You might also like
- Definitions and History of TelemedicineDocument39 pagesDefinitions and History of TelemedicineValarmathi100% (1)
- Telemedicine 2Document13 pagesTelemedicine 2manu sethiNo ratings yet
- TelemedicineDocument11 pagesTelemedicinemahendra singh100% (1)
- Nursing Informatics Master's Course OutlineDocument14 pagesNursing Informatics Master's Course OutlineFuad TalNo ratings yet
- TelemedicineDocument7 pagesTelemedicineAnnonymous963258No ratings yet
- TELEMEDICINEDocument6 pagesTELEMEDICINEbaby_ss100% (1)
- TelemedicineDocument8 pagesTelemedicineBarnita Sharma100% (1)
- Holy Family College of Nursing Seminar On Tele-MedicineDocument22 pagesHoly Family College of Nursing Seminar On Tele-MedicineTanviNo ratings yet
- Telemedicine- An Innovating Healthcare System In IndiaDocument20 pagesTelemedicine- An Innovating Healthcare System In IndiaSwami NathanNo ratings yet
- TeleHealth Lecture NotesDocument40 pagesTeleHealth Lecture NotesKarthik100% (3)
- Trends in Nursing PracticeDocument12 pagesTrends in Nursing PracticeJerome Cid100% (1)
- Telemedicine: Benefits, Types, Technologies and ApplicationsDocument23 pagesTelemedicine: Benefits, Types, Technologies and ApplicationsSushanth reddyNo ratings yet
- Tele Medcine PP TDocument48 pagesTele Medcine PP Trajh raj100% (1)
- Telemedicine ProposalDocument15 pagesTelemedicine ProposalIsadore Armah100% (3)
- Types of TelemedicinesDocument6 pagesTypes of TelemedicinesRahul BhagatNo ratings yet
- 7.1 TelemedicineDocument19 pages7.1 TelemedicineTrisha BawaNo ratings yet
- Tele MedicineDocument13 pagesTele MedicineBabita DhruwNo ratings yet
- TELEMEDICINE Attendance AssignmentDocument16 pagesTELEMEDICINE Attendance AssignmentShubham KumarNo ratings yet
- Trends in Telehealth White PaperDocument16 pagesTrends in Telehealth White PaperGalih Permana Qisty100% (1)
- TelemedicineDocument23 pagesTelemedicineapi-19989949No ratings yet
- Telemedicine GuidelinesDocument51 pagesTelemedicine GuidelinesNitesh100% (2)
- Telehealth Technology SyllabusDocument15 pagesTelehealth Technology SyllabusMerlin100% (1)
- Tele NursingDocument41 pagesTele Nursingcalvin100% (1)
- Telemedicine and The Transformation of Healthcare PracticeDocument16 pagesTelemedicine and The Transformation of Healthcare Practicerodrigur8036100% (3)
- Tele-Health The Modern Face of Healthcare (Jan. 2007) PDFDocument134 pagesTele-Health The Modern Face of Healthcare (Jan. 2007) PDFUsman AbbasNo ratings yet
- Telemedicine: Presenter:-Aditya Mba (Ha)Document21 pagesTelemedicine: Presenter:-Aditya Mba (Ha)Qweku BlackNo ratings yet
- Introduction to Telemedicine in 40 CharactersDocument26 pagesIntroduction to Telemedicine in 40 CharactersShane Bridges71% (7)
- Telemedicine SystemDocument22 pagesTelemedicine SystemSumit Singh100% (2)
- 13 ElectronicHealthRecordDocument48 pages13 ElectronicHealthRecordkimchi girl100% (1)
- Electronic Medical RecordDocument5 pagesElectronic Medical RecordSujatha J Jayabal100% (2)
- Telemedicine and Its Application in Public Health: Dr. Preeti TiwariDocument54 pagesTelemedicine and Its Application in Public Health: Dr. Preeti Tiwariravishukla81No ratings yet
