You might also like
- MAKING DMT GUIDE: The essential guide to master the art of making DMT the spirit molecule at home in a simplified wayFrom EverandMAKING DMT GUIDE: The essential guide to master the art of making DMT the spirit molecule at home in a simplified wayNo ratings yet
- Antipsychotics 1Document41 pagesAntipsychotics 1fahad rustam100% (1)
- DrUG STUDY PSYCHEDocument52 pagesDrUG STUDY PSYCHELiza MPNo ratings yet
- Anti PsychoticDocument38 pagesAnti PsychoticAsep Cece IrhamNo ratings yet
- Systemic PharmacologyDocument37 pagesSystemic PharmacologyMoNiruzzaman MoNirNo ratings yet
- Psychopharmacology in Psychopharmacology in Psychiatry PsychiatryDocument16 pagesPsychopharmacology in Psychopharmacology in Psychiatry PsychiatryHasnain HyderNo ratings yet
- PsychopharmacologyDocument50 pagesPsychopharmacologyapi-3703352No ratings yet
- Syllabus Pharmaceuticals Related Neurotoxicity C16 Kumar April 22 Sat 2023 AANDocument59 pagesSyllabus Pharmaceuticals Related Neurotoxicity C16 Kumar April 22 Sat 2023 AANJere AyerbeNo ratings yet
- AntipsychoticsDocument51 pagesAntipsychoticsShailja SharmaNo ratings yet
- Beers Criteria HandoutDocument3 pagesBeers Criteria Handoutapi-647779956No ratings yet
- CC Rubie Ann G. Tillor: IM: (Schizophrenia)Document11 pagesCC Rubie Ann G. Tillor: IM: (Schizophrenia)Rubie Ann TillorNo ratings yet
- Dug Study PsycheDocument33 pagesDug Study PsycheAziil LiizaNo ratings yet
- Topic 2 - TREATMENT OF MENTAL DISEASESDocument52 pagesTopic 2 - TREATMENT OF MENTAL DISEASESprashant singhNo ratings yet
- Drug StudyDocument4 pagesDrug StudyJessica GlitterNo ratings yet
- Antipsychotics - AMBOSS PDFDocument7 pagesAntipsychotics - AMBOSS PDFOpio Isaac100% (1)
- SchizopDocument43 pagesSchizopapi-548578435No ratings yet
- Antipsychotics: Mary A. Wittler and Eric J. LavonasDocument5 pagesAntipsychotics: Mary A. Wittler and Eric J. LavonasSNo ratings yet
- PsychiatryDocument5 pagesPsychiatryJohn SmithNo ratings yet
- Antipsychotic MedicationDocument3 pagesAntipsychotic MedicationMichelle Angela CerezoNo ratings yet
- Antipsychotic Drugs: Key Terms Chapter ObjectivesDocument10 pagesAntipsychotic Drugs: Key Terms Chapter ObjectivesChelzie LasernaNo ratings yet
- Mesoridazine Drug StudyDocument5 pagesMesoridazine Drug Studyshadow gonzalezNo ratings yet
- Drugs For Psyciatric DisordersDocument19 pagesDrugs For Psyciatric Disordersapi-36993610% (1)
- NPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesDocument83 pagesNPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesValeria AcevedoNo ratings yet
- Effectiveness Indicated by A Reduction in Psychotic BehaviorDocument4 pagesEffectiveness Indicated by A Reduction in Psychotic BehaviorGwyn RosalesNo ratings yet
- Year 2 Drug ListDocument8 pagesYear 2 Drug ListRay100% (1)
- Extra Pyramidal Symptoms AdvanceDocument5 pagesExtra Pyramidal Symptoms AdvanceMr. Psycho Sam100% (1)
- Biological Treatments in PsychiatryDocument56 pagesBiological Treatments in PsychiatryNurul AfzaNo ratings yet
- Of Drug Toxicities Psychiatric Emergencies & Medication Side EffectsDocument8 pagesOf Drug Toxicities Psychiatric Emergencies & Medication Side EffectsBaraa KhalafNo ratings yet
