You might also like
- Molecular, Genetic, and Nutritional Aspects of Major and Trace MineralsFrom EverandMolecular, Genetic, and Nutritional Aspects of Major and Trace MineralsNo ratings yet
- Diagnosis and Management of Iron Deficiency Anemia in The 21st CenturyDocument8 pagesDiagnosis and Management of Iron Deficiency Anemia in The 21st CenturyNur AlamNo ratings yet
- Iron Deficiency and Iron OverloadDocument9 pagesIron Deficiency and Iron Overloadkat9210No ratings yet
- 6 Iron Deficiency AnemiaDocument3 pages6 Iron Deficiency AnemiaMelita SabellinaNo ratings yet
- Red Blood Cell Disorders GuideDocument11 pagesRed Blood Cell Disorders GuideGea MarieNo ratings yet
- Data Interpretation For Medical StudentsDocument42 pagesData Interpretation For Medical StudentsPasTestBooks100% (6)
- Iron Deficiency Anemia & ManagementDocument60 pagesIron Deficiency Anemia & Managementswap58war100% (1)
- TRANS-1_231019_093400Document7 pagesTRANS-1_231019_093400MILLARD AYUGATNo ratings yet
- Anaemia Types and CausesDocument10 pagesAnaemia Types and CausesRazib HasanNo ratings yet
- AnemiaDocument3 pagesAnemiaAhmed ShakerNo ratings yet
- Cold Spring Harb Perspect Med-2013-MillerDocument14 pagesCold Spring Harb Perspect Med-2013-MillerIoana GhenadeNo ratings yet
- Nutrion Terapi of AnemiaDocument4 pagesNutrion Terapi of AnemiaRian LianNo ratings yet
- Anemia and Hematologic Drugs - KatzungDocument4 pagesAnemia and Hematologic Drugs - Katzungsarguss14100% (1)
- PathologyDocument30 pagesPathologyPRAJWAL PES HDNo ratings yet
- Iron, Vitamin B and Folate: Key PointsDocument6 pagesIron, Vitamin B and Folate: Key PointsyennyNo ratings yet
- Anemia - SFFTDocument5 pagesAnemia - SFFTShikha UpadhyayNo ratings yet
- Join our Telegram channel for iron deficiency anemiaDocument12 pagesJoin our Telegram channel for iron deficiency anemiaKirubel DeribNo ratings yet
- Microcytic AnemiasDocument3 pagesMicrocytic AnemiasGursimranKaurSehgalNo ratings yet
- Iron Metabolism and Its DisordersDocument10 pagesIron Metabolism and Its DisordersMario AbdiwijoyoNo ratings yet
- Iron Deficiency AnemiaDocument12 pagesIron Deficiency AnemiaMargarita TorresNo ratings yet
- Iron Deficiency: Review SeriesDocument11 pagesIron Deficiency: Review SeriesWisher PgeNo ratings yet
- ErythropoiesisDocument11 pagesErythropoiesisْNo ratings yet
- Iron Physiology of IronDocument7 pagesIron Physiology of IronAnna PodsiadłoNo ratings yet
- AnemiaDocument37 pagesAnemiadr.umme habibaNo ratings yet
- Iron Deficiency Anemia 2023Document46 pagesIron Deficiency Anemia 2023CITLALI YATZIL SANDOVAL CATALAN100% (1)
- Module 5 ERYTHROCYTE DISORDERSDocument23 pagesModule 5 ERYTHROCYTE DISORDERSPauline Louise S. DURANNo ratings yet
- Georgemar V. Arana Jr. June 20, 2014 Group III Pedia: Anemia 1) Iron Deficiency AnemiaDocument6 pagesGeorgemar V. Arana Jr. June 20, 2014 Group III Pedia: Anemia 1) Iron Deficiency AnemiageorgeNo ratings yet
- By: Dinsy Paul Juliet James Priya K Sravan Kumar. Potturi Govinda AjmeraDocument78 pagesBy: Dinsy Paul Juliet James Priya K Sravan Kumar. Potturi Govinda Ajmerashameer muhammedNo ratings yet
- Nutritional AnemiasDocument33 pagesNutritional Anemiasviviyanti znNo ratings yet
- Iron Deficiency AnemiaDocument13 pagesIron Deficiency AnemiaRommel IsraelNo ratings yet
- Disorders of Iron Metabolism Part II Iron Deficiency and Iron OverloadDocument10 pagesDisorders of Iron Metabolism Part II Iron Deficiency and Iron OverloadQistina SudarnotoNo ratings yet
- Dr. Haryanto - Kuliah Anemi Deff Fe 2011Document20 pagesDr. Haryanto - Kuliah Anemi Deff Fe 2011YeniNo ratings yet