- Summary of Purposes and ObjectivesDocument19 pagesSummary of Purposes and Objectivesrodolfo opido100% (1)
- HIS Lesson 3. Health Informatics-FinalDocument27 pagesHIS Lesson 3. Health Informatics-FinalArmand HisonaNo ratings yet
- Introduction To TelemedicineDocument25 pagesIntroduction To TelemedicineVaibhav SinhaNo ratings yet
- Telemedicine and Mobile TelemedicinDocument18 pagesTelemedicine and Mobile TelemedicinkirankumarikanchanNo ratings yet
- TelemedicineDocument39 pagesTelemedicineDeepti100% (1)
- MOH Telemedicine BlueprintDocument49 pagesMOH Telemedicine BlueprintFarihan Che MohamedNo ratings yet
- Hospital Information SystemDocument3 pagesHospital Information SystemLino MacalintalNo ratings yet
- Telehealth PaperDocument19 pagesTelehealth PaperLalitha PerumalNo ratings yet
- Telehealth and Telemedicine OverviewDocument23 pagesTelehealth and Telemedicine OverviewJoyae Chavez100% (1)
- Sample Business Plan Template A Document To Assist in The Business and Strategic Planning of Telehealth ProgramsDocument41 pagesSample Business Plan Template A Document To Assist in The Business and Strategic Planning of Telehealth Programsgopalchitta100% (3)
- Hospital Information Management SystemDocument13 pagesHospital Information Management SystemSarita yadavNo ratings yet
- HospitalDocument26 pagesHospitalPramod Kadam100% (1)
- E-Nursing TelenursingDocument12 pagesE-Nursing TelenursingAmanda Scarlet100% (1)
- Introduction to Health InformaticsDocument23 pagesIntroduction to Health InformaticsTHAO DANG100% (1)
- Model Telehealth 1Document14 pagesModel Telehealth 1Nam Pham Thanh100% (1)
- Healthcare Delivery Through Telemedicine During The COVID 19 Pandemic - Full PaperDocument11 pagesHealthcare Delivery Through Telemedicine During The COVID 19 Pandemic - Full PaperShreyas Suresh RaoNo ratings yet
- Use of Computers in Nursing ResearchDocument2 pagesUse of Computers in Nursing ResearchPrasanth Kurien Mathew50% (2)
- Global Telemedicine and EHealthDocument6 pagesGlobal Telemedicine and EHealthn1i1No ratings yet
- TelecardiologyDocument20 pagesTelecardiologyPushpavalli Mohan100% (1)
- Electronic Health RecordDocument20 pagesElectronic Health RecordLiza Visbal- DionaldoNo ratings yet
- E-Nursing, Telemedicine, Telenursing, EmrDocument42 pagesE-Nursing, Telemedicine, Telenursing, EmrDhanya100% (1)
- Global Telemedicine Market Outlook To 2018Document3 pagesGlobal Telemedicine Market Outlook To 2018SeoExportNo ratings yet
- Telemedicine in Ethiopia Report by GetuDocument8 pagesTelemedicine in Ethiopia Report by GetulayNo ratings yet
- Health Informatics & Legal Issues - DorisDocument59 pagesHealth Informatics & Legal Issues - DorisMonaNo ratings yet
- E-Nursing, Telemedicine and TelenursingDocument27 pagesE-Nursing, Telemedicine and TelenursingLekshmi Manu61% (28)
- 2.emerging Technology in Nursing Practice PDFDocument89 pages2.emerging Technology in Nursing Practice PDFgao1989100% (2)
- INTRODUCTIONDocument13 pagesINTRODUCTIONnimila gopiNo ratings yet
- Rockson Ohene AsanteDocument19 pagesRockson Ohene AsanteRockson Ohene AsanteNo ratings yet
- Managment of ScalesDocument19 pagesManagment of ScalesTanviNo ratings yet
- Genetic Counselling PDFDocument7 pagesGenetic Counselling PDFTanvi100% (1)
