You might also like
- Hasanbeigi Et AlDocument4 pagesHasanbeigi Et AlAhmad BukhariNo ratings yet
- 11 3854Document4 pages11 3854Yao RaNo ratings yet
- Preserving Efficacy of Chloramphenicol Against Typhoid Fever in A Tertiary Care Hospital, IndiaDocument5 pagesPreserving Efficacy of Chloramphenicol Against Typhoid Fever in A Tertiary Care Hospital, IndiaMelaniNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleAliyu labboNo ratings yet
- Epidemiology of Typhoid and Paratyphoid Fever in Kathmandu: Two Years Study and Trends of Antimicrobial ResistanceDocument5 pagesEpidemiology of Typhoid and Paratyphoid Fever in Kathmandu: Two Years Study and Trends of Antimicrobial ResistanceBerriFebriantoNo ratings yet
- BBRC Vol 14 No 04 2021-78Document4 pagesBBRC Vol 14 No 04 2021-78Dr Sharique AliNo ratings yet
- 32 Vol. 7 Issue 9 September 2016 IJPSR RA 6515Document5 pages32 Vol. 7 Issue 9 September 2016 IJPSR RA 6515Monyet...No ratings yet
- 5 SudharshanDocument5 pages5 SudharshaneditorijmrhsNo ratings yet
- Entericfever 201810061138061823280Document4 pagesEntericfever 201810061138061823280Cindy HerwitiNo ratings yet
- PsikosisDocument6 pagesPsikosisRizki UtamiNo ratings yet
- Typhoid FeverDocument6 pagesTyphoid FeverReeshabhdev GauttamNo ratings yet
- TRT2015 215015Document10 pagesTRT2015 215015faustinaNo ratings yet
- Diagnosis and Treatment of Human Salmonellosis inDocument8 pagesDiagnosis and Treatment of Human Salmonellosis inRajihaNo ratings yet
- 282 F 4 e 2 Edaf 124 A 0Document12 pages282 F 4 e 2 Edaf 124 A 0Mazin AlmaziniNo ratings yet
- Cross Sectional Study On Antibiotic Resistance Pattern of Almonella Typhi Clinical Isolates From AngladeshDocument6 pagesCross Sectional Study On Antibiotic Resistance Pattern of Almonella Typhi Clinical Isolates From AngladeshStella AngelicaNo ratings yet
- Multiple-Antibiotic Resistance Mediated by Plasmids and Integrons in Uropathogenic Escherichia Coli and Klebsiella PneumoniaeDocument5 pagesMultiple-Antibiotic Resistance Mediated by Plasmids and Integrons in Uropathogenic Escherichia Coli and Klebsiella PneumoniaeProbioticsAnywhereNo ratings yet
- Cegielski, Levo Vs Moxi 3Document13 pagesCegielski, Levo Vs Moxi 3hasan andrianNo ratings yet
- Research Article Salmonella From Human And: Molecular Characterization of Animal Origins in UgandaDocument10 pagesResearch Article Salmonella From Human And: Molecular Characterization of Animal Origins in UgandaGrclla McnonhengNo ratings yet
- Spectrum of Dysentery in Children Presenting To A Tertiary Level Teaching Hospital in New DelhiDocument5 pagesSpectrum of Dysentery in Children Presenting To A Tertiary Level Teaching Hospital in New DelhiNasNo ratings yet
- Drug Resistance Patterns in Comorbid and Non-Comorbid Relapsed TB CasesDocument8 pagesDrug Resistance Patterns in Comorbid and Non-Comorbid Relapsed TB Casesaang kunaifi adityaNo ratings yet
- 16 4170okeDocument4 pages16 4170okeFenni OktoberryNo ratings yet
- Pone 0198080Document15 pagesPone 0198080kornelis aribowoNo ratings yet
- Natural Products As Soruce of Dengue AntiviralsDocument26 pagesNatural Products As Soruce of Dengue AntiviralsKaren SánchezNo ratings yet
- HJNHNNDocument9 pagesHJNHNNProbioticsAnywhereNo ratings yet
- 32 JMSCRDocument6 pages32 JMSCRseanNo ratings yet
- Pattern of Antimicrobial Drug Resistance of Salmonella Typhi and Paratyphi A in A Teaching Hospital in IslamabadDocument5 pagesPattern of Antimicrobial Drug Resistance of Salmonella Typhi and Paratyphi A in A Teaching Hospital in IslamabadDevita RamadaniNo ratings yet
- The Rationality of Antibiotics Therapy Toward Children With Typhoid Fever at M.M. Dunda HospitalDocument4 pagesThe Rationality of Antibiotics Therapy Toward Children With Typhoid Fever at M.M. Dunda HospitalaisyahNo ratings yet
