You might also like
- XN-Series Clinical Case Report Vol. 2Document71 pagesXN-Series Clinical Case Report Vol. 2Görünmez gorunur100% (3)
- PRM03 Resource Planning Template - AdvancedDocument142 pagesPRM03 Resource Planning Template - AdvancedFernandoNo ratings yet
- Measuring The Interprofessional Collaborative Competencies of Health Care Students Using A Validated Indonesian Version of The CICS29Document10 pagesMeasuring The Interprofessional Collaborative Competencies of Health Care Students Using A Validated Indonesian Version of The CICS29AMIGOMEZNo ratings yet
- Collaboration of General and Special EducationDocument8 pagesCollaboration of General and Special EducationAzra HadžićNo ratings yet
- Thacker - An Ideal For Living - An Anti-Novel PDFDocument115 pagesThacker - An Ideal For Living - An Anti-Novel PDFantonio damataNo ratings yet
- Siare-Ge Press en PDFDocument1 pageSiare-Ge Press en PDFNoel SamNo ratings yet
- Concepts & Applications of E-BusinessDocument319 pagesConcepts & Applications of E-BusinessMohammed Mohammed Shoukry Naiem0% (1)
- How To Read and Write To T24 JMeterDocument2 pagesHow To Read and Write To T24 JMeterrosjaviNo ratings yet
- Narcisism and Its Discontents. Julie WalshDocument190 pagesNarcisism and Its Discontents. Julie WalshCalvacanti100% (3)
- Impact of Team Composition On Student Perceptions of Interprofessional Teamwork: A 6-Year Cohort StudyDocument9 pagesImpact of Team Composition On Student Perceptions of Interprofessional Teamwork: A 6-Year Cohort Studysasha geganaresi liardiNo ratings yet
- Impact of A Faculty Development Course On Relationship-Centered Communication SkillsDocument7 pagesImpact of A Faculty Development Course On Relationship-Centered Communication SkillstarapacawarezNo ratings yet
- Review IPCP Blok 4.5 2021Document25 pagesReview IPCP Blok 4.5 2021alyaNo ratings yet
- Surian Di Masi Supporting HE Frontiers 2017Document7 pagesSurian Di Masi Supporting HE Frontiers 2017asurianNo ratings yet
- YU and KoDocument5 pagesYU and KoFatmaxanimNo ratings yet
- Sicometrik ICP IndonesiaDocument10 pagesSicometrik ICP IndonesiaUchi SuhermanNo ratings yet
- Interprofessionals CompetenceDocument7 pagesInterprofessionals CompetenceGianmarco FerrariNo ratings yet
- Innovations in Education and Teaching InternationalDocument12 pagesInnovations in Education and Teaching InternationalNis NosNo ratings yet
- Article 2 (Teamwork) MGT648 PDFDocument9 pagesArticle 2 (Teamwork) MGT648 PDFNatasya ShaNo ratings yet
- Evans 2017Document12 pagesEvans 2017Novena MariaNo ratings yet
- AssessmentDocument9 pagesAssessmentdian maya puspitaNo ratings yet
- Transfer of Learning Using Simulation Based Education Among Students of Teaching InstitutionsDocument5 pagesTransfer of Learning Using Simulation Based Education Among Students of Teaching InstitutionsEditor IJTSRDNo ratings yet
- Barron 2017Document17 pagesBarron 2017Widiastuti Ledgeriana MugiriNo ratings yet
- Survey of Interprofessional CoDocument19 pagesSurvey of Interprofessional CorahmaNo ratings yet
- Development and Validation of An Enlarged Version of The Student Agentic Engagement ScaleDocument14 pagesDevelopment and Validation of An Enlarged Version of The Student Agentic Engagement ScaleNguyễnHoàngPhúcANo ratings yet
- Interprofesional Education (IPE) Meningkatkan Kemampuan KomunikasiDocument13 pagesInterprofesional Education (IPE) Meningkatkan Kemampuan KomunikasiNur Ainaa Almardhiyah TubungNo ratings yet