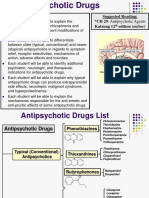
- Antipsychotic Present and FutureDocument34 pagesAntipsychotic Present and FuturepabitraNo ratings yet
- Anti PsychoticsDocument34 pagesAnti Psychotics88AKKNo ratings yet
- AntipsychoticsDocument29 pagesAntipsychoticsTyler Lawrence Coye100% (5)
- Psychopamacology PresentationDocument131 pagesPsychopamacology Presentationsalmalissu0No ratings yet
- Penyalahgunaan ObatDocument26 pagesPenyalahgunaan Obatvinna iasyaNo ratings yet
- PsychopharmacologyDocument77 pagesPsychopharmacologychachaazkaNo ratings yet
- Antidepressant DrugsDocument47 pagesAntidepressant DrugsOjambo Flavia100% (3)
- Drug StudyDocument10 pagesDrug StudyRubie Ann TillorNo ratings yet
- Drugs W/ Important Action On Smooth Muscle (Autacoids)Document3 pagesDrugs W/ Important Action On Smooth Muscle (Autacoids)Liezel Dejumo Bartolata100% (1)
- Antipsychotic Drugs - Pharmacology - An Illustrated ReviewDocument5 pagesAntipsychotic Drugs - Pharmacology - An Illustrated ReviewDragutin PetrićNo ratings yet
- Antipsychotic or Neuroleptic DrugsDocument12 pagesAntipsychotic or Neuroleptic Drugscamile buhanginNo ratings yet
- NCM 106 NarcoticsDocument25 pagesNCM 106 NarcoticsMelchizedek Tagarino TorioNo ratings yet
- NCM 106 NarcoticsDocument25 pagesNCM 106 NarcoticsMelchizedek Tagarino TorioNo ratings yet
- DRUG STUDY - BSN III Center For Behavioral Sciences: Generic Name: Psychosis Adult: PO Adverse Effects CNS:ExtrapyramidalDocument10 pagesDRUG STUDY - BSN III Center For Behavioral Sciences: Generic Name: Psychosis Adult: PO Adverse Effects CNS:ExtrapyramidalChris Denver BancaleNo ratings yet
- DRUG STUDY - BSN III Center For Behavioral Sciences: Generic Name: Psychosis Adult: PO Adverse Effects CNS:ExtrapyramidalDocument7 pagesDRUG STUDY - BSN III Center For Behavioral Sciences: Generic Name: Psychosis Adult: PO Adverse Effects CNS:ExtrapyramidalChris Denver BancaleNo ratings yet
- Agents Used For Schizophrenia (Antipsychotic) : Novita CaroliaDocument17 pagesAgents Used For Schizophrenia (Antipsychotic) : Novita CaroliaDetty NoviantyNo ratings yet
- Psychopharma 1Document7 pagesPsychopharma 1Mitchee Zialcita100% (1)
- AMITRIPTYLINEDocument1 pageAMITRIPTYLINERicky Ramos Jr.No ratings yet
- HaloperidolDocument4 pagesHaloperidolKyla Barrera TabungarNo ratings yet
- Haloperidol PDFDocument4 pagesHaloperidol PDFfatimahNo ratings yet
- Dr. Andy Tampubolon, SPS - Management of Diabetic NeuropathyDocument26 pagesDr. Andy Tampubolon, SPS - Management of Diabetic NeuropathyAthalia TalawayNo ratings yet
- Drug StudyDocument10 pagesDrug Studyrubie ann tillorNo ratings yet
- Drug Study (Haloperidol)Document3 pagesDrug Study (Haloperidol)Mae Ann Bueno CastillonNo ratings yet
- An Tide Pres AnDocument3 pagesAn Tide Pres AnPatricia MinickNo ratings yet
- Serba Serbi Neuroleptik Masa KiniDocument59 pagesSerba Serbi Neuroleptik Masa Kinikoas jiwa ragaNo ratings yet
- Drug Study: TramadolDocument6 pagesDrug Study: TramadolShara Lailanie A. AzisNo ratings yet
- Lecture 4, Antipsychotics, AntidepressantsDocument94 pagesLecture 4, Antipsychotics, Antidepressantsj.doe.hex_87100% (3)