- Demam TyfoidDocument6 pagesDemam Tyfoidseptia mutiaraNo ratings yet
- Salmonellosis Research PaperDocument5 pagesSalmonellosis Research PaperxkcwaaqlgNo ratings yet
- Article PDFDocument8 pagesArticle PDFSipkhotunWindayaniNo ratings yet
- Masyeni S Et Al 2018 - Antimicrobial Susceptibility Pattern of Pathogens Isolated From Various Specimens in Denpasar-BaliDocument10 pagesMasyeni S Et Al 2018 - Antimicrobial Susceptibility Pattern of Pathogens Isolated From Various Specimens in Denpasar-BaliGilbert LazarusNo ratings yet
- Atencio Azucena Besares Special ProblemDocument18 pagesAtencio Azucena Besares Special ProblemShane Catherine BesaresNo ratings yet
- Cjim 7 114Document6 pagesCjim 7 114Fi NoNo ratings yet
- Typhoid Fever in Children Aged Less Than PDFDocument4 pagesTyphoid Fever in Children Aged Less Than PDFAulia NurhanifaNo ratings yet
- Antimicrobial Susceptibility Testing For Salmonella Serovars Isolated From Food Samples - Five-Year Monitoring (2015-2019)Document14 pagesAntimicrobial Susceptibility Testing For Salmonella Serovars Isolated From Food Samples - Five-Year Monitoring (2015-2019)Daranee Nak-opatNo ratings yet
- Gastroenteritis Due To Typhoidal Salmonella: A Decade of Observation at An Urban and A Rural Diarrheal Disease Hospital in BangladeshDocument9 pagesGastroenteritis Due To Typhoidal Salmonella: A Decade of Observation at An Urban and A Rural Diarrheal Disease Hospital in BangladeshEmaa AmooraNo ratings yet
- Streptococcus Pneumoniae Carriage, Resistance and Serotypes Among Jordanian Children From Wadi Al Seer District, JordanDocument8 pagesStreptococcus Pneumoniae Carriage, Resistance and Serotypes Among Jordanian Children From Wadi Al Seer District, JordanInternational Medical PublisherNo ratings yet
- Tuberculosis Assayed by MODS (Microscopic-Observation DrugDocument6 pagesTuberculosis Assayed by MODS (Microscopic-Observation DrugIOSR Journal of PharmacyNo ratings yet
- 139683-Article Text-372650-1-10-20160718Document9 pages139683-Article Text-372650-1-10-20160718MATTHEW JALOWE MACARANASNo ratings yet
- Investigation of Plant Extracts in Traditional Medicine - 2010 - Journal of EthDocument6 pagesInvestigation of Plant Extracts in Traditional Medicine - 2010 - Journal of EthAgnes ContarNo ratings yet
- Islam S, Rahman F, Saurab K M, Ahmed J, Kamal SMM, Noor RDocument9 pagesIslam S, Rahman F, Saurab K M, Ahmed J, Kamal SMM, Noor RLUIS ALBERTO DE LA HOZ BARRIENTOSNo ratings yet
- Ujmr 1 - 1 2016 - 011 PDFDocument9 pagesUjmr 1 - 1 2016 - 011 PDFBahauddeen SalisuNo ratings yet
- A Retrospective Observational Study On The Sputum Samples Received by The Department of Microbiology, Teaching Hospital, Karapitiya in The Year 2007Document5 pagesA Retrospective Observational Study On The Sputum Samples Received by The Department of Microbiology, Teaching Hospital, Karapitiya in The Year 2007Rahmi AmiNo ratings yet
- First-Line Anti-Tuberculosis Drug Resistance Pattern: Original ArticleDocument6 pagesFirst-Line Anti-Tuberculosis Drug Resistance Pattern: Original ArticleyasserNo ratings yet
- Methicillin-Resistant Staphylococcus Aureus in NepDocument5 pagesMethicillin-Resistant Staphylococcus Aureus in NepHafiza AyeshaNo ratings yet
- CURRENT TRENDS IN TYPHOID FEVER MANAGEMENTDocument5 pagesCURRENT TRENDS IN TYPHOID FEVER MANAGEMENTEvaline PasakNo ratings yet
- Jurnal PDFDocument7 pagesJurnal PDFAjeng WidyastutiNo ratings yet
- Current Trends of Antibiotic Use in Bangladesh and Its Possible OutcomesDocument64 pagesCurrent Trends of Antibiotic Use in Bangladesh and Its Possible OutcomesMohammad Arafat Siddiqui75% (4)
- 6 Original CandiduriaDocument7 pages6 Original CandiduriaHarnadi WonogiriNo ratings yet
- Afriliana MDocument9 pagesAfriliana MHeniza IndriNo ratings yet