- Gandes IPE S2 KeperawatanDocument31 pagesGandes IPE S2 KeperawatanPinkinNo ratings yet
- Peer To PeerDocument7 pagesPeer To PeerChandra Hidayat RcrNo ratings yet
- Effectiveness of Interprofesional Education Implementation in Health Services: Literature ReviewDocument13 pagesEffectiveness of Interprofesional Education Implementation in Health Services: Literature Reviewtotok wahyudiNo ratings yet
- 1 s2.0 S1471595316301275 MainDocument8 pages1 s2.0 S1471595316301275 MainWarsonoNo ratings yet
- Nisbet Et Al. (2016) PDFDocument11 pagesNisbet Et Al. (2016) PDFKennedy AlecrimNo ratings yet
- Giving Feedback Effectively in The Clinical EnvironmentDocument5 pagesGiving Feedback Effectively in The Clinical EnvironmentMAurcioNo ratings yet
- A Framework For Interprofessional Team Collaboration in A Hospital Setting: Advancing Team Competencies and BehavioursDocument6 pagesA Framework For Interprofessional Team Collaboration in A Hospital Setting: Advancing Team Competencies and BehavioursGendi CynthiaNo ratings yet
- Coaching The DebrieferDocument7 pagesCoaching The DebrieferLan AnhNo ratings yet
- Interprofessional Education (Ipe) Improves Students' Communication Skills: A Literature ReviewDocument11 pagesInterprofessional Education (Ipe) Improves Students' Communication Skills: A Literature Reviewfransiskus mekuNo ratings yet
- IPEM NotesDocument28 pagesIPEM NotesJelcy MangulabnanNo ratings yet
- Factors Affecting MetacognitionDocument9 pagesFactors Affecting MetacognitionZilbran BerontaxNo ratings yet
- Framed Autoethnography As An Approach For UncoveriDocument9 pagesFramed Autoethnography As An Approach For UncoveriSullyvan GarciaNo ratings yet
- Interprofessional Education - The Way Forward in Health ProfessionDocument2 pagesInterprofessional Education - The Way Forward in Health ProfessionJLatriece Elizabeth CedeñoNo ratings yet
- Interprofessional Collaboration Three Best Practice Models of Interprofessional EducationDocument11 pagesInterprofessional Collaboration Three Best Practice Models of Interprofessional Educationgenta01100% (1)
- Owen 2014Document6 pagesOwen 2014David PintoNo ratings yet
- International Journal of Nursing Sciences: Yi Yang, Huaping Liu, Gwen D. SherwoodDocument9 pagesInternational Journal of Nursing Sciences: Yi Yang, Huaping Liu, Gwen D. SherwoodAbdulRahman MuthannaNo ratings yet
- Preparing Nursing Students For Interprofessional Learning: June 2014Document7 pagesPreparing Nursing Students For Interprofessional Learning: June 2014Ahmad Tri Anggara SasmitaNo ratings yet
- Enfermeria, 2019Document10 pagesEnfermeria, 2019aminNo ratings yet
- Agreli, Peduzzi e Bailey. Contributions of Team Climate in The Study of Interprofessional Collaboration OkDocument8 pagesAgreli, Peduzzi e Bailey. Contributions of Team Climate in The Study of Interprofessional Collaboration OkFernanda BragaNo ratings yet
- Educación Interprofesional (IPE) Basada en Simulación para Mejorar La Actitud y El Trabajo en Equipo de Los Residentes de Anestesiología y Los Estudiantes de Enfermería de Anestesia en IránDocument8 pagesEducación Interprofesional (IPE) Basada en Simulación para Mejorar La Actitud y El Trabajo en Equipo de Los Residentes de Anestesiología y Los Estudiantes de Enfermería de Anestesia en IránEmily Garcia EspinozaNo ratings yet