- Individualized treatment for iron deficiency anemiaDocument12 pagesIndividualized treatment for iron deficiency anemiaGoblin HunterNo ratings yet
- Causes and Types of AnemiaDocument11 pagesCauses and Types of AnemiaJanu ArmanNo ratings yet
- Article 1659164610Document14 pagesArticle 1659164610B49 Nabila Araishabeby YudyatirtaNo ratings yet
- Anemia Types, Causes, Symptoms & TreatmentDocument1 pageAnemia Types, Causes, Symptoms & TreatmentAthirahRaraNo ratings yet
- Iron Defisience AnemiaDocument61 pagesIron Defisience AnemiaYeni Jesika SilitongaNo ratings yet
- Iron Deficiency Anemia: Imran Shahzad Anjum, MDDocument38 pagesIron Deficiency Anemia: Imran Shahzad Anjum, MDshravaniNo ratings yet
- Iron Deficiency Anemia: Causes, Symptoms and TreatmentDocument20 pagesIron Deficiency Anemia: Causes, Symptoms and TreatmentChingHuaNo ratings yet
- Iron Def ADocument20 pagesIron Def Aacs.pathNo ratings yet
- Diagnosis and Management of Iron Deficiency Anemia in The 21st CenturyDocument8 pagesDiagnosis and Management of Iron Deficiency Anemia in The 21st CenturyireneNo ratings yet
- Hepcidin's Role in Iron Distribution and Anemia of Chronic Kidney DiseaseDocument7 pagesHepcidin's Role in Iron Distribution and Anemia of Chronic Kidney DiseasegigibesiNo ratings yet
- Disorders of Iron Kinetics and Heme Metabolism ConceptsDocument12 pagesDisorders of Iron Kinetics and Heme Metabolism ConceptsJoanne JardinNo ratings yet
- 8 - Basics in Deficiency AnaemiasDocument59 pages8 - Basics in Deficiency AnaemiasWasana MendisNo ratings yet
- Iron Deficiency Anaemia: DR Mrs Stella Kanu Bmls Mbbs MSCDocument17 pagesIron Deficiency Anaemia: DR Mrs Stella Kanu Bmls Mbbs MSCDavid KanuNo ratings yet
- ANEMIAS (Sickle Cell Anemia With Pathophysiology)Document31 pagesANEMIAS (Sickle Cell Anemia With Pathophysiology)mabec pagaduan70% (10)
- Anemia Pregnancy ACOG 2021.Document10 pagesAnemia Pregnancy ACOG 2021.Laura Daniela Murillo100% (1)
- Hae Matin IcsDocument22 pagesHae Matin IcsAfreen HashmiNo ratings yet
- Iron Deficiency Anemia Diagnosis and Treatment InsightsDocument6 pagesIron Deficiency Anemia Diagnosis and Treatment InsightschameleonNo ratings yet
- Physiology I Blood & ImmunityDocument13 pagesPhysiology I Blood & Immunitynadine azmyNo ratings yet
- Topic 29: Pathophysiology of Red Cell Series: 1. HematopoiesisDocument10 pagesTopic 29: Pathophysiology of Red Cell Series: 1. HematopoiesisAelita RuseelNo ratings yet
- Anemia of Iron Abnormal Metabolism: Blue Ocean 1Document40 pagesAnemia of Iron Abnormal Metabolism: Blue Ocean 1Sukhrian MuhdaNo ratings yet
- Hematology: FANER, Ned Denebe LACANILAO, Sunshine NUCUM, Billie Kim PAGADUAN, Maribec PUA, MonalisaDocument31 pagesHematology: FANER, Ned Denebe LACANILAO, Sunshine NUCUM, Billie Kim PAGADUAN, Maribec PUA, MonalisatzuquinoNo ratings yet
- Copper Metabolism: Distribution of Copper in The BodyDocument4 pagesCopper Metabolism: Distribution of Copper in The BodyMichael HiiNo ratings yet
- Management of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerDocument8 pagesManagement of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerGeorgina Aguilar GallardoNo ratings yet
- Anemia of Iron Abnormal Metabolism: DR Bidasari Lubis, Sp. A (K) Bagian Ilmu Kesehatan Anak RSU Haji Adam Malik MedanDocument40 pagesAnemia of Iron Abnormal Metabolism: DR Bidasari Lubis, Sp. A (K) Bagian Ilmu Kesehatan Anak RSU Haji Adam Malik Medanalfat22No ratings yet
