You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Starting A Business Candle Making 2009Document2 pagesStarting A Business Candle Making 2009Carlo Fabros Junio100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Year 10 Maths PlaneDocument62 pagesYear 10 Maths Planehal wangNo ratings yet
- Philippine LiteratureDocument82 pagesPhilippine LiteratureLovelene Chrizze100% (5)
- 2010-12 600 800 Rush Switchback RMK Service Manual PDFDocument430 pages2010-12 600 800 Rush Switchback RMK Service Manual PDFBrianCook73% (11)
- World Alzheimer Report 2021Document314 pagesWorld Alzheimer Report 2021MiguelySusy Ramos-RojasNo ratings yet
- 2010 HSC Exam PhysicsDocument42 pages2010 HSC Exam PhysicsVictor345No ratings yet
- Edith Kaplan and The Boston Process Approach Libon2013Document13 pagesEdith Kaplan and The Boston Process Approach Libon2013MiguelySusy Ramos-RojasNo ratings yet
- Ketchikan Shipyard Improvements Plan CompleteDocument230 pagesKetchikan Shipyard Improvements Plan CompleteOpó Ishak Bawias Adare100% (1)
- S06 - 1 THC560 DD311Document128 pagesS06 - 1 THC560 DD311Canchari Pariona Jhon AngelNo ratings yet
- IntroducingCompassionFocusedTherapy (Gilbert, 2009)Document10 pagesIntroducingCompassionFocusedTherapy (Gilbert, 2009)MiguelySusy Ramos-RojasNo ratings yet
- Building and Enhancing New Literacies Across The CurriculumDocument119 pagesBuilding and Enhancing New Literacies Across The CurriculumLowela Kasandra100% (3)
- Memory Complaint Scale (MCS)Document7 pagesMemory Complaint Scale (MCS)MiguelySusy Ramos-RojasNo ratings yet
- Metabolic Syndrome, Mild Cognitive Impairment, and Dementia: A Meta-Analysis of Longitudinal StudiesDocument13 pagesMetabolic Syndrome, Mild Cognitive Impairment, and Dementia: A Meta-Analysis of Longitudinal StudiesMiguelySusy Ramos-RojasNo ratings yet
- Metabolic Syndrome and LongitudinalDocument11 pagesMetabolic Syndrome and LongitudinalMiguelySusy Ramos-RojasNo ratings yet
- Carroll - Identity Grief and SelfDocument19 pagesCarroll - Identity Grief and SelfMiguelySusy Ramos-RojasNo ratings yet
- Establishing and Measuring Treatment Fidelity of A Complex Cognitive Rehabilitation Intervention The Multicontext ApproachDocument12 pagesEstablishing and Measuring Treatment Fidelity of A Complex Cognitive Rehabilitation Intervention The Multicontext ApproachMiguelySusy Ramos-RojasNo ratings yet
- Clinical Assessment of Prefrontal Lobe Functions Stuss 2018Document23 pagesClinical Assessment of Prefrontal Lobe Functions Stuss 2018MiguelySusy Ramos-RojasNo ratings yet
- Overview of cognitive and perceptual rehabilitationDocument31 pagesOverview of cognitive and perceptual rehabilitationDewi Nur Puspita SariNo ratings yet
- Factor Structure of The Everyday Memory Questionnaire Cornish2000Document12 pagesFactor Structure of The Everyday Memory Questionnaire Cornish2000MiguelySusy Ramos-RojasNo ratings yet
- Compassion Focused Therapy After Traumatic Brain Injury: Theoretical Foundations and A Case IllustrationDocument13 pagesCompassion Focused Therapy After Traumatic Brain Injury: Theoretical Foundations and A Case IllustrationMiguelySusy Ramos-RojasNo ratings yet
- Standardized Outcome Measures in Stroke Rehabilitation and Falls After Discharge - A Cohort StudyDocument9 pagesStandardized Outcome Measures in Stroke Rehabilitation and Falls After Discharge - A Cohort StudyMiguelySusy Ramos-RojasNo ratings yet
- Reconstruction Identity After Brain InjuryDocument17 pagesReconstruction Identity After Brain InjuryMiguelySusy Ramos-RojasNo ratings yet
- Cognitive Rehabilitation: A Goal-Planning Approach: Barbara A. Wilson, PHDDocument14 pagesCognitive Rehabilitation: A Goal-Planning Approach: Barbara A. Wilson, PHDMiguelySusy Ramos-RojasNo ratings yet
- Establishing and Measuring Treatment Fidelity of A Complex Cognitive Rehabilitation Intervention The Multicontext ApproachDocument12 pagesEstablishing and Measuring Treatment Fidelity of A Complex Cognitive Rehabilitation Intervention The Multicontext ApproachMiguelySusy Ramos-RojasNo ratings yet
- Goal Planning and Neurorehabilitation: The Wolfson Neurorehabilitation Centre ApproachDocument13 pagesGoal Planning and Neurorehabilitation: The Wolfson Neurorehabilitation Centre ApproachMiguelySusy Ramos-RojasNo ratings yet
- Overview of cognitive and perceptual rehabilitationDocument31 pagesOverview of cognitive and perceptual rehabilitationDewi Nur Puspita SariNo ratings yet