- Learning Organization and Work Engagement: The Mediating Role of Employee ResilienceDocument25 pagesLearning Organization and Work Engagement: The Mediating Role of Employee ResilienceAmy BCNo ratings yet
- Jurnal IpeDocument11 pagesJurnal IpemusaffaNo ratings yet
- Interprofessional Collaboration Three Best Practice Models of Interprofessional EducationDocument11 pagesInterprofessional Collaboration Three Best Practice Models of Interprofessional Educationanzila widyaNo ratings yet
- Knowledge Self-Efficacy and Research Collaboration Towards Knowledge Sharing: The Moderating Effect of Employee CommitmentDocument8 pagesKnowledge Self-Efficacy and Research Collaboration Towards Knowledge Sharing: The Moderating Effect of Employee CommitmentIAEME PublicationNo ratings yet
- MacDonald2017 ModelofCog-ComCompetenceDocument23 pagesMacDonald2017 ModelofCog-ComCompetenceconstanza duran cordovaNo ratings yet
- Naskah Publikasi FixDocument14 pagesNaskah Publikasi FixSabet LilyNo ratings yet
- Blended Learning Approach Promotes The Applicationin Orthopedics, A Mixed Prospective StudyDocument11 pagesBlended Learning Approach Promotes The Applicationin Orthopedics, A Mixed Prospective StudyIJAR JOURNALNo ratings yet
- Interprofessional Education and Collaboration Among Healthcare Students and Professionals A Systematic Review and Call For ActionDocument19 pagesInterprofessional Education and Collaboration Among Healthcare Students and Professionals A Systematic Review and Call For ActionNguyên NguyễnNo ratings yet
- Women and Birth: Linda Sweet, Janice Bass, Mary Sidebotham, Jennifer Fenwick, Kristen GrahamDocument8 pagesWomen and Birth: Linda Sweet, Janice Bass, Mary Sidebotham, Jennifer Fenwick, Kristen GrahamDian OktavianiNo ratings yet
- Collaboration Skill of Biology Students at Universitas Islam Riau IndonesiaDocument4 pagesCollaboration Skill of Biology Students at Universitas Islam Riau IndonesiaLena EnjelinaNo ratings yet
- ReindersKrijnen2023Interprof IDandmotivationDocument12 pagesReindersKrijnen2023Interprof IDandmotivationsusi adeNo ratings yet
- Ipe and Ipc Assignment Part 1Document17 pagesIpe and Ipc Assignment Part 1api-547401454No ratings yet
- Ways of Knowing As A Framework For Developing Reflective Practice Among Nursing StudentsDocument11 pagesWays of Knowing As A Framework For Developing Reflective Practice Among Nursing StudentsMoonyNo ratings yet
- Different Models of Collaboration Between Nursing Education and (Autosaved)Document13 pagesDifferent Models of Collaboration Between Nursing Education and (Autosaved)Elsy MayjoNo ratings yet
- 17 - Jic - Learning Outcomes For Interprofessional Education 2010 Thistlethwaite and Moran PDFDocument11 pages17 - Jic - Learning Outcomes For Interprofessional Education 2010 Thistlethwaite and Moran PDFRizka ArifahNo ratings yet
- Learning Outcomes For Interprofessional Education (IPE) : Literature Review and SynthesisDocument11 pagesLearning Outcomes For Interprofessional Education (IPE) : Literature Review and SynthesisJane BagaporoNo ratings yet
- Self-Directed and Lifelong LearningDocument10 pagesSelf-Directed and Lifelong LearningZilbran BerontaxNo ratings yet
- 1 s2.0 S2405844020307052 MainDocument4 pages1 s2.0 S2405844020307052 Mainrodriguescatia306992No ratings yet
- 56 239 1 PBDocument11 pages56 239 1 PBahmad acengNo ratings yet