- Iron Deficiency Anaemia Armando HasudunganDocument1 pageIron Deficiency Anaemia Armando HasudunganhiNo ratings yet
- Nutritional Anemia: Dr. Mardiana, M.Kes, SP - GK Department of Clinical Nutrition Hasanuddin University MakassarDocument77 pagesNutritional Anemia: Dr. Mardiana, M.Kes, SP - GK Department of Clinical Nutrition Hasanuddin University MakassarDianaNo ratings yet
- Blood Loss: Acute Chronic Inadequate Production of Normal Blood CellsDocument11 pagesBlood Loss: Acute Chronic Inadequate Production of Normal Blood CellsSheila Amor BodegasNo ratings yet
- Fate of The Embryonic Germ LayersDocument3 pagesFate of The Embryonic Germ Layersmalav1989No ratings yet
- Infantile Hypertrophic Pyloric Stenosis: DR Feeroz Alam Khan Pediatric SurgeonDocument17 pagesInfantile Hypertrophic Pyloric Stenosis: DR Feeroz Alam Khan Pediatric SurgeonPrabhat GuptaNo ratings yet
- Haemorrhagic Anemia in PregnancyDocument8 pagesHaemorrhagic Anemia in PregnancyPrabhat GuptaNo ratings yet
- CD-3 Molecular Control of Development PDFDocument10 pagesCD-3 Molecular Control of Development PDFPrabhat GuptaNo ratings yet
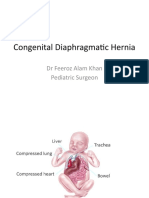
- Congenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonDocument21 pagesCongenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonPrabhat GuptaNo ratings yet
- Fate of The Embryonic Germ LayersDocument3 pagesFate of The Embryonic Germ Layersmalav1989No ratings yet
- 5 6 Intravascular UnderproductionDocument5 pages5 6 Intravascular UnderproductionPrabhat GuptaNo ratings yet
- EAR Anat and Physiol.Document22 pagesEAR Anat and Physiol.Bhaskarjyoti KheriaNo ratings yet
- Anatomy and Physiology of EarDocument11 pagesAnatomy and Physiology of EarAriguna WijayaNo ratings yet
- Anatomy and Physiology of EarDocument11 pagesAnatomy and Physiology of EarAriguna WijayaNo ratings yet
- Ear Anatomy GuideDocument29 pagesEar Anatomy GuideMenik AndromedaNo ratings yet
- 3 1 Neoplasia PDFDocument3 pages3 1 Neoplasia PDFPrabhat GuptaNo ratings yet
- Inflammation, Inflammatory Disorders, and Wound HealingDocument5 pagesInflammation, Inflammatory Disorders, and Wound HealingPrabhat GuptaNo ratings yet
- Produksi Aquos HumorDocument31 pagesProduksi Aquos Humorlady1605No ratings yet
- Acute Leukemia: Basic PrinciplesDocument3 pagesAcute Leukemia: Basic PrinciplesPrabhat GuptaNo ratings yet
- 1 4 Free Radical Injury PDFDocument2 pages1 4 Free Radical Injury PDFPrabhat GuptaNo ratings yet
- Produksi Aquos HumorDocument31 pagesProduksi Aquos Humorlady1605No ratings yet
- Is.4544.2000 0Document17 pagesIs.4544.2000 0Davorin IvićNo ratings yet
- Hba1C: Materials Required But Supplied On DemandDocument2 pagesHba1C: Materials Required But Supplied On Demandmaha muhammedNo ratings yet
- MAS110 - Week 1 - Infection Control Worksheet 2Document4 pagesMAS110 - Week 1 - Infection Control Worksheet 2geonikawilliamsNo ratings yet
- Review of Related LiteratureDocument25 pagesReview of Related LiteratureKarlvin De CardoNo ratings yet
- Attention, Distraction, and Cognitive Control Under LoadDocument7 pagesAttention, Distraction, and Cognitive Control Under LoadJosé GresalNo ratings yet
- 2019 Clinical Performance of Direct Anterior Composite Restorations A Systematic Literature Review and Critical AppraisalDocument19 pages2019 Clinical Performance of Direct Anterior Composite Restorations A Systematic Literature Review and Critical Appraisalmaroun ghalebNo ratings yet
- Member Engagement Survey Results: Hemel East Catholic Parish, Hemel Hempstead, UK - Gallup ME25 2022Document8 pagesMember Engagement Survey Results: Hemel East Catholic Parish, Hemel Hempstead, UK - Gallup ME25 2022jacobNo ratings yet
