in-
quiet, private room for some specific speech service provided by the school. The organisation
pathology activities. Access to up to date of parent meetings and obtaining consent
specialised assessments and intervention to work with students is another duty to be
equipment and tests is essential for evidence- negotiated when you are negotiating your
based practice. Principals have been advised to contract.
consider how these resources will be provided
in situations where they directly employ you or if Depending on the purpose of your speech
they have chosen to use you as an independent pathology service in the school, it is likely that
contractor. This should be discussed at the you will need to ensure that processes for
interview stage (either for an employee or collaborative program planning with teachers
contractor) to ensure that you and the principal is established. This may include negotiation
have a shared understanding of what is needed of teacher release time so that you and the
and who will provide it. teachers can work together.
Contracting a speech pathologist
Speech Pathology Australia: Speech Pathology in Schools Project 33
Children from Culturally and Linguistically
Diverse Backgrounds (CALD)9)
According to the Australian Bureau of Statistics family. Additional information is required from
(2017), many Australians do not speak English individuals from CALD backgrounds including a
at home; indeed in 2016, 72.7% of Australians comprehensive language profile and information
spoke only English at home. The most about their beliefs, concerns and reasons for
frequently spoken other languages included seeking help as these may differ from dominant
Mandarin 2.5%, Arabic 1.4%, Cantonese western perspectives on health and disability.
1.2%, Vietnamese 1.2% and Italian 1.2%. In
Case history information should be obtained in a
2016, 66.7% of people were born in Australia,
culturally respectful and ethical way. Often family
whereas 34.4% of people had both parents born
members are asked to complete a case history
overseas. To remain relevant and effective in the
form. However, this may not be appropriate as
changing landscape of the Australian population,
families may not read or speak English fluently
it is essential that your speech pathology
or understand western medical questions and
services are informed with sound knowledge
concepts. The use of an interpreter, multicultural
and equipped with the appropriate resources to
worker, or cultural broker from the family’s
support students from culturally and linguistically
cultural background may be required in order
diverse (CALD) backgrounds.
to make families feel more comfortable in the
It is also important to undertake culturally clinical setting, to explain concepts and to
sensitive services when working with Indigenous accurately collect case history information during
Australian students. This will include awareness an interview.
of local (vs. individual students’) Indigenous
Once you are aware of a student’s specific
knowledge, customs, and approaches to
language and culture from the information
learning, education and health care. Speech
collected in the case history interview, you
pathologists need to be aware of the features
should obtain information about the features of
of Aboriginal English compared with standard
significant cultural and linguistic influences, as
Australian English and acknowledge that for
well as the typical developmental characteristics
some children English (or Aboriginal English)
of the language(s)/dialect(s) that are spoken or
may not be a student’s first language, but may
signed. When explaining the assessment and
be one of eight languages spoken (McLeod,
intervention process to the family, you should be
Verdon, & Bennetts Kneebone, 2014).
sensitive to their reactions. In certain cultures it
Verdon (2015) outlines six key principles for may be offensive or cause “shame” to challenge
speech pathologists to undertake culturally a person’s abilities or to use a label to diagnose
competent practice. These are: difficulties. Therefore, cultural knowledge and
understanding on your part is essential for
1) getting to know yourself; 2) knowing
engaging in culturally competent practice with
and forming relationships with families and
diverse families.
communities; 3) setting mutually motivating
goals; 4) using appropriate tools and resources; When assessing multilingual speakers it is
5) collaborating with other key people, and 6) important to distinguish between an underlying
being flexible: one size does not fit all. speech and/or language disorder (which can
be expected to affect learning in the home
Speech Pathology Australia (2016 a, b) has
language(s) as well as English) and language
published clinical guidelines and a position paper
differences which arise from learning a second
titled Working in a Culturally and Linguistically
language. Determining whether speech and
Diverse Society that provides resources, and
language learning difficulties are evident in
additional resources are found below.
each language is most appropriate for the
Prior to planning assessment and intervention, identification of speech and/or language disorder
you will need to undertake a comprehensive in people from CALD backgrounds. Practical
case history with individuals and/or their considerations may, however, make this difficult.
9
It takes up to 5–7 years of exposure to a second language in order to be able to adequately complete standardised
testing; hence, there is a need to use other forms of assessment (criterion referenced procedures, observation,
language sampling, dynamic assessment) for children who are learning English as an additional language
(Roseberry-McKibbin, 2007).
34 Speech Pathology Australia: Speech Pathology in Schools Project
It is important that assessment take place in individual’s contexts. Factors to be taken into
the dominant language, as assessment in the account include:
non-dominant language may falsely suggest
• family preferences and attitudes;
language disorder due to a lack of exposure or
proficiency in this language. • the range of linguistic and cultural contexts
in which a person participates;
Assessment of multilingual speakers with
acquired speech and/or language disorders • current/past proficiency in both languages;
must consider patterns of use in both
• levels of English proficiency within the
languages. It is important to assess the
home;
communicative contexts in which each language
is needed. Assessment in all the multilingual • the availability of resources to support
student’s languages is recommended. intervention in the home language; and
The provision of intervention for speech, • the speech pathologist’s skills in languages
language and communication difficulties in all other than English.
of the languages spoken by an individual is the
Additionally, many factors need to be taken
current recommendation for best practice. Much
into account when selecting and implementing
research has shown that often intervention is
an alternative or augmentative communication
only provided in the language of the speech
system for use in families from CALD
pathologist (usually English) and not in the
backgrounds.
languages spoken by the person receiving
intervention. However, intervention in the home Finally, students, families, schools and
language has been found to have positive effects communities are excellent resources for
on the development of additional languages. understanding students’ cultures and languages.