- The Foot: Original ArticleDocument5 pagesThe Foot: Original ArticleKarinaayu SerinNo ratings yet
- POTENTIAL RESISTANCEDocument6 pagesPOTENTIAL RESISTANCEMichael KevinNo ratings yet
- Microorganisms 09 02484Document12 pagesMicroorganisms 09 02484Rizwan KhalidNo ratings yet
- Whole Genome Analysis of Extensively Drug Resistant Mycobacterium Tuberculosis Strains in PeruDocument13 pagesWhole Genome Analysis of Extensively Drug Resistant Mycobacterium Tuberculosis Strains in PeruCarlos AscNo ratings yet
- 3 PDFDocument6 pages3 PDFFriskyShandy BadiNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleerikaNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Typhoidal Salmonaelle in Holy Familyred Crescent Medical College Hospital, Dhaka, BangladeshDocument4 pagesTyphoidal Salmonaelle in Holy Familyred Crescent Medical College Hospital, Dhaka, BangladeshTanveer KhanNo ratings yet
- 7712 - PMIT Fee Notice Fall 2018 D95edbDocument1 page7712 - PMIT Fee Notice Fall 2018 D95edbTanveer KhanNo ratings yet
- 9 10 16 - Civicscitizenship Bangla PDFDocument150 pages9 10 16 - Civicscitizenship Bangla PDFSharmeen HelalNo ratings yet
- Masters in Bank Management Intake-2019Document1 pageMasters in Bank Management Intake-2019Tanveer KhanNo ratings yet
- A Review of Energy Sector of Bangladesh PDFDocument8 pagesA Review of Energy Sector of Bangladesh PDFShahabuddin SuzanNo ratings yet
- 40th BCS Advertisement Download PDF, BPSC - GOV.BD, Bdjobs - GuruDocument20 pages40th BCS Advertisement Download PDF, BPSC - GOV.BD, Bdjobs - GuruIndia Jobs Seeker50% (2)
- BCS 41 - Computer & IT - PreliDocument5 pagesBCS 41 - Computer & IT - Prelisalma begumNo ratings yet
- SL No Name of Post Roll TotalDocument11 pagesSL No Name of Post Roll TotalTanveer KhanNo ratings yet
- TumiDocument1 pageTumiTanveer KhanNo ratings yet
- TheGlobalCompetitivenessReport2016-2017 FINAL PDFDocument400 pagesTheGlobalCompetitivenessReport2016-2017 FINAL PDFFermin TrujilloNo ratings yet
- This Is Ur FilleDocument1 pageThis Is Ur FilleTanveer KhanNo ratings yet
- This Is Ur FilleDocument1 pageThis Is Ur FilleTanveer KhanNo ratings yet
- 3 Bangladesh PDFDocument43 pages3 Bangladesh PDFTanveer KhanNo ratings yet
- শিকরDocument13 pagesশিকরsiam zamanNo ratings yet
- This Is Ur FilleDocument1 pageThis Is Ur FilleTanveer KhanNo ratings yet
- ( )Document24 pages( )নুরুন নবী খোকন100% (1)
- This Is Ur FilleDocument1 pageThis Is Ur FilleTanveer KhanNo ratings yet
- This Is Ur FilleDocument1 pageThis Is Ur FilleTanveer KhanNo ratings yet
- Essay Project For Written Compaigner PDFDocument105 pagesEssay Project For Written Compaigner PDFLal100% (1)
- This Is Ur FilleDocument1 pageThis Is Ur FilleTanveer KhanNo ratings yet
- This Is Ur FilleDocument1 pageThis Is Ur FilleTanveer KhanNo ratings yet
- Communal RelationDocument14 pagesCommunal RelationTanveer KhanNo ratings yet
- Bangabandhu Satellite-1Document2 pagesBangabandhu Satellite-1Tanveer KhanNo ratings yet
- RMG: Prospect of Contribution in Economy of Bangladesh: Dr. M. Habibur Rahman, Sayeed Ahmed SiddiquiDocument8 pagesRMG: Prospect of Contribution in Economy of Bangladesh: Dr. M. Habibur Rahman, Sayeed Ahmed SiddiquiTanveer KhanNo ratings yet
- Tourism in Bangladesh: A Prospects AnalysisDocument8 pagesTourism in Bangladesh: A Prospects AnalysisTanveer KhanNo ratings yet
- BCS VivaDocument111 pagesBCS VivaTanveer KhanNo ratings yet
- Delta Plan BangladeshDocument7 pagesDelta Plan BangladeshTanveer KhanNo ratings yet
- You KnoweDocument1 pageYou KnoweTanveer KhanNo ratings yet
- AbcDocument1 pageAbcTanveer KhanNo ratings yet
- © 2017 Lanternfish ESL @Document5 pages© 2017 Lanternfish ESL @DanniNo ratings yet
- Magsaysay Memorial College of Zambales, IncDocument4 pagesMagsaysay Memorial College of Zambales, IncJoanne CuestaNo ratings yet