- DSE Biology - Structured Questions on Human GrowthDocument6 pagesDSE Biology - Structured Questions on Human GrowthEmily LiNo ratings yet
- Method of Statement For Survey & Setting Out MakkahDocument17 pagesMethod of Statement For Survey & Setting Out MakkahToufeeq.HSE AbrarNo ratings yet
- Shouldice Hospital Case Study SolutionDocument10 pagesShouldice Hospital Case Study SolutionSambit Rath89% (9)
- Watchkeeper oral exam guideDocument4 pagesWatchkeeper oral exam guidebandar2No ratings yet
- Study Protocol For A Randomized Controlled Trial To Test For Preventive Effects of Diabetic Foot Ulceration by Telemedicine That Includes Sensor-Equipped Insoles Combined With Photo DocumentationDocument12 pagesStudy Protocol For A Randomized Controlled Trial To Test For Preventive Effects of Diabetic Foot Ulceration by Telemedicine That Includes Sensor-Equipped Insoles Combined With Photo DocumentationAna GalvãoNo ratings yet
- PSY632 Assign Solution 1Document3 pagesPSY632 Assign Solution 1safoora ilyasNo ratings yet
- Petroleum Engineering Handbook For The Practicing Engineer Vol. 1 by M. A.Document5 pagesPetroleum Engineering Handbook For The Practicing Engineer Vol. 1 by M. A.ashishNo ratings yet
- ID Gambaran Status Gizi Pasien Diabetes Mel PDFDocument12 pagesID Gambaran Status Gizi Pasien Diabetes Mel PDFcatur rinawatiNo ratings yet
- Unsafe Acts and Unsafe ConditionsDocument47 pagesUnsafe Acts and Unsafe ConditionsGabriel Flores100% (1)
- Ki Fact Sheet - FLDocument3 pagesKi Fact Sheet - FLvitruviuzNo ratings yet
- Collaborative Working RelationshipsDocument15 pagesCollaborative Working RelationshipsMadhabi MondalNo ratings yet
- Some Info On Australian Medical Schools For CanadiansDocument5 pagesSome Info On Australian Medical Schools For Canadiansstargaze_night_42No ratings yet
- Craniofacial Surgery Brochure - PRINTDocument2 pagesCraniofacial Surgery Brochure - PRINTLaily AkbarNo ratings yet
- Care of The Older Adult P1 PointersDocument19 pagesCare of The Older Adult P1 Pointersrica sebabillonesNo ratings yet
- Read The Following Text Written by Jacquie Mccarnan and Answer The Questions On The RightDocument1 pageRead The Following Text Written by Jacquie Mccarnan and Answer The Questions On The Rightjuan florezNo ratings yet
- Optimism, Explanatory Style, and Hope: Positive PsychologyDocument25 pagesOptimism, Explanatory Style, and Hope: Positive PsychologyJay Mark Samson CabreraNo ratings yet
- Learning Materials and Students WorksheetDocument3 pagesLearning Materials and Students WorksheetRatu Rini NurhayatiNo ratings yet
- Return To Work After Work Related Injury in The Construction Sector: A Scoping ReviewDocument21 pagesReturn To Work After Work Related Injury in The Construction Sector: A Scoping ReviewchizitarankwoparaNo ratings yet
- HA-RLE-WS # 6 Assessing PainDocument3 pagesHA-RLE-WS # 6 Assessing PainJULIE ANNE CORTEZNo ratings yet
- WHO EURO 2017 2241 41996 57723 EngDocument27 pagesWHO EURO 2017 2241 41996 57723 EngNur AtiqahNo ratings yet
- Model Analysis 1 / Orthodontic Courses by Indian Dental AcademyDocument36 pagesModel Analysis 1 / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Guide to Slip, Jump and Travelling Formwork SystemsDocument7 pagesGuide to Slip, Jump and Travelling Formwork Systemssamukagomes01No ratings yet
- Maslach Burnout Toolkit For Medical Personnel Intro SheetDocument1 pageMaslach Burnout Toolkit For Medical Personnel Intro SheetMyint ZuNo ratings yet