- Bait-It Zennesah Carmelle - CP Activity 24 Medication ReconciliationDocument4 pagesBait-It Zennesah Carmelle - CP Activity 24 Medication ReconciliationBait-it Zennesah CarmelleNo ratings yet
- Mental Health and Psychiatric Nursing: Vernalin B. Terrado, RNDocument35 pagesMental Health and Psychiatric Nursing: Vernalin B. Terrado, RNverna100% (1)
- AntidepressantsDocument4 pagesAntidepressantsGrace CabilloNo ratings yet
- GG Mental Dan Perilaku Akibat Alkohol &zat Psikoaktif LainnyaDocument125 pagesGG Mental Dan Perilaku Akibat Alkohol &zat Psikoaktif Lainnya326449No ratings yet
- Drug StudyDocument4 pagesDrug Studyshiela marie cortezNo ratings yet
- Febuxostat Vs AlopurinolDocument13 pagesFebuxostat Vs AlopurinolNilson Morales CordobaNo ratings yet
- Cardiorenal SyndromeDocument39 pagesCardiorenal SyndromeitalofgNo ratings yet
- Default PDFDocument29 pagesDefault PDFNilson Morales CordobaNo ratings yet
- Risk Factor For Sever Postpartum Hemorrhage A Case Control StudyDocument9 pagesRisk Factor For Sever Postpartum Hemorrhage A Case Control StudyAhmad SyaukatNo ratings yet
- Default PDFDocument29 pagesDefault PDFNilson Morales CordobaNo ratings yet
- Default PDFDocument29 pagesDefault PDFNilson Morales CordobaNo ratings yet
- Accuracy of Blood-Glucose Measurements Using GlucoDocument14 pagesAccuracy of Blood-Glucose Measurements Using GlucoNilson Morales CordobaNo ratings yet
- Ecocardiograma para Guiar Reanimacion PDFDocument7 pagesEcocardiograma para Guiar Reanimacion PDFJose santos MembreñoNo ratings yet
- AS6964381116129281543055193345 Content 1Document12 pagesAS6964381116129281543055193345 Content 1César Enrique Rojas LópezNo ratings yet
- Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19) A ReviewDocument13 pagesPathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19) A ReviewJose de Jesus Ayala LeyvaNo ratings yet
- 30794136: Aspiration Pneumonia in Older AdultsDocument7 pages30794136: Aspiration Pneumonia in Older AdultsNilson Morales CordobaNo ratings yet
- COMMIT ClopidogrelDocument15 pagesCOMMIT ClopidogrelCristina PazmiñoNo ratings yet
- Crite RiosDocument8 pagesCrite RiosNilson Morales CordobaNo ratings yet
- Update: Lipid Guidelines: Do Not Burn The CookiesDocument50 pagesUpdate: Lipid Guidelines: Do Not Burn The CookiesNilson Morales CordobaNo ratings yet
- 26989182: Diabetic Ketoacidosis With Canagliflozin, A Sodium-Glucose Cotransporter 2 Inhibitor, in Patients With Type 1 DiabetesDocument7 pages26989182: Diabetic Ketoacidosis With Canagliflozin, A Sodium-Glucose Cotransporter 2 Inhibitor, in Patients With Type 1 DiabetesNilson Morales CordobaNo ratings yet
- Standards Ofmedical Care in Diabetesd2018Document2 pagesStandards Ofmedical Care in Diabetesd2018Pitchya WangmeesriNo ratings yet
- Phobia ListDocument3 pagesPhobia ListAun NaqviNo ratings yet
- Soap NoteDocument9 pagesSoap NoteHusaini83% (6)
- Cognitive Behavior Therapy For Generalized Social Anxiety DisorderDocument11 pagesCognitive Behavior Therapy For Generalized Social Anxiety DisorderZsuzsa BoscaNo ratings yet
- Medical Diagnostic Centre-10lDocument17 pagesMedical Diagnostic Centre-10lRENUSREE ENTERPRISES100% (1)
- Autism - Gender and GeneticsDocument12 pagesAutism - Gender and GeneticsAggrey SmartfieldNo ratings yet