Participate in cultural activities and events in
Decision-making around the choice of
order to learn and make partnerships that will
language(s) for intervention must be done
benefit your students.
in collaboration with the family and teacher
to facilitate optimal participation in all of an
Speech Pathology Australia: Speech Pathology in Schools Project 35
Children from Culturally and Linguistically
Diverse Backgrounds (CALD)9)
Free resources for speech pathologists
McLeod, S. (2017). Multilingual children’s speech [website]. Retrieved October 2017, from http://
www.csu.edu.au/research/multilingual-speech/home
McLeod, S., Verdon, S., & International Expert Panel on Multilingual Children’s Speech. (2017).
Tutorial: Speech assessment for multilingual children who do not speak the same language(s) as the
speech-language pathologist. American Journal of Speech-Language Pathology, 26(3), 691–708.
http://www.dx.doi.org/10.1044/2017_AJSLP-15-0161
Speech Pathology Australia (Verdon, S., Armstrong, H., Basso, R., Blake, H., Crowe, K., Heine,
C., Hopf, S., Huang, A., McLeod, S., Ph-m, B., Walker-Smith, K., & Webster, K.). (2016). Clinical
guideline: Working in a culturally and linguistically diverse society. Melbourne, Australia: Speech
Pathology Association of Australia.
Speech Pathology Australia (Verdon, S., Armstrong, H., Basso, R., Blake, H., Crowe, K., Heine, C.,
Hopf, S., Huang, A., McLeod, S., Ph-m, B., Walker-Smith, K., & Webster, K.) (2016). Working in a
culturally and linguistically diverse society. Position paper. Melbourne, Australia: Speech Pathology
Association of Australia.
Paradis, J., Emmerzael, K., Sorensen Duncan, T. (2010). Assessment of English language learners:
Using parent report on first language development. Journal of Communication Disorders, 43, 474-
497. www.ualberta.ca/linguistics/cheslcentre/questionnaires
References
Australian Bureau of Statistics (2017). 2016 Census QuickStats. Retrieved October 2017, from www.
censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/036
Genesee, Fred, Johanne Paradis, and Martha B. Crago. Dual language development & disorders: A
handbook on bilingualism & second language learning, Vol. 11. Paul H Brookes Publishing, 2004.
Roseberry-McKibbin, C. (2007). Language disorders in children: A multicultural and case
perspective. Boston, Pearson.
McLeod, S., Verdon, S., & Bennetts Kneebone, L. (2014). Celebrating young Indigenous Australian
children’s speech and language competence. Early Childhood Research Quarterly, 29(2), 118-131.
doi:10.1016/j.ecresq.2013.11.003
Verdon, S. (2015). Enhancing practice with culturally and linguistically diverse families: Six key
principles from the field. Journal of Clinical Practice in Speech-Language Pathology, 17(1), 2–6.
36 Speech Pathology Australia: Speech Pathology in Schools Project
The different needs of rural and regional schools
Service delivery within remote, rural and regional person and thus would not be recommended.
areas of Australia places specific demands on All speech pathologists involved in the dual
the speech pathology profession. At present, servicing arrangement must be cognisant of the
there is an increased obligation on you, the fact that they are equally ethically responsible
speech pathologist to provide the most effective for ensuring that they work cooperatively and
service possible, in the most efficient and collaboratively and that the service they provide
cost-effective manner in order to achieve a is appropriate, evidence based and consistent
greater throughput of clients. If you run a private with the client’s need.
practice, you may have a considerable waiting
When dual servicing occurs it will require careful
list and already be unable to see as many clients
planning and coordination in order to maximise
as you wish.
outcomes and not compromise the benefit to
An increased focus on evidence-based practice the client. In particular, if a client requests that an
challenges the profession to use intervention external speech pathologist provide a service in
methods which have been shown to be both a school, you, the speech pathologist must:
effective and efficacious.
• gain permission to see the client from the
Telepractice considerations person responsible (for example, the parent
Telepractice has the same delivery but there and school principal);
are technical and privacy considerations. Think • familiarise yourself with any policies and
about bandwidth and the platform used as procedures that the school may have about
schools will have specific requirements and external providers coming into that facility;
are not likely to be able to use all platforms. and
Consider collaborating with staff, and staff
requirements for provision of support through • negotiate the service agreement in
telepractice. consultation with the principal and any other
professionals involved.
Telepractice in Speech Pathology Each of the speech pathologists involved in the
Position Statement dual servicing arrangement must contribute
to the development of the client’s speech
pathology service plan. From the outset,
Working with other speech pathologists clear lines of communication will need to be
(dual servicing) established between all those involved in the
dual servicing arrangement.
Dual Servicing in Speech Pathology
The two, or more, speech pathologists in
Position Statement
consultation with the client, caregiver (if
applicable), and any other professionals involved
Dual servicing in speech pathology occurs
will need to develop a speech pathology service
when a client accesses speech pathology
plan which includes:
services from two or more speech pathologists,
frequently from different organisations or • the overall goals to be worked on;
services, at the same time. • a breakdown of the goals to be worked on
Speech Pathology Australia has determined by each speech pathologist;
that there may be some occasions where • specific roles and responsibilities for each
dual servicing in speech pathology would not speech pathologist;
achieve positive outcomes for a child or young
Speech Pathology Australia: Speech Pathology in Schools Project 37
The different needs of rural and regional schools
• how often the therapy will occur; A client who is accessing a speech pathology
service should not be excluded from accessing
• how home practice will be managed;
another speech pathology service on the basis
• how often the team will communicate and of already receiving a service. Speech Pathology
how that communication will occur. Australia is aware that some speech pathologists
work in organisations with a policy/policies
• how issues will be dealt with;
that prohibit or discourage dual servicing. SPA
• when and how the team is going to review believes that all clients should have equal access
and evaluate the delivery of the dual to services. Simply having access to one speech
services so that they ensure it continues to pathologist should not be the reason why the
meet the needs of the client. client is prohibited from accessing another
service.