- Inborn Errors of Metabolism - 2019 PDFDocument13 pagesInborn Errors of Metabolism - 2019 PDFTanviNo ratings yet
- Managment of ScalesDocument19 pagesManagment of ScalesTanviNo ratings yet
- Holy Family College of Nursing Seminar On Tele-MedicineDocument22 pagesHoly Family College of Nursing Seminar On Tele-MedicineTanviNo ratings yet
- Major Stake Holders in Health Care System-GovernmentDocument22 pagesMajor Stake Holders in Health Care System-GovernmentTanviNo ratings yet
- Draft National Standards For Paediatric Critical Care Jan 2013Document16 pagesDraft National Standards For Paediatric Critical Care Jan 2013sarasNo ratings yet
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi0% (1)
- Anatomy and Physiology of BloodDocument2 pagesAnatomy and Physiology of BloodTanviNo ratings yet
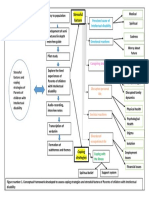
- Conceptual Framework FinalDocument1 pageConceptual Framework FinalTanviNo ratings yet
- Leaflet InventoryDocument8 pagesLeaflet InventoryTanviNo ratings yet
- Essential Guide to Complementary FeedingDocument8 pagesEssential Guide to Complementary FeedingTanviNo ratings yet
- Lesson Plan On Learning DisabilityDocument28 pagesLesson Plan On Learning DisabilityTanviNo ratings yet
- Common SkinDocument24 pagesCommon SkinTanviNo ratings yet
- Conceptual Framework FinalDocument1 pageConceptual Framework FinalTanviNo ratings yet
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi100% (4)
- Material On Wilms TumorDocument7 pagesMaterial On Wilms TumorTanviNo ratings yet
- DPT PresentationDocument36 pagesDPT PresentationTanviNo ratings yet
- ANOMALIES OF MuscloDocument114 pagesANOMALIES OF MuscloTanviNo ratings yet
- Managmnt SeminarDocument24 pagesManagmnt SeminarTanviNo ratings yet
- Evaluation FormatDocument1 pageEvaluation FormatTanviNo ratings yet
- Evaluation FormatDocument1 pageEvaluation FormatTanviNo ratings yet
- Conjugated Bilirubin Direct Bilirubin Unconjugated Bilirubin Indirect BilirubinDocument12 pagesConjugated Bilirubin Direct Bilirubin Unconjugated Bilirubin Indirect BilirubinTanviNo ratings yet
- Sick Young Infants (Referral, Treatment, Oral Drugs) : ImnciDocument46 pagesSick Young Infants (Referral, Treatment, Oral Drugs) : ImnciTanviNo ratings yet
- Counseling AssignmentDocument13 pagesCounseling AssignmentTanviNo ratings yet
- Presentation On Behavioral DisorderDocument81 pagesPresentation On Behavioral DisorderTanviNo ratings yet
- Evaluation FormatDocument1 pageEvaluation FormatTanviNo ratings yet
- Inventory ControlDocument32 pagesInventory ControlTanvi33% (3)
- Amoxgentin - Amoxycillin & Potassium Clavulanate Injection - Export 600mg I.V - InFODocument1 pageAmoxgentin - Amoxycillin & Potassium Clavulanate Injection - Export 600mg I.V - InFOAnonymous BVD7IKfNo ratings yet
- UpperairwayobstructionDocument9 pagesUpperairwayobstructionAzzhr FahNo ratings yet
- Classification of Partially Edentulous ArchesDocument5 pagesClassification of Partially Edentulous ArchesmujtabaNo ratings yet
- Active+Assistive+ PPT+6Document28 pagesActive+Assistive+ PPT+6Mhmd IrakyNo ratings yet
- Mandibular Molar Protraction With Temporary Anchorage DevicesDocument5 pagesMandibular Molar Protraction With Temporary Anchorage Devicescarlosasd15No ratings yet