- Dimensional Models of Personality DisordersDocument316 pagesDimensional Models of Personality Disorderseva pravitasari nefertiti100% (1)
- A Comparative Study Machine Learning Algorithms For Parkinson's Disease AnalysisDocument12 pagesA Comparative Study Machine Learning Algorithms For Parkinson's Disease AnalysisIJRASETPublicationsNo ratings yet
- List of Psychological DisordersDocument12 pagesList of Psychological DisordersClaire TeoxonNo ratings yet
- L4 Chapter 4 Mood DisordersDocument9 pagesL4 Chapter 4 Mood DisordersHui Li TehNo ratings yet
- Brochure 201516 MBCHB AdmissionsDocument21 pagesBrochure 201516 MBCHB Admissionsaxn0241No ratings yet
- Lecture Notes On EpidemiologyDocument196 pagesLecture Notes On Epidemiologypushpa devkota100% (1)
- Psychogenic Nonepileptic Seizures - Management and Prognosis - UpToDateDocument18 pagesPsychogenic Nonepileptic Seizures - Management and Prognosis - UpToDateAndré MendonçaNo ratings yet
- Diagnosis of Vascular Cognitive ImpairmentDocument17 pagesDiagnosis of Vascular Cognitive ImpairmentInes Strenja LinićNo ratings yet
- Sma22 Cs-3d-Imaging Ug Ed-04 English enDocument182 pagesSma22 Cs-3d-Imaging Ug Ed-04 English enDorel ManNo ratings yet
- Aspergers PowerPointDocument10 pagesAspergers PowerPointAmmutha SokayahNo ratings yet
- Personality Belief Questionnaire Scoring KeyDocument1 pagePersonality Belief Questionnaire Scoring KeyKrystal100% (1)
- hs200 - 04 0904b Term SyllabusDocument13 pageshs200 - 04 0904b Term Syllabuscindyfuller68No ratings yet
- Anxiety DisordersDocument9 pagesAnxiety DisordersShara SampangNo ratings yet
- Whole MagDocument132 pagesWhole MagshemagononlyNo ratings yet
- Medical Supplies and Equipment For Primary Health Care. A Practical Resource For Procurement and Management PDFDocument192 pagesMedical Supplies and Equipment For Primary Health Care. A Practical Resource For Procurement and Management PDFMandela KibiritiNo ratings yet
- Bipolar NCPDocument4 pagesBipolar NCPcandy19agustin100% (1)
- Every Patient Tells A Story: Medical Mysteries and The Art of Diagnosis - Lisa SandersDocument5 pagesEvery Patient Tells A Story: Medical Mysteries and The Art of Diagnosis - Lisa Sandersdegyxuby0% (1)
- Module 1 - Introduction To Health AssessmentDocument6 pagesModule 1 - Introduction To Health AssessmentJehssa Jee SarmientoNo ratings yet
- Guide Olympus2009Document36 pagesGuide Olympus2009Carlos RamirezNo ratings yet
- First-Generation Versus Second-Generation Antipsychotics in Adults: Comparative EffectivenessDocument4 pagesFirst-Generation Versus Second-Generation Antipsychotics in Adults: Comparative EffectivenessAbdullah ZuhairNo ratings yet
- An Atlas of Cast Gold ProceduresDocument270 pagesAn Atlas of Cast Gold ProceduresBotoc BeatriceNo ratings yet
- CAT Diagnosis FormDocument2 pagesCAT Diagnosis FormVictoria Perreault QuattrucciNo ratings yet
- Malaria Parasite Detection Using Image ProcessingDocument5 pagesMalaria Parasite Detection Using Image Processingsimha srivatsaNo ratings yet
- Module 1: Health AssessmentDocument16 pagesModule 1: Health AssessmentAmberNo ratings yet
- Bipolar DisorderDocument30 pagesBipolar Disorderapi-401906698No ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)