38 Speech Pathology Australia: Speech Pathology in Schools Project
Terminology
Terminology
Developmental language disorder is used to refer to conditions with no known differentiating
condition. However, this does not include any nonverbal criteria – children with low normal-range
nonverbal ability can be included as cases of DLD. Generally children with intellectual disability will be
identified as having a language disorder with an identifiable genetic or neurological cause.
It is anticipated that the word “developmental” would be dropped in adulthood, leaving the diagnosis
“language disorder” – there is not a specific agreed age at which the change is made, and may
depend on the individual’s choice.
Language disorder is the adopted term for children who are likely to have language problems
enduring into middle childhood and beyond, with a significant impact on everyday social interactions
or educational progress.
Where language disorders occur as part of a more complex pattern of impairments it is suggested
that the term “language disorder associated with X” is used, where X is the differentiating condition.
Differentiating conditions may include ASD, genetic conditions such as Down syndrome and sensori-
neural hearing loss.
References
Bishop, D. V. M. Snowling, M. J., Thompson, P. A., & Greenhalgh, T. (2016). CATALISE: A
multinational and multidisciplinary Delphi consensus study. Identifying language impairments in
children. PLoS One 11(7), e0158753[CT26].
Dorothy Bishop gave a lecture for RCSLT about the project. You can view the YouTube clip here and
the summary in the RCSLT Bulletin.
Susan Ebbels also summarised the project here.
This summary has a good diagram of the questions to consider in reaching a diagnosis of DLD, and
also provides links to good research papers including Ebbels’ article in the International Journal of
Language and Communication Disorders.
Team teaching
The classroom teacher and the speech pathologist each teach from their respective areas of
expertise. Prior planning must take place for a team teaching model to be successful. The speech
pathologist and the classroom teacher must decide how they will divide the workload responsibilities
related to the classroom organisation, the type of lesson design, the materials, the behaviour
management or conflict resolution approach, time management, the materials, modifications and/
or adaptations needed, the assessment activities, and accountability exercises, (e.g. who conducts
the parent–teacher conferences). Team teaching may prove to be very time-consuming in the early
stages. Once the groundwork has been established, however, all parties benefit from providing
services to students.
Speech Pathology Australia: Speech Pathology in Schools Project 39
Resources
Other resources
Developmental language disorder
RALLI (Raising Awareness of Language Learning Impairment) now RADLD
Raising Awareness of Developmental Language Disorder Youtube clip
The Communication Trust: www.thecommunicationtrust.org.uk
LINK–S: www.linksresources.com.au
Learning Difficulties Australia: www.ldaustralia.org
Learning Difficulties Coalition of NSW: www.ldc.org.au/factsheets.html
Motif – Macquarie Online Test Interface: www.motif.org.au/home
Snowling, Maggie – Dyslexia and developmental language disorder: same or different?
Blog post
Talking Point: www.talkingpoint.org.uk
References
Prevalence and background information
Bercow, J. (2008). The Bercow Report: A review of services for children and young people (0–19)
with speech, language and communication needs.
Bishop, D. V. M., Snowling, M. J., Thompson, P. A., & Greenhalgh, T. (2016). CATALISE: a
multinational and multidisciplinary Delphi consensus study. Identifying language impairments in
children. PLoS One, 11(7), e0158753.
Clegg, J., et al. [CT29](2005). Developmental language disorders – a follow-up in later adult life:
Cognitive, language and psychosocial outcomes. Journal of Child Psychology and Psychiatry, 46(2),
128–149.
The Communication Trust (2017) Communication Commitment. UK. www.thecommunicationtrust.
org.uk
Gotsis, T. (2015). NSW school education: NAPLAN, measurement and performance. In care,
out of trouble. (2017). Report of an independent review chaired by Lord Laming. http://www.
prisonreformtrust.org.uk/Portals/0/Documents/In%20care%20out%20of%20trouble%20summary.
Lindsay, G., & Dockrell, J. E. (2012). The relationship between speech, language and communication
needs and behavioural, emotional and social difficulties.
McLeod, S. & McKinnon, D. H. (2007). Prevalence of communication disorders compared with other
learning needs in 14,500 primary and secondary school students. International Journal of Language
and Communication Disorders, 42(sup1), 37–59.
McLeod, S., & Harrison, L. J. (2009). Epidemiology of speech and language impairment in a
nationally representative sample of 4-to 5-year-old children. Journal of Speech, Language, and
Hearing Research, 52(5), 1213–1229.
McLeod, S., et al. (2015). NAPLAN outcomes for children identified with speech and language
difficulties in early childhood. Second report.
McLeod, S., et al.(2016). Multilingualism and speech-language competence in early childhood:
Impact on academic and social-emotional outcomes at school. Early Childhood Research Quarterly
34, 53–66.
Snow, P. C., & Powell, M. B. (2011). Oral language competence in incarcerated young offenders:
Links with offending severity. International Journal of Speech-Language Pathology, 13(6), 480–489.
Snow, P. C., & Powell, M. B. (2008). Oral language competence, social skills and high-risk boys:
What are juvenile offenders trying to tell us? Children and Society 22(1), 16–28.
Snow, P. C., & Powell, M. B.. (2012). Youth (in) justice: Oral language competence in early life and
risk for engagement in antisocial behaviour in adolescence. Trends and Issues in Crime and Criminal
Justice 435, 1.
Talking Point: The first stop for information on children’s communication. www.talkingpoint.org.uk/
(March 2017).
42 Speech Pathology Australia: Speech Pathology in Schools Project
References
Whole school approach/ response to intervention
American Speech-Language-Hearing Association. (2006). New roles in response to intervention:
Creating success for schools and children. Retrieved March 2017, from www.asha.org/
uploadedFiles/slp/schools/prof-consult/rtiroledefinitions.pdf
Archibald, L.. (2017). SLP-educator classroom collaboration: A review to inform reason-based
practice. Autism and Developmental Language Impairments, 2 2396941516680369.