- 2019 BerryDocument15 pages2019 BerrybryaneatscamerasNo ratings yet
- An Interactive Videogame For Arm and Hand Exercise in People With Parkinson's Disease - A Randomized Controlled Trial - Journals - NCBIDocument4 pagesAn Interactive Videogame For Arm and Hand Exercise in People With Parkinson's Disease - A Randomized Controlled Trial - Journals - NCBIWenderson MoraisNo ratings yet
- YAWNEY, C. Ways of Seeing IllnessDocument8 pagesYAWNEY, C. Ways of Seeing IllnessfernandoNo ratings yet
- Biochemistry Papers MSUDocument20 pagesBiochemistry Papers MSUShiv BhattNo ratings yet
- Association Between Working Memory Impairment and ActivitiesDocument6 pagesAssociation Between Working Memory Impairment and ActivitiesDaniel OrregoNo ratings yet
- Cardiovascular System PharmacothDocument78 pagesCardiovascular System PharmacothKumera Dinkisa ToleraNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemMary Joyce RamosNo ratings yet
- Dialog of Antenatal Care ExaminationDocument7 pagesDialog of Antenatal Care Examinationvina1598No ratings yet
- Effect of Virtual Reality Exercises On BalanceDocument9 pagesEffect of Virtual Reality Exercises On BalanceLuís Otávio S. BarbosaNo ratings yet
- Questions and Answers A Guide To Fitness and Wellness 4th Edition Ebook PDFDocument62 pagesQuestions and Answers A Guide To Fitness and Wellness 4th Edition Ebook PDFjames.jones106100% (34)
- (Neurology Now Books) Lynne P. Taylor, Alyx B. Porter Umphrey, Diane Richard - Navigating Life With A Brain Tumor-Oxford University Press, USA (2012) PDFDocument214 pages(Neurology Now Books) Lynne P. Taylor, Alyx B. Porter Umphrey, Diane Richard - Navigating Life With A Brain Tumor-Oxford University Press, USA (2012) PDFYutasya TeresaNo ratings yet
- Chapter 29: Perinatal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument2 pagesChapter 29: Perinatal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Short Blessed TestDocument3 pagesShort Blessed TestRomelyn OrdillasNo ratings yet
- Medicine: The Effectiveness of Tai Chi For Postpartum DepressionDocument4 pagesMedicine: The Effectiveness of Tai Chi For Postpartum DepressionNisa RohmatinNo ratings yet
- Uttaranchal PG College of Biomedical Sciences and HospitalDocument14 pagesUttaranchal PG College of Biomedical Sciences and HospitalpawanNo ratings yet
- Joseph Murphy Book ReviewsDocument54 pagesJoseph Murphy Book ReviewsDr. Peter Fritz Walter100% (4)
- This Is What Happens When You're A Couch Potato: Que-Resultan-Insultantes-Para-Los-HombresDocument6 pagesThis Is What Happens When You're A Couch Potato: Que-Resultan-Insultantes-Para-Los-HombresKatarina JovanovićNo ratings yet
- Case Study Ischemic Heart DiseaseDocument16 pagesCase Study Ischemic Heart DiseaseRawan KhateebNo ratings yet
- Covid Letter - North Peace Seniors HousingDocument2 pagesCovid Letter - North Peace Seniors HousingAlaskaHighwayNewsNo ratings yet
- Soal Compile Hemato-OncologyDocument25 pagesSoal Compile Hemato-OncologyDapot SianiparNo ratings yet
- Cardiac Myocytes CultureDocument6 pagesCardiac Myocytes CultureÉmerson MoreiraNo ratings yet
- Ventilasi MekanikDocument47 pagesVentilasi MekanikzahrahNo ratings yet
- The Effect of Smoking OnDocument42 pagesThe Effect of Smoking OnAndreina AcevedoNo ratings yet
- Cancer Outline Explains Causes and TreatmentsDocument3 pagesCancer Outline Explains Causes and TreatmentsDita PramudiaNo ratings yet
- Allergic RhinitisDocument27 pagesAllergic Rhinitispaningbatan.kristine.bNo ratings yet
- Infectii Oportuniste CovidDocument12 pagesInfectii Oportuniste CovidAndreea CiorneaNo ratings yet
- Chanca Piedra - Various Properties (Potential) PDFDocument17 pagesChanca Piedra - Various Properties (Potential) PDFSurya WijayaNo ratings yet
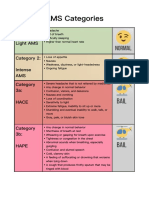
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet