You might also like
- University Hospitals of Leicester NHS Trust Chart PDFDocument12 pagesUniversity Hospitals of Leicester NHS Trust Chart PDFDesy Purnama100% (1)
- Cheat Sheet 1Document1 pageCheat Sheet 1Rick Frea100% (10)
- NCP - Excess Fluid Volume Related Compromised Regulatory Mechanism (Renal Failure) (Acute Renal Failure)Document3 pagesNCP - Excess Fluid Volume Related Compromised Regulatory Mechanism (Renal Failure) (Acute Renal Failure)Kian Herrera100% (1)
- Scientific Rationale For Dental Implant DesignDocument53 pagesScientific Rationale For Dental Implant DesignM Priya100% (1)
- Blood Coagulation, Anticoagulants, Fibrinolityc & Antithrombotic DrugsDocument10 pagesBlood Coagulation, Anticoagulants, Fibrinolityc & Antithrombotic DrugsVincentius Michael WilliantoNo ratings yet
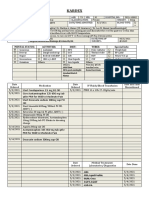
- Kardex: Mental Status: Activities: Diet: Tubes: Special InfoDocument3 pagesKardex: Mental Status: Activities: Diet: Tubes: Special InfoJanelle Cabida SupnadNo ratings yet
- Kardex: Mental Status: Activities: Diet: Tubes: Special InfoDocument3 pagesKardex: Mental Status: Activities: Diet: Tubes: Special InfoJanelle Cabida SupnadNo ratings yet
- Kardex: Mental Status: Activities: Diet: Tubes: Special InfoDocument3 pagesKardex: Mental Status: Activities: Diet: Tubes: Special InfoRyrey Abraham PacamanaNo ratings yet
- Recognized Ho So ListDocument64 pagesRecognized Ho So ListGuru MogaralaNo ratings yet
- 2024BA6844RDocument1 page2024BA6844Rahsanbakhtawar8No ratings yet
- 11062023EL4700RDocument1 page11062023EL4700Rtalibh577No ratings yet
- Venous Thromboprophylaxis After Total Hip Arthroplasty: Aspirin, Warfarin, Enoxaparin, or Factor Xa Inhibitors?Document8 pagesVenous Thromboprophylaxis After Total Hip Arthroplasty: Aspirin, Warfarin, Enoxaparin, or Factor Xa Inhibitors?Dita Putri DamayantiNo ratings yet
- Aiims PDFDocument1 pageAiims PDFRahul RaiNo ratings yet
- 15072022ag0153r PDFDocument1 page15072022ag0153r PDFTahaNo ratings yet
- March 12Document7 pagesMarch 12OB-GYNE DEPARTMENTNo ratings yet
- 13 Districts Recognized Hospitals List PDFDocument86 pages13 Districts Recognized Hospitals List PDFseetha ramNo ratings yet
- L02ifj 19091107234Document1 pageL02ifj 19091107234Muhammad Umar FarooqNo ratings yet
- 17062023AG0258RDocument1 page17062023AG0258RMuniba NasimNo ratings yet
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument1 pageThis Is An Electronic Report & Not: To Be Used For Any Legal PurposesurbeakhanNo ratings yet
- Kim Johnson Kardex To Discharge PlanDocument13 pagesKim Johnson Kardex To Discharge PlanFranz Patrick Legria, CPAC - SNNo ratings yet
- Template Laboratory Request Form - 0Document2 pagesTemplate Laboratory Request Form - 0elmore kakaNo ratings yet
- Hgfyjgf 7 IuDocument2 pagesHgfyjgf 7 IuPavan KumarNo ratings yet
- Laboratory Request Form - SVH: Patient Details Requester DetailsDocument2 pagesLaboratory Request Form - SVH: Patient Details Requester DetailsMahmoud SherifNo ratings yet
- GOS18 Referral Form 1Document2 pagesGOS18 Referral Form 1parvathyNo ratings yet
- SOP-BB-017 - Validation of ABO and Rhesus Blood Grouping SeraDocument7 pagesSOP-BB-017 - Validation of ABO and Rhesus Blood Grouping SeraesaumulimaNo ratings yet
- Blood Transfusion Request FormDocument1 pageBlood Transfusion Request Formshivampal778877No ratings yet
- Physician'S Order/Progress Notes: 23 S. Avila Male JhonDocument2 pagesPhysician'S Order/Progress Notes: 23 S. Avila Male JhonKrizha Angela Nicolas100% (1)
- Touseef Finance ReportDocument1 pageTouseef Finance ReportHaseeb AliNo ratings yet
- Age Related Cerebral Cortical Atrophy Is SeenDocument5 pagesAge Related Cerebral Cortical Atrophy Is SeenTamanash ChowdharyNo ratings yet
- FCVM 10 1263482Document10 pagesFCVM 10 1263482ReywersonNo ratings yet