Cirrin, F. M., Schooling, T. L., Nelson, N. W., Diehl, S. F., Flynn, P. F., Staskowski, M., et al. (2010).
Evidence-based systematic review: Effects of different service delivery models on communication
outcomes for elementary school-age children. Language, Speech, and Hearing Services in Schools,
41(3), 233–264.
Ehren, B. J., Montgomery, J., Rudebusch, J. and Whitmire, K. Responsiveness to intervention: New
roles for speech-language pathologists. Retrieved July 1 (2006): 2008.
Forbes, J. (2008). Knowledge transformations: Examining the knowledge needed in teacher and
speech and language therapist co-work. Educational review, 60(2), 141–154.
Forlin, C., Chambers, D. J., Loreman, T., Deppler, J. and Sharma, U. (2013). Inclusive education
for students with disability. A review of the best evidence in relation to theory and practice: ARACY
(2013).
From Assessment to programming: Assisting students requiring additional support in reading.
NSW DET. Retrieved March 2017, from www.schools.nsw.edu.au/media/downloads/schoolsweb/
studentsupport/programs/disabilitypgrms/assessprogad.pdf
Hartas, D. (2004). Teacher and speech-language therapist collaboration: Being equal and achieving
a common goal? Child Language Teaching and Therapy, 20(1), 33–54.
Masters, G. N. (2012). National School Improvement Tool. (2012).
McKew, M. (2014). Class act. Melbourne: Melbourne Univ. Publishing.
Mecrow, C., Beckwith, J., & Klee, T. (2010). An exploratory trial of the effectiveness of an enhanced
consultative approach to delivering speech and language intervention in schools. International
Journal of Language and Communication Disorders, 45(3), 354–367.
Moore-Brown, B. J. (1991). Moving in the direction of change: Thoughts for administrators and
speech-language pathologists. Language, Speech, and Hearing Services in Schools, 22(3), 148–
149.
Panerai, S., Zingale, M., Trubia, G., Finocchiaro, M., Zuccarello, R., Ferri, R. and Elia, M. (2009).
Special education versus inclusive education: the role of the TEACCH program. Journal of Autism
and Developmental Disorders, 39(6), 874–882.
Prelock, P. A., Miller, B. L., and Reed, N. L. (1995). Collaborative partnerships in a language in the
classroom program. Language, Speech, and Hearing Services in Schools, 26(3), 286–292.
Sage, R. (2001). Supporting primary and secondary pupils with communication and behaviour
problems. International Journal of Language and Communication Disorders, 36(S1) 423–428.
Schraeder, T. (2013). Guide to school services in speech-language pathology. Plural Publishing.
Shaddock, A. J. (2007). Improving learning outcomes for all students: Strategies for teachers who
don’t claim to be super heroes. University of Sydney Successful Learning Conference, Glebe,
Sydney.
Speech Pathology Australia: Speech Pathology in Schools Project 43
References
Snow, P. C., Sanger, D. D., Childers, C., Pankonin, C. and Wright, S. (2013). Response to
intervention in secondary settings: Speech-language pathologists’ perspectives. International journal
of speech-language pathology, 15(5), 463–470.
Snow, P., & Powell, M. (2004). Developmental language disorders and adolescent risk: A public-
health advocacy role for speech pathologists? Advances in Speech Language Pathology, 6(4),
221–229. doi:https://doi.org/10.1177/2396941516680369
Suleman, S., McFarlane, L., Pollock, K., Schneider, P., Leroy, C., Skoczylas, M. (2014). Collaboration:
More than “Working Together”: An exploratory study to determine effect of interprofessional
education on awareness and application of models of specialised service delivery by student
speech-language pathologists and teachers. Canadian Journal of Speech-Language Pathology and
Audiology, 37(4).
Throneburg, R. N., Calvert, L. K., Sturm, J. J., Paramboukas, A. A., Paul, P. J. (2000). A comparison
of service delivery models: Effects on curricular vocabulary skills in the school setting. American
Journal of Speech-Language Pathology, 9(1), 10–20.
Ukrainetz, T. A. (2006). The implications of RTI and EBP for SLPs: Commentary on LM Justice.
Language, Speech, and Hearing Services in Schools, (37), 298–303.
Vicker, B. (2009). The 21st century speech language pathologist and integrated services in
classrooms. The Reporter, 14(2),1-5,17.
Whitmire, K. A., Rivers, K. O., Mele-McCarthy, J. A., Staskowski, M. (2014). Building an
evidence base for speech-language services in the schools: Challenges and recommendations.
Communication Disorders Quarterly, 35(2), 84–92.
Wright, A., Mitchell, S., O’Donoghue, A., Cowhey, S. and Kearney, M. (2015). Making sense of it:
a brief programme to improve reading comprehension in adolescents with language impairments
in main stream school. International Journal of Language and Communication Disorders, 50(6),
776–787.
Zabiela, C., Williams, C., & Leitão, S. (2007). Service delivery in rural, remote and regional speech
pathology. ACQuiring Knowledge in Speech, Language and Hearing, 9(2), 39–47.
Speech pathology evidence-based practice
American Speech-Language-Hearing Association. (1991). A model for collaborative service delivery
for students with language-learning disorders in the public schools.
Bailey, R. L., Angell, M. E., & Stoner, J. B. (2011). Improving literacy skills in students with complex
communication needs who use augmentative/alternative communication systems. Education and
Training in Autism and Developmental Disabilities, 352–368.
Beck, A. R., & Dennis, M. (1997). Speech-language pathologists’ and teachers’ perceptions
of classroom-based interventions. Language, Speech, and Hearing Services in Schools, 28(2),
146–153.