- Social and Healthcare Students Competence in Patient Orie - 2023 - Nurse EducatDocument11 pagesSocial and Healthcare Students Competence in Patient Orie - 2023 - Nurse EducatRonald QuezadaNo ratings yet
- Augmenting Health and Social Care Students’ Clinical Learning Experiences: Outcomes and ProcessesFrom EverandAugmenting Health and Social Care Students’ Clinical Learning Experiences: Outcomes and ProcessesNo ratings yet
- Purposeful Development of Professional Learning Processes: Considerations for Pedagogy, Research and PracticeFrom EverandPurposeful Development of Professional Learning Processes: Considerations for Pedagogy, Research and PracticeNo ratings yet
- CbarDocument11 pagesCbarapi-615586274No ratings yet
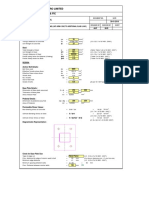
- Design of Base Plate LKP Arm 4-F-30.01.2018Document5 pagesDesign of Base Plate LKP Arm 4-F-30.01.2018HarikrishnaNo ratings yet
- REE AssignmentDocument14 pagesREE AssignmentEmmanNo ratings yet
- Fiber-Optic Cables: Ordering InformationDocument1 pageFiber-Optic Cables: Ordering Information10ahmad yusuf maulanaNo ratings yet
- Drivers' Guide To Use of The Analogue TachographDocument31 pagesDrivers' Guide To Use of The Analogue TachographRomeo LepadatuNo ratings yet
- Objective: Working ExperienceDocument2 pagesObjective: Working ExperienceNitin MahawarNo ratings yet
- Post Test English LanguageDocument3 pagesPost Test English LanguageelvianaNo ratings yet
- Mini Project Report (Edited)Document30 pagesMini Project Report (Edited)Vineeth KRNo ratings yet
- Lesson Plan - Uncle Tom's Cabin - Google SketchDocument2 pagesLesson Plan - Uncle Tom's Cabin - Google SketchErin ThomasNo ratings yet
- PP41 Rev.3Document1 pagePP41 Rev.3Ashish ChackoNo ratings yet
- OSI Data Layer HDLC: High-Level Data Link Control: School of Engineering and Advanced Technology (SEAT)Document30 pagesOSI Data Layer HDLC: High-Level Data Link Control: School of Engineering and Advanced Technology (SEAT)deepika_srivastav_1No ratings yet
- Armstrong Automatic Air Vent ValveDocument2 pagesArmstrong Automatic Air Vent ValveT. LimNo ratings yet
- Delphi 184Document2 pagesDelphi 184Krish MechsterNo ratings yet
- Enactivism and The Nature of Mind Interv PDFDocument11 pagesEnactivism and The Nature of Mind Interv PDFValéria MarquesNo ratings yet
- EagleBurgmann TS4000 enDocument3 pagesEagleBurgmann TS4000 enkeyur1109No ratings yet
- Ystral Mixing Tech. CataloueDocument11 pagesYstral Mixing Tech. Catalouemmk111No ratings yet
- ICCA 2018 Statistics Public AbstractDocument85 pagesICCA 2018 Statistics Public AbstractTatiana RokouNo ratings yet
- Marathi Jungle Bhraman Katha by Padmakar Lad AmravatiDocument15 pagesMarathi Jungle Bhraman Katha by Padmakar Lad Amravatiapi-3777175No ratings yet
- BSP Bio Instruction - RecruitmentDocument2 pagesBSP Bio Instruction - RecruitmentPaolo SantillanNo ratings yet
- E Ticket Pakuan 1Document2 pagesE Ticket Pakuan 1Esha Septian Pesilat KbpcNo ratings yet
- HP Indigo Division Service Instructions 2 Million Imp - Preventive Maintenance GuideDocument18 pagesHP Indigo Division Service Instructions 2 Million Imp - Preventive Maintenance GuideWilliam moreNo ratings yet
- Phloroglucinol TrimethyloroglucinolDocument1 pagePhloroglucinol TrimethyloroglucinolziadddNo ratings yet
- Finite Element Analysis of Circular Annular PlatesDocument9 pagesFinite Element Analysis of Circular Annular PlatesLakshman ReddyNo ratings yet