You might also like
- Check Unit 557 Jan-Feb Genetics v3 PDFDocument36 pagesCheck Unit 557 Jan-Feb Genetics v3 PDFdragon66No ratings yet
- Intensive Nursing Practicum: SchizophreniaDocument44 pagesIntensive Nursing Practicum: SchizophreniaAngelicaNo ratings yet
- Acute Urinary ObstructionDocument34 pagesAcute Urinary ObstructionHafizur RashidNo ratings yet
- Major Depressive Disorder PDFDocument22 pagesMajor Depressive Disorder PDFapi-545811586No ratings yet
- Leg UlcerDocument28 pagesLeg UlcerRanindya PutriNo ratings yet
- Ophthalmology - Passmedicine 2012 - 62013146Document18 pagesOphthalmology - Passmedicine 2012 - 62013146abuahmed&janaNo ratings yet
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Congenital Heart Disease 1Document14 pagesCongenital Heart Disease 1OzzeyNo ratings yet
- VASCULITIS: AN OVERVIEW OF DIAGNOSIS AND MANAGEMENTDocument79 pagesVASCULITIS: AN OVERVIEW OF DIAGNOSIS AND MANAGEMENTSol CamusNo ratings yet
- DD ScrotumDocument4 pagesDD ScrotumAy HaanNo ratings yet
- Musculoskeletal: Unit 553 September 2018Document34 pagesMusculoskeletal: Unit 553 September 2018dragon66No ratings yet
- Acute Renal FailureDocument5 pagesAcute Renal FailureSalman KhanNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Dyspnea, (Breathlessness) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDyspnea, (Breathlessness) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionFrom EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionNo ratings yet
- 6675 Final ExamDocument32 pages6675 Final ExamtroillerdrippyNo ratings yet
- Pathy's Principles and Practice of Geriatric MedicineFrom EverandPathy's Principles and Practice of Geriatric MedicineAlan J. SinclairNo ratings yet
- Anterior Pituitary Gland: Fawwaz Ammari Laith & HaniDocument22 pagesAnterior Pituitary Gland: Fawwaz Ammari Laith & HaniRashed ShatnawiNo ratings yet
- Disorders of Motility2Document46 pagesDisorders of Motility2valdomiroNo ratings yet
- Antipsychotic Deprescribing Algorithm PDFDocument2 pagesAntipsychotic Deprescribing Algorithm PDFFitri Amelia RizkiNo ratings yet
- Shock, Sirs & ModsDocument37 pagesShock, Sirs & ModsambitioustamannaNo ratings yet
- Clinical Skills Handbook 2015 MEDN40060 2Document66 pagesClinical Skills Handbook 2015 MEDN40060 2Wilson KhawNo ratings yet
- USMLE Step 2 CK Notes on Neurology and Neurological ConditionsDocument5 pagesUSMLE Step 2 CK Notes on Neurology and Neurological ConditionsLoyla RoseNo ratings yet
- Critical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeFrom EverandCritical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeNo ratings yet
- Medad Andrology Special Note NMT13 PDFDocument70 pagesMedad Andrology Special Note NMT13 PDFSelim TarekNo ratings yet
- Impact of High Sensitivity Troponins For 6nov Cardiac ForumDocument39 pagesImpact of High Sensitivity Troponins For 6nov Cardiac Forummouna6685No ratings yet
- Acromegaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAcromegaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Vasculitis: Disorder Vessels Pathology Presentation Test TX OtherDocument3 pagesVasculitis: Disorder Vessels Pathology Presentation Test TX OthermcwnotesNo ratings yet
- Treatment and Classification of Heart FailureDocument2 pagesTreatment and Classification of Heart FailureShannon RamsumairNo ratings yet