Bhargava, D. (2011). Getting started: Using visual systems to support the development of self-
esteem. Perth, WA: Education Department WA.
Boyle, J. M., McCartney, E., O’Hare, A. and Forbes, J. (2009). Direct versus indirect and individual
versus group modes of language therapy for children with primary language impairment: Principal
outcomes from a randomized controlled trial and economic evaluation. International Journal of
Language and Communication Disorders, 44(6), 826–846.
44 Speech Pathology Australia: Speech Pathology in Schools Project
References
Brandel, J. & Loeb, D. F. (2011). Program intensity and service delivery models in the schools: SLP
survey results. Language, Speech, and Hearing Services in Schools, 42(4), 461–490.
Brent, M., Gough, F. and Robinson, S. (2001). One in eleven: Practical strategies for teaching
adolescents with a language learning disability. Melbourne: Aust Council for Ed Research.
Burns, M. K., Hodgson, J., Parker, D. C. and Fremont, K. (2011). Comparison of the effectiveness
and efficiency of text previewing and preteaching keywords as small-group reading comprehension
strategies with middle-school students. Literacy Research and Instruction, 50(3), 241–252.
Cantrell, S. C., Almasi, J. F., Carter, J. C. and Rintamaa, M. (2013). Reading intervention in middle
and high schools: Implementation fidelity, teacher efficacy, and student achievement. Reading
Psychology, 34(1), 26–58.
Cirrin, F. M., & Gillam, R. B. (2008). Language intervention practices for school-age children with
spoken language disorders: A systematic review. Language, Speech, and Hearing Services in
Schools, 39(1), S110–S137.
Dockrell, J., Lindsay, G., Roulstone, S. and Law, J. (2014). Supporting children with speech,
language and communication needs: an overview of the results of the Better Communication
Research Programme. International Journal of Language and Communication Disorders, 49(5),
543–557.
Ehren, B. J. (2002). Speech-language pathologists contributing significantly to the academic success
of high school students: A vision for professional growth. Topics in Language Disorders, 22(2),
60–80.
Eisenmajer, N., Ross, N. & Pratt, C. (2005). Specificity and characteristics of learning disabilities.
Journal of Child Psychology and Psychiatry, 46(10), 1108–1115.
Faggella-Luby, M. & Wardwell, M. (2011). RTI in a middle school: Findings and practical implications
of a tier 2 reading comprehension study. Learning Disability Quarterly, 34(1), 35–49.
Hempenstall, K. (2016). Read about it: Scientific evidence for effective teaching of reading. In
Jennifer Buckingham(Ed.).
Lang, L., Torgesen, J., Vogel, W., Chanter, C., Lefsky, E. and Petscher, Y. (2009). Exploring the
relative effectiveness of reading interventions for high school students. Journal of Research on
Educational Effectiveness, 2(2) 149–175.
Leading Learning 4 All. Retrieved March 2017, from www.leadinglearning4all.edu.au
Lee, W., & Pring, T. (2016). Supporting language in schools: Evaluating an intervention for children
with delayed language in the early school years. Child Language Teaching and Therapy, 32(2), 135-
146.
McCallum, R. S., Krohn, K. R., Skinner, C. H., Hilton-Prillhart, A., Hopkins, M., Waller, S. et al. (2011).
Improving reading comprehension of at-risk high-school students: The ART of reading program.
Psychology in the Schools, 48(1), 78–86.
McLeod, S., & McKinnon, D. H. (2010). Support required for primary and secondary students with
communication disorders and/or other learning needs. Child language teaching and therapy, 26(2),
123–143.
Norbury, C. F., Gooch, D., Wray, C., Baird, G., Charman, T., Simonoff, E. et al. (2016). The impact
of nonverbal ability on prevalence and clinical presentation of language disorder: evidence from a
population study. Journal of Child Psychology and Psychiatry, 57(11), 1247–1257.
Parsons, S., Law, J., & Gascoigne, M. (2005). Teaching receptive vocabulary to children with specific
language impairment: a curriculum-based approach. Child Language Teaching and Therapy, 21(1),
39–59.
Speech Pathology Australia: Speech Pathology in Schools Project 45
References
Paul, S-N. S., and & Clarke, P. J. (2016). A systematic review of reading interventions for secondary
school students. International Journal of Educational Research, 79, 116–127.
Serry, T. A., & Oberklaid, F. (2015). Children with reading problems: Missed opportunities to make a
difference. Australian Journal of Education, 59(1), 22–34.
Smith, L. (2007). Pelican talk speech therapy resources. Retrieved February 2017, from www.
pelicantalk.com
Snow, P. C., Eadie, T., Connell, J., Dalheim, B., McCusker, H. and Munro, J. Oral language supports
early literacy: A pilot cluster randomized trial in disadvantaged schools. International Journal of
Speech-Language Pathology, 16(5), 495–506.
Speech, language and communication in secondary aged pupils. I CAN Talk series – Issue 10.
Retrieved March 2017, from www.ican.org.uk/~/media/Ican2/Whats%20the%20Issue/Evidence/
ICAN_TalkSeries10.ashx
Starling, J., Munro, N., Togher, L. and Arciuli, J. (2011). Supporting secondary school students with
language impairment. ACQuiring Knowledge in Speech, Language and Hearing, 13(1) 26–30.
Starling, J., Munro, N., Togher, L. and Arciuli, J. (2011). Recognising language impairment in
secondary school student populations. Australian Journal of Learning Difficulties, 16(2), 145–158.
Starling, J., Munro, N., Togher, L. and Arciuli, J. (2012). Training secondary school teachers in
instructional language modification techniques to support adolescents with language impairment: A
randomized controlled trial. Language, Speech, and Hearing Services in Schools, 43, (4), 474–495.
Vandervelden, M., & Siegel, L. (1999). Phonological processing and literacy in AAC users and
students with motor speech impairments. Augmentative and Alternative Communication, 15(3),
191–211.
Speech Pathology Australia documents
Speech Pathology Australia. (2011). Speech Pathology Services in Schools Clinical Guideline.
Melbourne: Speech Pathology Australia.
Speech Pathology Australia. (2012). Augmentative and Alternative Communication Clinical Guideline.
Melbourne: Speech Pathology Australia.
Speech Pathology Australia. (2016). Speech Pathologists Working in Literacy Clinical Guideline.
Melbourne: Speech Pathology Australia.
Speech Pathology Australia. (2016). Working in a Culturally and Linguistically Diverse Society Clinical
Guideline. Melbourne: Speech Pathology Australia.
Speech Pathology Australia. (2016). Principles of Practice. Melbourne: Speech Pathology Australia.
Speech Pathology Australia. Employing or contracting a speech pathologist. Fact sheet. Melbourne.
Speech Pathology Australia.
Speech Pathology Australia.: What is a speech pathologist? Fact sheet. Melbourne. The Speech
Pathology Association of Australia Limited.
Speech Pathology Australia. (2010). Speech Pathology in Mental Health Position Statement:.
Melbourne: Speech Pathology Australia.
Speech Pathology Australia. (2011). Literacy Position Statement. Melbourne: Speech Pathology
Australia.
Speech Pathology Australia. (2014). Telepractice in Speech Pathology Position Statement.
Melbourne: Speech Pathology Australia.
46 Speech Pathology Australia: Speech Pathology in Schools Project
References
Speech Pathology Australia. (2015). Dual Servicing in Speech Pathology Position Statement.
Melbourne: Speech Pathology Australia.
Speech Pathology Australia. (2016). Working in a Culturally and Linguistically Diverse Society Position
Statement. Melbourne: Speech Pathology Australia.
Speech Pathology Australia. (2015). Proposal to the NSW’s DEC Working together to Support
Students with Speech, Language and Literacy Problems in NSW Schools. Melbourne: Speech
Pathology Australia.
Speech Pathology Australia. (2014). Submission to the Senate Community Affairs References
Committee. Inquiry into the prevalence of different types of speech, language and communication
disorders and speech pathology services in Australia.
Speech Pathology Australia. (2015). Submission to the Senate Education and Employment
References Committee. Inquiry into the current levels of access and attainment for students with
disability in the school system, and the impact on students and families associated with inadequate
levels of support.
Speech Pathology Australia. (2015). Submission to the 2015 Review of the Disability Standards for
Education. Melbourne: Speech Pathology Australia.
Speech Pathology Australia. (2017). Submission to the Parliament of New South Wales. Inquiry into
the provision of education to students with a disability or special needs in government and non-
government schools in New South Wales. Melbourne: Speech Pathology Australia.
Appendix
Australian Capital Territory – Education Directorate www.education.act.gov.au
New South Wales – Department of Education www.education.nsw.gov.au
Northern Territory – Department of Education www.education.nt.gov.au
Queensland - Department of Education and Training www.education.qld.gov.au
South Australia – Department for Education and Child development www.decd.sa.gov.au/department
Tasmania – The Department of Education www.education.tas.gov.au
Victoria – Department of Education and training www.education.vic.gov.au
Victoria – Inclusive education www.education.vic.gov.au
Western Australia – The Department of Education www.education.wa.edu.au
Speech Pathology Australia: Speech Pathology in Schools Project 47
You might also like
- Embedding Evidence-Based Practice in Speech and Language Therapy: International ExamplesFrom EverandEmbedding Evidence-Based Practice in Speech and Language Therapy: International ExamplesHazel RoddamRating: 5 out of 5 stars5/5 (1)
- Speech and Language Therapy - Speech - CerebralPalsy - OrgcerebralpalsyDocument4 pagesSpeech and Language Therapy - Speech - CerebralPalsy - OrgcerebralpalsyEileen YongNo ratings yet
- Assessment of Speech and LanguageDocument39 pagesAssessment of Speech and LanguageAmarra Astudillo RoblesNo ratings yet
- Sample Treatment PlanDocument3 pagesSample Treatment PlanLiza NaumannNo ratings yet
- Fluency Assessment ExamDocument18 pagesFluency Assessment Examapi-294798019No ratings yet
- Articulation and Phonological Processess SummarisedDocument2 pagesArticulation and Phonological Processess SummarisedSuné GreeffNo ratings yet
- AAC GuideDocument23 pagesAAC Guidejames.benedik92No ratings yet
- Efficacy of Stuttering TherapiesDocument21 pagesEfficacy of Stuttering Therapiespappu713No ratings yet
- GN Chapter 8 Communication DisordersDocument7 pagesGN Chapter 8 Communication Disordersapi-316496339No ratings yet
- What Works SLT Interventions For SLCNDocument170 pagesWhat Works SLT Interventions For SLCNlionella12No ratings yet