- Minggu 3 (Medical Terminology)Document51 pagesMinggu 3 (Medical Terminology)Wiwit AndriyaniNo ratings yet
- Kishwar Bibi, Occult BloodDocument1 pageKishwar Bibi, Occult BloodWaqas SaleemNo ratings yet
- Fecalysis SampleDocument1 pageFecalysis SampleReiel PeñaNo ratings yet
- Mediclaim: Karan Jain, Hbe Emp Code: 530024 H.Q. Jaipur Iffco Tokkyo Policy No. 52727509-1-0Document2 pagesMediclaim: Karan Jain, Hbe Emp Code: 530024 H.Q. Jaipur Iffco Tokkyo Policy No. 52727509-1-0Madhusudan DadhichNo ratings yet
- Original Research Paper: PathologyDocument5 pagesOriginal Research Paper: PathologyNurul Huda KowitaNo ratings yet
- Blood Transfusion Policy 6.3Document90 pagesBlood Transfusion Policy 6.3raNo ratings yet
- El-Lab Limited: Test Request FormDocument2 pagesEl-Lab Limited: Test Request FormMannyNo ratings yet
- Adobe Scan 12-Jul-2023Document2 pagesAdobe Scan 12-Jul-2023baibhabnayak20No ratings yet
- Borang Ujian FizikalDocument4 pagesBorang Ujian FizikalAmmar daniel ShahrilNo ratings yet
- Hysterrectomies Information - Ner BlockDocument1 pageHysterrectomies Information - Ner BlockTejas ChuteNo ratings yet
- 22042024CI4184RDocument1 page22042024CI4184Rnauraizsubhan01No ratings yet
- OB Requirements 2020-2021Document6 pagesOB Requirements 2020-2021KIM LORIE YAP PASCUALNo ratings yet
- Docteur Rafiaa Alia: Laboratoire D'Analyses MedicalesDocument6 pagesDocteur Rafiaa Alia: Laboratoire D'Analyses MedicalesazouaouuNo ratings yet
- Hosneara Begum - Aastha ConcentDocument2 pagesHosneara Begum - Aastha ConcentAbul HasnatNo ratings yet
- May 2Document45 pagesMay 2Johanna Hamnia PobleteNo ratings yet
- 17112016CP2144SDocument1 page17112016CP2144SFareed KhanNo ratings yet
- Fnac Results - 31 - 08 - 2023 - 05 - 44 - 51 - AmDocument1 pageFnac Results - 31 - 08 - 2023 - 05 - 44 - 51 - AmClan of comedyNo ratings yet
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument1 pageThis Is An Electronic Report & Not: To Be Used For Any Legal PurposesSalman Fateh AliNo ratings yet
- Template Laboratory Request Form - 0Document2 pagesTemplate Laboratory Request Form - 0Shafiq Azam RumiNo ratings yet
- Laboratory Request Form - TemplateDocument2 pagesLaboratory Request Form - TemplateShafiq Azam RumiNo ratings yet
- KARDEX (Admission)Document1 pageKARDEX (Admission)JA BerzabalNo ratings yet
- 1559211383206-Medical Exam ProformaDocument2 pages1559211383206-Medical Exam ProformaSwatiNo ratings yet
- Jiyo Healthy Jiyo Wellthy Any Time Package: Complete Blood Count (CBC)Document6 pagesJiyo Healthy Jiyo Wellthy Any Time Package: Complete Blood Count (CBC)Lalit VashistaNo ratings yet
- KARDEX (Admission)Document1 pageKARDEX (Admission)JA BerzabalNo ratings yet
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument1 pageThis Is An Electronic Report & Not: To Be Used For Any Legal PurposesHamid PashaNo ratings yet
- Blood Transfusion FormDocument1 pageBlood Transfusion FormFitz Gerald CastilloNo ratings yet
- Gonzales Zosimo AbstractDocument2 pagesGonzales Zosimo AbstractDarnel Jasper HurtadoNo ratings yet
- SHPP.694442 15560863 31102023Document12 pagesSHPP.694442 15560863 31102023Roop TomarNo ratings yet
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument2 pagesThis Is An Electronic Report & Not: To Be Used For Any Legal PurposesanieedanishNo ratings yet
- Template Laboratory Request Form - 0Document1 pageTemplate Laboratory Request Form - 0dawnNo ratings yet
- Win Debate Aboi RanjaneeDocument50 pagesWin Debate Aboi RanjaneeRANJANEE MUTHUNo ratings yet
- Test Request Form - (Name Laboratory) : Patient Details Requester DetailsDocument1 pageTest Request Form - (Name Laboratory) : Patient Details Requester DetailsBilal AbbasNo ratings yet
- Sodium Fluoride PET/CT in Clinical UseFrom EverandSodium Fluoride PET/CT in Clinical UseKalevi KairemoNo ratings yet
- RFP For Legal ServicesDocument7 pagesRFP For Legal ServicesWartan WuNo ratings yet