- Informant Questionnaire On Cognitive Decline in The Elderly (IQCODE) For Classifying Cognitive Dysfunction As Cognitively Normal, Mild Cognitive Impairment, and DementiaDocument7 pagesInformant Questionnaire On Cognitive Decline in The Elderly (IQCODE) For Classifying Cognitive Dysfunction As Cognitively Normal, Mild Cognitive Impairment, and DementiaMiguelySusy Ramos-RojasNo ratings yet
- A Scoping Review of Communicating Neuropsychological Test Results To Patients and Family Members2021Document22 pagesA Scoping Review of Communicating Neuropsychological Test Results To Patients and Family Members2021MiguelySusy Ramos-RojasNo ratings yet
- Soto-Añari Et Al., IPADocument2 pagesSoto-Añari Et Al., IPAMiguelySusy Ramos-RojasNo ratings yet
- ArdilaDocument3 pagesArdilaMiguelySusy Ramos-RojasNo ratings yet
- Clinical Assessment of Prefrontal Lobe Functions Stuss 2018Document23 pagesClinical Assessment of Prefrontal Lobe Functions Stuss 2018MiguelySusy Ramos-RojasNo ratings yet
- The Association Between Subjective Memory Complaints and Sleep Within Older African American AdultsDocument10 pagesThe Association Between Subjective Memory Complaints and Sleep Within Older African American AdultsMiguelySusy Ramos-RojasNo ratings yet
- From Subjective Cognitive Complaints To Dementia - Who Is at Risk? - A Systematic ReviewDocument10 pagesFrom Subjective Cognitive Complaints To Dementia - Who Is at Risk? - A Systematic ReviewMiguelySusy Ramos-RojasNo ratings yet
- Depression and Incidence of Frailty in Older People From Six Latin American CountriesDocument8 pagesDepression and Incidence of Frailty in Older People From Six Latin American CountriesMiguelySusy Ramos-RojasNo ratings yet
- Improving The Quality of Clinical Neuropsychological Research - Mandatory Use of Reporting GuidelinesDocument21 pagesImproving The Quality of Clinical Neuropsychological Research - Mandatory Use of Reporting GuidelinesMiguelySusy Ramos-RojasNo ratings yet
- JoernalDocument7 pagesJoernalyennaputriNo ratings yet
- NIH Public AccessDocument19 pagesNIH Public AccessMiguelySusy Ramos-RojasNo ratings yet
- 99th Indian Science Congress (Bhubaneshwar)Document95 pages99th Indian Science Congress (Bhubaneshwar)Aadarsh DasNo ratings yet
- School of Public Health: Haramaya University, ChmsDocument40 pagesSchool of Public Health: Haramaya University, ChmsRida Awwal100% (1)
- Tuberculin Skin Test: Facilitator GuideDocument31 pagesTuberculin Skin Test: Facilitator GuideTiwi NaloleNo ratings yet
- How To Pass in University Arrear Exams?Document26 pagesHow To Pass in University Arrear Exams?arrearexam100% (6)
- TNG UPDATE InstructionsDocument10 pagesTNG UPDATE InstructionsDiogo Alexandre Crivelari CrivelNo ratings yet
- Guitar Chords:: Chorus: CF CF FCFC CFGC Verse: CF CF FCFC CFGCDocument17 pagesGuitar Chords:: Chorus: CF CF FCFC CFGC Verse: CF CF FCFC CFGCKhuanZumeNo ratings yet
- Victor Mejia ResumeDocument1 pageVictor Mejia Resumeapi-510300922No ratings yet
- GastrectomyDocument19 pagesGastrectomyCyrus GarciaNo ratings yet
- Fashion Cycle StepsDocument2 pagesFashion Cycle Stepssaranya narenNo ratings yet
- Jotrun TDSDocument4 pagesJotrun TDSBiju_PottayilNo ratings yet
- Presentation of Urban RegenerationsDocument23 pagesPresentation of Urban RegenerationsRafiuddin RoslanNo ratings yet
- Early Diabetic Risk Prediction Using Machine Learning Classification TechniquesDocument6 pagesEarly Diabetic Risk Prediction Using Machine Learning Classification TechniquesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Appendix 1 Application FormDocument13 pagesAppendix 1 Application FormSharifahrodiah SemaunNo ratings yet
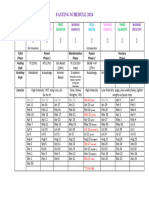
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Guillermo Estrella TolentinoDocument15 pagesGuillermo Estrella TolentinoJessale JoieNo ratings yet
- Characteristics and Guidelines of PublicspaceDocument3 pagesCharacteristics and Guidelines of PublicspaceJanani SurenderNo ratings yet
- An Overview of The FUPLA 2 Tools: Project DatabaseDocument2 pagesAn Overview of The FUPLA 2 Tools: Project DatabaseJulio Cesar Rojas SaavedraNo ratings yet
- One - Pager - SOGEVAC SV 320 BDocument2 pagesOne - Pager - SOGEVAC SV 320 BEOLOS COMPRESSORS LTDNo ratings yet
- Technical Description: BoilerDocument151 pagesTechnical Description: BoilerÍcaro VianaNo ratings yet
- Technology Consulting: Amruta Kulkarni Anu Abraham Rajat JainDocument9 pagesTechnology Consulting: Amruta Kulkarni Anu Abraham Rajat JainRajat JainNo ratings yet
- History and Development of the Foodservice IndustryDocument23 pagesHistory and Development of the Foodservice IndustryMaria Athenna MallariNo ratings yet
- Clarinet Lecture Recital - Jude StefanikDocument35 pagesClarinet Lecture Recital - Jude Stefanikapi-584164068No ratings yet