- Apraxia of Speech CharacteristicsDocument2 pagesApraxia of Speech CharacteristicsJoseph AngelloNo ratings yet
- Sppa 544 Articulation and Phonological DisordersDocument6 pagesSppa 544 Articulation and Phonological DisordersMaria P12No ratings yet
- Understanding Childhood Apraxia: Super Duper Handy Handouts!Document3 pagesUnderstanding Childhood Apraxia: Super Duper Handy Handouts!Staci NeustadtNo ratings yet
- Admission:Discharge Criteria in Speech-Language Pathology - ASHADocument16 pagesAdmission:Discharge Criteria in Speech-Language Pathology - ASHANádia MarquesNo ratings yet
- Augmentative and Alternative CommunicationDocument19 pagesAugmentative and Alternative Communicationt_areNo ratings yet
- 356 Phonological DisordersDocument2 pages356 Phonological DisordersWARWICKJ100% (1)
- Documentation of Diagnostic, Thearaputic and Referral Reports (Piyush Malviya)Document16 pagesDocumentation of Diagnostic, Thearaputic and Referral Reports (Piyush Malviya)Piyush Malviya100% (1)
- Speech and Language StudiesDocument17 pagesSpeech and Language StudiesafrawrrNo ratings yet
- Aphasia: Western Aphasia Battery (WAB)Document13 pagesAphasia: Western Aphasia Battery (WAB)amandaNo ratings yet
- People Games Parent HandoutDocument2 pagesPeople Games Parent HandoutFreebie SpeechieNo ratings yet
- SLP Student Intake Form Referral Consent Case HistoryDocument3 pagesSLP Student Intake Form Referral Consent Case Historyapi-617678622No ratings yet
- Template For EvalsDocument15 pagesTemplate For EvalsNGEslp13No ratings yet
- Treatment of Language Disorders (McCauley) - Rehabilita ShopDocument789 pagesTreatment of Language Disorders (McCauley) - Rehabilita ShopLuisa MantillaNo ratings yet
- Articulation Apps For Speech Therapists by GeekSLPDocument14 pagesArticulation Apps For Speech Therapists by GeekSLPBarbara FernandesNo ratings yet
- Evaluation Report - Kirsten CSCD 4396Document15 pagesEvaluation Report - Kirsten CSCD 4396Jeremy LoveNo ratings yet
- Adductor Spasmodic Dysphonia: A Case For Speech and Language TherapyDocument3 pagesAdductor Spasmodic Dysphonia: A Case For Speech and Language TherapySpeech & Language Therapy in PracticeNo ratings yet
- Speech Impairment Eligibility FluencyDocument51 pagesSpeech Impairment Eligibility FluencyRuhiyyih Devy0% (1)
- Clinical Review: Dysarthria, HypokineticDocument19 pagesClinical Review: Dysarthria, HypokineticRashid HussainNo ratings yet
- Critical Appraisal For Speech and Language Therapists: Expert OpinionDocument3 pagesCritical Appraisal For Speech and Language Therapists: Expert OpinionSpeech & Language Therapy in PracticeNo ratings yet
- Session 2 9Document15 pagesSession 2 9Ersya Muslih0% (1)
- Generic Aphasia Eval JHSPR 2014Document5 pagesGeneric Aphasia Eval JHSPR 2014ReemNo ratings yet
- Progress Report Example-Child PDFDocument3 pagesProgress Report Example-Child PDFRiang PuochNo ratings yet
- Proforma For Fluency Disorders / KUNNAMPALLIL GEJODocument2 pagesProforma For Fluency Disorders / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNNo ratings yet
- Physical Development 0-3 Years:: 3-6 MonthsDocument13 pagesPhysical Development 0-3 Years:: 3-6 MonthsAnonymous l0VyrOPNo ratings yet
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeFrom EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeNo ratings yet
- Oral and Written Language Scales Listening Comprehension and Oral Expression (OWLS)Document13 pagesOral and Written Language Scales Listening Comprehension and Oral Expression (OWLS)alessarpon7557No ratings yet
- Voice Assessment ProceduresDocument7 pagesVoice Assessment ProceduressplijaNo ratings yet
- Feeding Evaluation Report Client Name: Date Evaluated: D.O.B. TherapistDocument41 pagesFeeding Evaluation Report Client Name: Date Evaluated: D.O.B. Therapistlisa de los santos100% (1)
- Assessment and Treatment of CASDocument46 pagesAssessment and Treatment of CASPaulita Sierra Avila100% (2)
- Assessment of Speech - Sound Production PDFDocument50 pagesAssessment of Speech - Sound Production PDFAnn VillablancaNo ratings yet
- Motor Speech Skills in Down SyndromeDocument11 pagesMotor Speech Skills in Down SyndromePaulaNo ratings yet
- Language and Literacy Disorders Sivaswetha RDocument14 pagesLanguage and Literacy Disorders Sivaswetha RSriram Manikantan100% (1)
- CfyresumeDocument2 pagesCfyresumeapi-401014427No ratings yet
- Apraxia TXDocument20 pagesApraxia TXadriricaldeNo ratings yet
- 2014mshahandouts StoeckelDocument37 pages2014mshahandouts StoeckelAna Vogeley100% (1)
- SLP Case StudyDocument8 pagesSLP Case StudyMaria Fernanda Leiva ArguelloNo ratings yet
- Classification of Speech Disorders: December 2019Document21 pagesClassification of Speech Disorders: December 2019Kirti Gunjikar0% (2)
- Test Results Templates 09-11-12Document13 pagesTest Results Templates 09-11-12Shawn StevensNo ratings yet
- Assessment and Treatment of Linguistic Deficits PDFDocument96 pagesAssessment and Treatment of Linguistic Deficits PDFJumraini TammasseNo ratings yet