- Primary Care Antibiotic Guideline FINAL May 2015Document10 pagesPrimary Care Antibiotic Guideline FINAL May 2015Atta Muhammad MemonNo ratings yet
- Pro32 SupraventricularTachycardiaDocument1 pagePro32 SupraventricularTachycardiaRonald KendallNo ratings yet
- Psychosis ThesisDocument19 pagesPsychosis ThesisjustoneoftheguysNo ratings yet
- Pulmonary Arterial Hypertension in Congenital Heart Disease: Eisenmenger’s Syndrome - A Global PerspectiveFrom EverandPulmonary Arterial Hypertension in Congenital Heart Disease: Eisenmenger’s Syndrome - A Global PerspectiveNo ratings yet
- REVISED-Med TaperingDocument3 pagesREVISED-Med TaperingDwi HerawatiNo ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Cardiology Guide: Key Concepts, Formulas and Treatment StrategiesDocument5 pagesCardiology Guide: Key Concepts, Formulas and Treatment StrategiesRodrigo FonsecaNo ratings yet
- Pharm Fall Cardiovascular Pharmacology Study Guide-106Document47 pagesPharm Fall Cardiovascular Pharmacology Study Guide-106sean liyanageNo ratings yet
- Management of Diabetes Ketoacidosis in PregnancyDocument19 pagesManagement of Diabetes Ketoacidosis in PregnancySudhir PaulNo ratings yet
- Coronary Artery Disease Cad2Document182 pagesCoronary Artery Disease Cad2Mamot MotNo ratings yet
- Pharmacologic TX For Idiopathic Parkinsons: Strategy Class / Drug MOA Side Effects USEDocument2 pagesPharmacologic TX For Idiopathic Parkinsons: Strategy Class / Drug MOA Side Effects USEnicdeepNo ratings yet
- Von Willebrand Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandVon Willebrand Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DDocument28 pagesAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaNo ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
- Faria Chaudhry - CVDocument9 pagesFaria Chaudhry - CVapi-548578435No ratings yet
- Teaching Experience Log - FariaDocument3 pagesTeaching Experience Log - Fariaapi-548578435No ratings yet
- Teaching Manual - FariaDocument7 pagesTeaching Manual - Fariaapi-548578435No ratings yet
- Iptec Preceptor FeedbackDocument2 pagesIptec Preceptor Feedbackapi-548578435No ratings yet
- MidpointDocument4 pagesMidpointapi-548578435No ratings yet
- Podiatry ScheduleDocument2 pagesPodiatry Scheduleapi-548578435No ratings yet
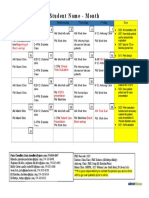
- Example Student CalendarDocument1 pageExample Student Calendarapi-548578435No ratings yet
- Updated 2020 Purdue Am Care Lecture Updated 2Document31 pagesUpdated 2020 Purdue Am Care Lecture Updated 2api-548578435No ratings yet
- Seizure ReflectionDocument1 pageSeizure Reflectionapi-548578435No ratings yet
- Id ReflectionDocument1 pageId Reflectionapi-548578435No ratings yet
- Preventative Health ReflectionDocument2 pagesPreventative Health Reflectionapi-548578435No ratings yet
- Ambulatory Care ReflectionDocument1 pageAmbulatory Care Reflectionapi-548578435No ratings yet
- Final Public Health Awv Lecture - 4Document58 pagesFinal Public Health Awv Lecture - 4api-548578435No ratings yet
- Id 2Document39 pagesId 2api-548578435No ratings yet
- New Seizures - Faria ChaudhryDocument50 pagesNew Seizures - Faria Chaudhryapi-548578435No ratings yet
- Sample SOP Pharmacy ChemistryDocument3 pagesSample SOP Pharmacy ChemistryPrawin Kumar100% (1)
- Antifungal DrugsDocument45 pagesAntifungal DrugsAbdulai WakoNo ratings yet