- Ex Parte Schulhauser 2016 - 04 - 28Document22 pagesEx Parte Schulhauser 2016 - 04 - 28Wartan WuNo ratings yet
- New Jersey Manual On Style FOR Judicial OpinionsDocument30 pagesNew Jersey Manual On Style FOR Judicial OpinionsWartan WuNo ratings yet
- House Resolution No. 103Document4 pagesHouse Resolution No. 103Wartan WuNo ratings yet
- Hours of Sleep Chart: Hours Slept Times Date Interruptions NotesDocument1 pageHours of Sleep Chart: Hours Slept Times Date Interruptions NotesWartan WuNo ratings yet
- Cold Flu Tracker PDFDocument1 pageCold Flu Tracker PDFWartan WuNo ratings yet
- SGH How To Approach SBAsDocument49 pagesSGH How To Approach SBAsArnav RaiNo ratings yet
- 358 Muhammad Zul SikkDocument3 pages358 Muhammad Zul SikkMar Yana MamehNo ratings yet
- History TakingDocument28 pagesHistory TakingHemantNo ratings yet
- INTRODUCTIONDocument2 pagesINTRODUCTIONEldonVinceIsidroNo ratings yet
- BSP-Medical FormDocument1 pageBSP-Medical FormNyleg Aicilag100% (2)
- Daily Consumption of Growing-Up Milk Is Associated With Less Stunting Among Indonesian ToddlersDocument7 pagesDaily Consumption of Growing-Up Milk Is Associated With Less Stunting Among Indonesian ToddlersAnugerah DestiaNo ratings yet
- Chest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryDocument5 pagesChest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryGopi KrishnanNo ratings yet
- Function and Importance of The Cardiovascular SystemDocument3 pagesFunction and Importance of The Cardiovascular SystemBenjamin SmithNo ratings yet
- Effects of Luminance and Illuminance OnDocument8 pagesEffects of Luminance and Illuminance Onpatricia nhavotoNo ratings yet
- The Combination of Lemon Grass (Cymbopogon Citratus) and Garlic Extract (AlliumDocument49 pagesThe Combination of Lemon Grass (Cymbopogon Citratus) and Garlic Extract (AlliumysaaaNo ratings yet
- Defining Mental Illness' in Mental Health PolicyDocument13 pagesDefining Mental Illness' in Mental Health PolicyMohammad AfiefNo ratings yet
- PDF Nutrition CM 3 CU 11 LAB WEEK 13Document6 pagesPDF Nutrition CM 3 CU 11 LAB WEEK 13Chezer KiethNo ratings yet
- 5 - Farmakoterapi Pediatri - Dr. Nanang MunifDocument45 pages5 - Farmakoterapi Pediatri - Dr. Nanang MunifEdzhar Hasiholan100% (1)
- Abnormal Bowel Gas PatternDocument136 pagesAbnormal Bowel Gas PatternEdward ElricNo ratings yet
- The Meanings of Craft To An OTDocument10 pagesThe Meanings of Craft To An OTAriadne de PaulaNo ratings yet
- COVID ChildCareProgram Flowchart HDocument2 pagesCOVID ChildCareProgram Flowchart HRosefel DumapeNo ratings yet
- Graphites 01 PDFDocument3 pagesGraphites 01 PDFASLAMNo ratings yet
- JobadDocument1 pageJobadapi-344276587No ratings yet
- The Benefits of Pets For Human Health: Psychology and Behavioral ScienceDocument3 pagesThe Benefits of Pets For Human Health: Psychology and Behavioral ScienceEden Ben HamoNo ratings yet
- Multidimensional Schizotypy Scale Manual v28Document22 pagesMultidimensional Schizotypy Scale Manual v28asdasNo ratings yet
- Daftar Pustaka - 2Document6 pagesDaftar Pustaka - 2Rafi PutraNo ratings yet
- Material Safety AvabiomodDocument4 pagesMaterial Safety Avabiomodfs1640No ratings yet
- RAPPLER - Ferrer Ferrer and Emmanuel - Incineration of Coronavirus Wastes Will Worsen The SituationDocument5 pagesRAPPLER - Ferrer Ferrer and Emmanuel - Incineration of Coronavirus Wastes Will Worsen The SituationRolando E. CaserNo ratings yet
- Katie Nelson PDFDocument3 pagesKatie Nelson PDFKatie NNo ratings yet
- Activity 2 Nervous SystemDocument2 pagesActivity 2 Nervous SystemElaine BaratitaNo ratings yet
- Teen Social Media Use May Increase Risk of Mental Health ProblemsDocument3 pagesTeen Social Media Use May Increase Risk of Mental Health ProblemsThenaNo ratings yet
- Dentistry 11 00079Document19 pagesDentistry 11 00079maroun ghalebNo ratings yet