- The ICF Body Functions and Structures Related To Speech-Language PathologyDocument10 pagesThe ICF Body Functions and Structures Related To Speech-Language Pathologylinm@kilvington.vic.edu.auNo ratings yet
- Apraxia Kids Fast FactsDocument4 pagesApraxia Kids Fast FactsTamiris AlvesNo ratings yet
- Functional Communication AssessmentDocument1 pageFunctional Communication AssessmentRoss AdamsNo ratings yet
- Aphasia TableDocument2 pagesAphasia TableFajar Rudy QimindraNo ratings yet
- Aphasia Short Term Goals Long Term Goals Evaluation Assessment WriteUpDocument4 pagesAphasia Short Term Goals Long Term Goals Evaluation Assessment WriteUpTarienNo ratings yet
- IEP Goals and Objectives Bank Printable PDFDocument132 pagesIEP Goals and Objectives Bank Printable PDFUzma KhanNo ratings yet
- TxreportmulticulturalDocument4 pagesTxreportmulticulturalapi-294798019No ratings yet
- APPROACHES TO MANAGEMENT OF FLUENCY DISORDERS - PDF / KUNNAMPALLIL GEJODocument150 pagesAPPROACHES TO MANAGEMENT OF FLUENCY DISORDERS - PDF / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHN100% (2)
- Language and Speech DevelopmentDocument23 pagesLanguage and Speech DevelopmentR'punzel CurlyNo ratings yet
- Vertical Root FractureDocument26 pagesVertical Root FractureAkash RautNo ratings yet
- MG Hse Bulletin 01 2020 The Take 5 For SafetyDocument1 pageMG Hse Bulletin 01 2020 The Take 5 For SafetyvivekNo ratings yet
- Understanding Emotion in Trading: Course 1. Forex Basic Knowledge Course - From Zero To ExpertDocument10 pagesUnderstanding Emotion in Trading: Course 1. Forex Basic Knowledge Course - From Zero To ExpertAhmedNo ratings yet
- Restaurant Report Card - December 2, 2021Document3 pagesRestaurant Report Card - December 2, 2021KBTXNo ratings yet
- MLC Title 1.1 Young Persons: Marine - Survey@gov - ImDocument7 pagesMLC Title 1.1 Young Persons: Marine - Survey@gov - ImTan DatNo ratings yet
- About The STS Risk Calculator v2 81Document4 pagesAbout The STS Risk Calculator v2 81raghesh VNo ratings yet
- 2021 Salmon Industry HandbookDocument118 pages2021 Salmon Industry HandbookLeydi Yessenia Huerta VillanuevaNo ratings yet
- Richard Corbeil - Vocal Integration - CD Cover (2007)Document1 pageRichard Corbeil - Vocal Integration - CD Cover (2007)tradingaopNo ratings yet
- Vimal PAD - SlidesDocument53 pagesVimal PAD - SlidesVimal NishadNo ratings yet
- Awakening From AlzheimersDocument138 pagesAwakening From AlzheimersCynthia Breman-Rooke92% (13)
- 0000000saudi Aramco Gi PDFDocument12 pages0000000saudi Aramco Gi PDFKrunalNo ratings yet
- M. Hill Physiology (16) Regulation of Arterial PressureDocument28 pagesM. Hill Physiology (16) Regulation of Arterial PressureEfrain AnayaNo ratings yet
- Per Dev Module 4Document8 pagesPer Dev Module 4Marciana JulianNo ratings yet
- A. Classification: Taenia Solium and Taenia SaginataDocument8 pagesA. Classification: Taenia Solium and Taenia SaginataadhiNo ratings yet
- Badger Airbrush Model 175 CrescendoDocument12 pagesBadger Airbrush Model 175 CrescendoKristel ClearyNo ratings yet
- Om 1531026 0102Document270 pagesOm 1531026 0102chinh nguyenNo ratings yet
- Skryabin 2021Document14 pagesSkryabin 2021cupin 69PKNo ratings yet
- EPIQ Elite and Affiniti Portfolio: UltrasoundDocument4 pagesEPIQ Elite and Affiniti Portfolio: UltrasoundNam LeNo ratings yet
- Edition 4.0: Please Input The Below Numbers : Subject-Wise Study Time CalculatorDocument2 pagesEdition 4.0: Please Input The Below Numbers : Subject-Wise Study Time Calculatorsuraj kantNo ratings yet
- 台 灣 漢 族 酒 癮 者 以 ALDH2對 偶 基 因 型 分 組 後 於 酒 精 效 果 預 期 、 酒 癮 渴 求 與 飲 酒 量 之 差 異 The Differences in Alcohol Outcome Expectancy, Alcohol Craving and Alcohol Consumption betweenDocument80 pages台 灣 漢 族 酒 癮 者 以 ALDH2對 偶 基 因 型 分 組 後 於 酒 精 效 果 預 期 、 酒 癮 渴 求 與 飲 酒 量 之 差 異 The Differences in Alcohol Outcome Expectancy, Alcohol Craving and Alcohol Consumption betweenjennyNo ratings yet
- Study - Id82560 - Digital Health in IndiaDocument50 pagesStudy - Id82560 - Digital Health in IndiaharishNo ratings yet
- Ephedrine: DR Henny RachdiatiDocument20 pagesEphedrine: DR Henny Rachdiatitiara rizkiaNo ratings yet
- Seven Secrets of The Killer Resume: AuthorDocument3 pagesSeven Secrets of The Killer Resume: AuthorjayNo ratings yet
- Pediatric Mock Resuscitation ScenariosDocument6 pagesPediatric Mock Resuscitation ScenariosdinkytinkNo ratings yet
- Developing Early Childhood Curriculum in Australia - 1600wordsDocument8 pagesDeveloping Early Childhood Curriculum in Australia - 1600wordsNguyễn Hải AnhNo ratings yet
- An Investigation Into The Barriers To and Priorities For Research Engagement in Health LibrarianshipDocument22 pagesAn Investigation Into The Barriers To and Priorities For Research Engagement in Health LibrarianshipKrisha FernandezNo ratings yet
- Methods of ResearchDocument35 pagesMethods of ResearchGerik JavonilloNo ratings yet
- CPP Mini Cex Form v1.0Document2 pagesCPP Mini Cex Form v1.0bobfooNo ratings yet
- Jacob Levy Morenos Psychodrama As A Work TechniquDocument12 pagesJacob Levy Morenos Psychodrama As A Work TechniquAdriana EneNo ratings yet
- Fizioterapie MasectomieDocument46 pagesFizioterapie MasectomieSimona SăvucăNo ratings yet