- TS PG Medical Management Quota Admissions ListDocument1 pageTS PG Medical Management Quota Admissions ListSunny4288No ratings yet
- Newman Carranza's Clinical Periodonyology 11th Ed-Ublog TKDocument5 pagesNewman Carranza's Clinical Periodonyology 11th Ed-Ublog TKFahmi RexandyNo ratings yet
- Contemporary Oral Oncology Diagnosis and ManagementDocument327 pagesContemporary Oral Oncology Diagnosis and ManagementJacky JunaediNo ratings yet
- Meconium Passage in UteroDocument12 pagesMeconium Passage in UteroJennifer IbarraNo ratings yet
- "Article-PDF-naresh Sharma Binita Srivastava Hind P Bhatia Arch-849Document3 pages"Article-PDF-naresh Sharma Binita Srivastava Hind P Bhatia Arch-849Ruchi ShahNo ratings yet
- 8 Places in Europe LWRDocument4 pages8 Places in Europe LWRArjelle MalazaNo ratings yet
- Rhazes' Contributions to Neuroanatomy and NeurologyDocument3 pagesRhazes' Contributions to Neuroanatomy and NeurologyNirav PatelNo ratings yet
- Bipolar Disorder by Fountoulakis2014Document733 pagesBipolar Disorder by Fountoulakis2014Santhana Raj J100% (3)
- Safe and Gentle Ventilation For Little Patients Easy - Light - SmartDocument4 pagesSafe and Gentle Ventilation For Little Patients Easy - Light - SmartSteven BrownNo ratings yet
- GoodPractice WL U01ReceivingPatientDocument3 pagesGoodPractice WL U01ReceivingPatientReka Kutasi100% (1)
- HyphemaDocument19 pagesHyphemaLiyanti RinceNo ratings yet
- Organizational AssessmentDocument11 pagesOrganizational Assessmentapi-437229197No ratings yet
- Eye, E.N.T. & Dental AnaesthesiaDocument22 pagesEye, E.N.T. & Dental AnaesthesiawellawalalasithNo ratings yet
- Quality Indicators & Safety PresentationDocument63 pagesQuality Indicators & Safety Presentationapi-28181342267% (3)
- Melanie Klein and Early Object Relations TheoryDocument72 pagesMelanie Klein and Early Object Relations TheoryAastha Jain100% (5)
- Pediatrics Case StudiesDocument32 pagesPediatrics Case StudiesprinceejNo ratings yet
- Infanrix Hexa PI 005Document13 pagesInfanrix Hexa PI 005m.i.n.h.a.j100% (1)
- Kumpulan Jurnal JantungDocument200 pagesKumpulan Jurnal JantungMaya RustamNo ratings yet
- Children Traffic Safety and Traffic EducationDocument7 pagesChildren Traffic Safety and Traffic EducationCristina IoanaNo ratings yet
- Ministry of Health Malaysia releases updated credentialing guidelinesDocument142 pagesMinistry of Health Malaysia releases updated credentialing guidelinesFirdaus Al HafizNo ratings yet
- Surgery or General Medicine - A Study of The Reasons Underlying The Choice of Medical SpecialtyDocument6 pagesSurgery or General Medicine - A Study of The Reasons Underlying The Choice of Medical SpecialtyCarol BusseNo ratings yet
- Healthcare Professionals Qualification Requirements (PQR) 2014-1Document123 pagesHealthcare Professionals Qualification Requirements (PQR) 2014-1JerilNo ratings yet
- Myasthenia Gravis ReferatDocument26 pagesMyasthenia Gravis ReferatUlfa TitiswariNo ratings yet
- Weil-Felix Test in Diagnosis of ScrubDocument3 pagesWeil-Felix Test in Diagnosis of ScrubvyasakandarpNo ratings yet
- Cerebellar InfarctionDocument23 pagesCerebellar InfarctionShane LuyNo ratings yet