- Med Thera 1.1 Rational Drug Use and Prescription Writing ExercisesDocument6 pagesMed Thera 1.1 Rational Drug Use and Prescription Writing ExercisesZazaNo ratings yet
- Cleaning Validation StandardDocument20 pagesCleaning Validation StandardAndy RojasNo ratings yet
- Vigorin Gold CapsuleDocument3 pagesVigorin Gold Capsulehk_scribd100% (1)
- Bravecto 3 MonthsDocument3 pagesBravecto 3 MonthsDerrick LimNo ratings yet
- Daftar Harga Obat Asuransi 24Document23 pagesDaftar Harga Obat Asuransi 24Widu Jalak SlpNo ratings yet
- Puskesmas: Modo Kecamatan: Bukal Kab/Kota: Buol Propinsi: Sulawesi Tengah Bulan: JanuariDocument42 pagesPuskesmas: Modo Kecamatan: Bukal Kab/Kota: Buol Propinsi: Sulawesi Tengah Bulan: JanuariFransiskaNo ratings yet
- Abstract Comparison Between Albendazole and MebendazoleDocument25 pagesAbstract Comparison Between Albendazole and MebendazoleluzNo ratings yet
- Why Biocon has achieved success as India's largest biotech companyDocument12 pagesWhy Biocon has achieved success as India's largest biotech companyVipul KhemkaNo ratings yet
- AnnexG eKAS&ePresSDocument2 pagesAnnexG eKAS&ePresSLaish Christle CapiendoNo ratings yet
- Spravato For Treatment Resistant DepressionDocument7 pagesSpravato For Treatment Resistant DepressionRobert ChambersNo ratings yet
- Professor List China For PharmacyDocument13 pagesProfessor List China For Pharmacyadil yousafNo ratings yet
- Brenner Adjustment DoseDocument34 pagesBrenner Adjustment Dosecygnus112No ratings yet
- CIPHIDocument256 pagesCIPHIसदानंद देशपांडेNo ratings yet
- Pharmaceutical Orgainc Chemistry I (PHA110) - Lab Report FormatDocument3 pagesPharmaceutical Orgainc Chemistry I (PHA110) - Lab Report Formataya benshiNo ratings yet
- Anti-Fungal Drugs Guide for Mycosis TreatmentDocument6 pagesAnti-Fungal Drugs Guide for Mycosis Treatmentbilal ahmadNo ratings yet
- Triazole Antifungal Therapeutic Drug Monitoring: ECIL 6 MeetingDocument76 pagesTriazole Antifungal Therapeutic Drug Monitoring: ECIL 6 MeetingBengt HörbergNo ratings yet
- List Obat Dr. Daniel RantetondokDocument3 pagesList Obat Dr. Daniel RantetondokBudhi KaromaNo ratings yet
- Reporte de Lista de Precios de Productos de Drogueria Vitacore, C.ADocument2 pagesReporte de Lista de Precios de Productos de Drogueria Vitacore, C.ALaura PeñaNo ratings yet
- Executive Office Street Drug Slang ReferenceDocument38 pagesExecutive Office Street Drug Slang ReferenceChae No100% (1)
- Drug Study: Diphenhydramine IVDocument6 pagesDrug Study: Diphenhydramine IVMarson RosaritoNo ratings yet
- Dosage Form - WikipediaDocument4 pagesDosage Form - WikipediaMohamed IbrahimNo ratings yet
- Pharmacology of Disopyramide: Yosephine A. H. 020100058Document20 pagesPharmacology of Disopyramide: Yosephine A. H. 020100058zulfantri1983No ratings yet
- DSTC 1586861258Document139 pagesDSTC 1586861258Manjeet Thakur100% (2)
- Inidivor Indictment - Returned 2019-04-09 RedactedDocument47 pagesInidivor Indictment - Returned 2019-04-09 RedactedWCYBDigitalNo ratings yet
- Aduro ADocument17 pagesAduro AEvelyn AssahNo ratings yet
- Biosimilar Development - An Overview: Correspondence ToDocument8 pagesBiosimilar Development - An Overview: Correspondence ToAjay IyerNo ratings yet
- ZDocument3 pagesZBenjamin TantiansuNo ratings yet
- Anjali (1915)Document16 pagesAnjali (1915)vikasNo ratings yet