You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Muscle Stiffness and Strength and Their PDFDocument6 pagesMuscle Stiffness and Strength and Their PDFVioleta OrsettiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Probability of Walking Wheeled Mobility PDFDocument6 pagesProbability of Walking Wheeled Mobility PDFVioleta OrsettiNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Living With Cerebral Palsy and The PowerDocument8 pagesLiving With Cerebral Palsy and The PowerVioleta OrsettiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Caries Experience in Children and Adoles PDFDocument2 pagesCaries Experience in Children and Adoles PDFVioleta OrsettiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Drooling Saliva Production and Swallowin PDFDocument6 pagesDrooling Saliva Production and Swallowin PDFVioleta OrsettiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Context-Dependency of Mobility in ChildrDocument6 pagesContext-Dependency of Mobility in ChildrVioleta OrsettiNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Female Age-Related Fertility Decline: Committee Opinion No. 589Document2 pagesFemale Age-Related Fertility Decline: Committee Opinion No. 589Violeta OrsettiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Start Browse by Day Author Index Keyword IndexDocument2 pagesStart Browse by Day Author Index Keyword IndexVioleta OrsettiNo ratings yet
- Testing and Interpreting Measures of Ovarian Reserve-NoprintDocument9 pagesTesting and Interpreting Measures of Ovarian Reserve-NoprintVioleta OrsettiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
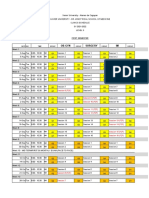
- Level 3 Clinics Schedule Clinics Groupings Group Leaders and PreceptorsDocument24 pagesLevel 3 Clinics Schedule Clinics Groupings Group Leaders and PreceptorsKIM LORIE YAP PASCUALNo ratings yet
- 3rd Lecture On The Histology of Female Reproductive System by Dr. RoomiDocument19 pages3rd Lecture On The Histology of Female Reproductive System by Dr. RoomiMudassar RoomiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- DR Andreas Patsalides MD, PHD, Gynecologist Head of Gynecology Clinic Pafos General Hospital CyprusDocument85 pagesDR Andreas Patsalides MD, PHD, Gynecologist Head of Gynecology Clinic Pafos General Hospital CypruspingusNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Adoption MethodDocument18 pagesAdoption Methodsuchismita pandaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Evaluation of Infertile CoupleDocument70 pagesEvaluation of Infertile CoupleNdenwaneku OkuwaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 2018521625078-Mohan EthirajanDocument7 pages2018521625078-Mohan EthirajanMohan EthirajanNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Quarter3 Week 1: (MELC) : Compose An Argumentative Essay Reference: English 10 Learner's Material - Celebrating DiversityDocument7 pagesQuarter3 Week 1: (MELC) : Compose An Argumentative Essay Reference: English 10 Learner's Material - Celebrating Diversitymy musicNo ratings yet
- Preventive Powers of Ovulation and ProgesteroneDocument6 pagesPreventive Powers of Ovulation and ProgesteroneEuge GuareschiNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Menstruation Myths and Their FactsDocument3 pagesMenstruation Myths and Their FactsAngelica Calamba CalicaNo ratings yet
- 6worksheet ReproductionDocument2 pages6worksheet ReproductionivyNo ratings yet
- Evaluate The Size of The Pelvis and Cervix Trusted SourceDocument2 pagesEvaluate The Size of The Pelvis and Cervix Trusted SourceDjoudji ngoune AmabelleNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Dism-PMSDocument29 pagesDism-PMSAg NesNo ratings yet
- Efektivitas Pemberian Rebusan Kunyit Asam Terhadap Penurunan DismenoreaDocument9 pagesEfektivitas Pemberian Rebusan Kunyit Asam Terhadap Penurunan DismenoreaDianita NurramaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Leaflet VaginasisDocument2 pagesLeaflet VaginasisMymy SofiNo ratings yet
- Case Study - Uterine FibroidsDocument4 pagesCase Study - Uterine FibroidsRomeo ReyesNo ratings yet
- Abnormalities Involving UterusDocument20 pagesAbnormalities Involving UterusDrRajkumar PatelNo ratings yet
- Family PlanningDocument18 pagesFamily Planningselja0% (1)
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmGabriella AguirreNo ratings yet
- Proposed Regional Genitourinary Center: in CalabarzonDocument45 pagesProposed Regional Genitourinary Center: in Calabarzonallyssa monica duNo ratings yet
- For The MRCOG and Beyond: Reproductive EndocrinologyDocument19 pagesFor The MRCOG and Beyond: Reproductive EndocrinologyApurba PailanNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument7 pagesBest Practice & Research Clinical Obstetrics and GynaecologyEko TulusNo ratings yet
- Full Download Book Cunningham and Gilstraps Operative Obstetrics PDFDocument41 pagesFull Download Book Cunningham and Gilstraps Operative Obstetrics PDFrogelio.dorcy170100% (16)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Reproductive System of Cats and DogsDocument19 pagesReproductive System of Cats and DogsKatrina PonceNo ratings yet
- Ass Ectopic PregnancyDocument10 pagesAss Ectopic PregnancyPriyaNo ratings yet
- Oral Hormonal Contraceptive: BY Magdyabdelrahmanmohamed 2 0 1 5Document36 pagesOral Hormonal Contraceptive: BY Magdyabdelrahmanmohamed 2 0 1 5UdtjeVanDerJeykNo ratings yet
- Lesson Plan On MenopauseDocument16 pagesLesson Plan On MenopauseRavina Patel100% (6)
- Delivery Nurses NotesDocument2 pagesDelivery Nurses NotesRS Buenavista67% (3)
- Science and Health 5Document15 pagesScience and Health 5Ryrl ShinNo ratings yet
- Assessment Diagnosis Rationale Planning Interventio N Rationale EvaluationDocument2 pagesAssessment Diagnosis Rationale Planning Interventio N Rationale Evaluationbambem aevanNo ratings yet
- Section A:: Breastfeeding Counselling and Support Actions - Breastfeeding 1 - 21Document24 pagesSection A:: Breastfeeding Counselling and Support Actions - Breastfeeding 1 - 21Abebe TilahunNo ratings yet