You might also like
- Draft National Standards For Paediatric Critical Care Jan 2013Document16 pagesDraft National Standards For Paediatric Critical Care Jan 2013sarasNo ratings yet
- Managment of ScalesDocument19 pagesManagment of ScalesTanviNo ratings yet
- Holy Family College of Nursing Seminar On Tele-MedicineDocument22 pagesHoly Family College of Nursing Seminar On Tele-MedicineTanviNo ratings yet
- Genetic Counselling PDFDocument7 pagesGenetic Counselling PDFTanvi100% (1)
- Major Stake Holders in Health Care System-GovernmentDocument22 pagesMajor Stake Holders in Health Care System-GovernmentTanviNo ratings yet
- Managment of ScalesDocument19 pagesManagment of ScalesTanviNo ratings yet
- Anatomy and Physiology of BloodDocument2 pagesAnatomy and Physiology of BloodTanviNo ratings yet
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi0% (1)
- Lesson Plan On Learning DisabilityDocument28 pagesLesson Plan On Learning DisabilityTanviNo ratings yet
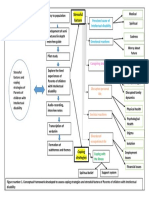
- Conceptual Framework FinalDocument1 pageConceptual Framework FinalTanviNo ratings yet
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi100% (4)
- Conjugated Bilirubin Direct Bilirubin Unconjugated Bilirubin Indirect BilirubinDocument12 pagesConjugated Bilirubin Direct Bilirubin Unconjugated Bilirubin Indirect BilirubinTanviNo ratings yet
- Common SkinDocument24 pagesCommon SkinTanviNo ratings yet
- Comlementary FeedDocument8 pagesComlementary FeedTanviNo ratings yet
- Evaluation FormatDocument1 pageEvaluation FormatTanviNo ratings yet
- Managmnt SeminarDocument24 pagesManagmnt SeminarTanviNo ratings yet
- Leaflet InventoryDocument8 pagesLeaflet InventoryTanviNo ratings yet
- DPT PresentationDocument36 pagesDPT PresentationTanviNo ratings yet
- Conceptual Framework FinalDocument1 pageConceptual Framework FinalTanviNo ratings yet
- Material On Wilms TumorDocument7 pagesMaterial On Wilms TumorTanviNo ratings yet
- Evaluation FormatDocument1 pageEvaluation FormatTanviNo ratings yet
- Evaluation FormatDocument1 pageEvaluation FormatTanviNo ratings yet
- Counseling AssignmentDocument13 pagesCounseling AssignmentTanviNo ratings yet
- ANOMALIES OF MuscloDocument114 pagesANOMALIES OF MuscloTanviNo ratings yet
- Telemedicine and TelehealthDocument22 pagesTelemedicine and TelehealthTanvi100% (1)
- Sick Young Infants (Referral, Treatment, Oral Drugs) : ImnciDocument46 pagesSick Young Infants (Referral, Treatment, Oral Drugs) : ImnciTanviNo ratings yet
- Presentation On Behavioral DisorderDocument81 pagesPresentation On Behavioral DisorderTanviNo ratings yet
- Inventory ControlDocument32 pagesInventory ControlTanvi33% (3)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 9814774723Document467 pages9814774723Ortopedia FabioNo ratings yet
- Anatomy of The Ear TMN NewDocument26 pagesAnatomy of The Ear TMN NewMerriNo ratings yet
- Faktor Resiko Neuropati Perifer Diabetik 09d66707Document9 pagesFaktor Resiko Neuropati Perifer Diabetik 09d66707Lastri AsmuniatiNo ratings yet
- 4000 IELTS Academic Word List (1) - 2: View All Words of The ListDocument3 pages4000 IELTS Academic Word List (1) - 2: View All Words of The Listfahadiqbal1992No ratings yet
- Endocrine SystemDocument4 pagesEndocrine SystemCELLINA CLARISSE DE LEONNo ratings yet
- HIV SeminarDocument45 pagesHIV SeminarDelphy VargheseNo ratings yet
- 345-Article Text-1032-1-10-20180629Document4 pages345-Article Text-1032-1-10-20180629Regina AyediaNo ratings yet
- Rapid Sequence Intubation: A Guide For AssistantsDocument6 pagesRapid Sequence Intubation: A Guide For AssistantsjackyploesNo ratings yet
- DR Ayano Final-Impacts of Sustainable Development Goals On Economic Growth in NigeriaDocument39 pagesDR Ayano Final-Impacts of Sustainable Development Goals On Economic Growth in NigeriaAyano DavidNo ratings yet
- Scott Foresman Science Grade 4Document8 pagesScott Foresman Science Grade 4rofi modiNo ratings yet
- Treatment of Acute AppendicitisDocument17 pagesTreatment of Acute Appendicitiszamir90No ratings yet
- Spiritual EndocrinologyDocument1 pageSpiritual EndocrinologyAmit RanjanNo ratings yet
- COVID-19 and The Need For Dynamic State Capabilities:: An International ComparisonDocument30 pagesCOVID-19 and The Need For Dynamic State Capabilities:: An International ComparisonTomas TomicNo ratings yet
- Chapter 1 Serology DZ 2010Document77 pagesChapter 1 Serology DZ 2010Anduamlak TeferaNo ratings yet
- 01a Calgary Cambridge Framework - BasicDocument3 pages01a Calgary Cambridge Framework - BasicJohn Sebastian Bittner SolisNo ratings yet
- Definition:: Pleural EffusionDocument4 pagesDefinition:: Pleural EffusionGetom NgukirNo ratings yet
- Monday, October 06, 2014 EditionDocument12 pagesMonday, October 06, 2014 EditionFrontPageAfricaNo ratings yet
- MCQs VTEDocument7 pagesMCQs VTEMUHAMMADNo ratings yet
- Rabbies Health Talk NewDocument10 pagesRabbies Health Talk NewAmit Ranjan100% (1)
- Chapter 8. Clinical Case Studies of AuriculotherapyDocument25 pagesChapter 8. Clinical Case Studies of AuriculotherapyIkshitNo ratings yet
- 2018 European Guidance Diagnosis and Management OsteoporosisDocument42 pages2018 European Guidance Diagnosis and Management OsteoporosisManel PopescuNo ratings yet
- Nursing Care Plan and Diagnosis For Substance AbuseDocument87 pagesNursing Care Plan and Diagnosis For Substance AbuseZohrahLiaqatNo ratings yet
- Wilson Soap Jordan SimDocument8 pagesWilson Soap Jordan Simapi-704711481No ratings yet
- 11 Nursing Care Pacemaker Emil 2019Document5 pages11 Nursing Care Pacemaker Emil 2019ameliajamirusNo ratings yet
- Logistics HandbookDocument196 pagesLogistics Handbooknikolaos13100% (1)
- CDC Lead Poisoning Prevention Signatures PDFDocument1,125 pagesCDC Lead Poisoning Prevention Signatures PDFJenika Liddell JacksonNo ratings yet
- PTBD 2Document4 pagesPTBD 2Alcntara AllenNo ratings yet
- Persistent Cough in ChildrenDocument6 pagesPersistent Cough in Childrenyujin KimNo ratings yet
- Impaired Gas ExchangeDocument1 pageImpaired Gas Exchangeruggero07No ratings yet
- Invitro Antibacterial Activity of Tamra BhasmaDocument15 pagesInvitro Antibacterial Activity of Tamra BhasmaPrashant ShastryNo ratings yet