You might also like
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- SJDS 34100 103Document4 pagesSJDS 34100 103Andi Sry PermatasariNo ratings yet
- E1ht PDFDocument15 pagesE1ht PDFShweta KhannaNo ratings yet
- Fixed Partial Denture (PDFDrive)Document23 pagesFixed Partial Denture (PDFDrive)Mohamad JihadNo ratings yet
- Complete Denture Copy Technique - A Practical Application: Case ReportDocument6 pagesComplete Denture Copy Technique - A Practical Application: Case ReportRNo ratings yet
- Variations in Bracket Placement in The Preadjusted Orthodontic ApplianceDocument6 pagesVariations in Bracket Placement in The Preadjusted Orthodontic ApplianceAna Maria Clara HernándezNo ratings yet
- A Tooth-Stabilized Surgical Template For AlveolectomyDocument3 pagesA Tooth-Stabilized Surgical Template For Alveolectomyheri asriyadiNo ratings yet
- The Socket Shield Technique Case ReportDocument5 pagesThe Socket Shield Technique Case ReportAhmed Mohammed Saaduddin SapriNo ratings yet
- Dental ArticulatorsDocument10 pagesDental ArticulatorsOmar Al-FatyanNo ratings yet
- Three Dimensional Imaging in DentistryDocument26 pagesThree Dimensional Imaging in Dentistrydorasani99No ratings yet
- Study Models Key for Orthodontic DiagnosisDocument9 pagesStudy Models Key for Orthodontic DiagnosisAhmed SharabyNo ratings yet
- 1988 - Template For Positioning and Angulation of Intraosseous ImplantsDocument5 pages1988 - Template For Positioning and Angulation of Intraosseous ImplantsVõHoàngThủyTiênNo ratings yet
- Broderick Occlusal Plane Analyzer (1DIEGO)Document5 pagesBroderick Occlusal Plane Analyzer (1DIEGO)diegoNo ratings yet
- Dental - Ijdrd-Unconventional Denture-Deepak VikhheDocument6 pagesDental - Ijdrd-Unconventional Denture-Deepak VikhheTJPRC PublicationsNo ratings yet
- Emergence Angles of The Cej in Natural Max Ant TeethDocument8 pagesEmergence Angles of The Cej in Natural Max Ant TeethN&M CHANNELNo ratings yet
- Pneumocephalus As A Fatal But Very RareDocument27 pagesPneumocephalus As A Fatal But Very RareHossam ThabetNo ratings yet
- Jaw Relation Records Guide Fixed ProsthodonticsDocument16 pagesJaw Relation Records Guide Fixed ProsthodonticsbkprosthoNo ratings yet
- Chiu 2015 BimaxillaryDocument36 pagesChiu 2015 BimaxillaryMax FerNo ratings yet
- The ABCs of Occlusion and Articulation Reducing Positive Errors For Fewer Adjustments - Dentistry TodayDocument12 pagesThe ABCs of Occlusion and Articulation Reducing Positive Errors For Fewer Adjustments - Dentistry Todayfabian hernandez medinaNo ratings yet
- Case Report: Telescopic Overdenture and Implant Supported Fixed Partial Denture: A Pragmatic Treatment ApproachDocument8 pagesCase Report: Telescopic Overdenture and Implant Supported Fixed Partial Denture: A Pragmatic Treatment ApproachJyoti VermaNo ratings yet
- Hobo Technique PDFDocument8 pagesHobo Technique PDFAmar BimavarapuNo ratings yet
- 85-6403 e (C) F (T) PF1 (MH) Pfa (H)Document3 pages85-6403 e (C) F (T) PF1 (MH) Pfa (H)ikeuchi_ogawaNo ratings yet
- Using Intraoral Gothic Arch Tracing To Balance Full Dentures and Determine Centric Relation and Occlusal Vertical DimensionDocument15 pagesUsing Intraoral Gothic Arch Tracing To Balance Full Dentures and Determine Centric Relation and Occlusal Vertical DimensionAlfred OrozcoNo ratings yet
- Tanvi Jaiswal........ Afs... Swe..Document8 pagesTanvi Jaiswal........ Afs... Swe..sumeet sharmaNo ratings yet
- Reviewing Occlusal Protection Theory and PracticeDocument10 pagesReviewing Occlusal Protection Theory and PracticeHuong KamNo ratings yet
- Prosthodontics May 2015Document39 pagesProsthodontics May 2015samikshaNo ratings yet
- RPD 2016 Quiz 1 Study GuideDocument9 pagesRPD 2016 Quiz 1 Study Guideapi-296866881No ratings yet
- Ortho Bone ScrewDocument17 pagesOrtho Bone ScrewmedicalcenterNo ratings yet
- Hourfar2015 PDFDocument7 pagesHourfar2015 PDFAndres CoboNo ratings yet
- A Modification of The Altered Cast TechniqueDocument2 pagesA Modification of The Altered Cast TechniqueChirag Gorasiya100% (1)
- SJRD Id34Document5 pagesSJRD Id34Pradeep PradyNo ratings yet
- Prepearing Teeth For RPDDocument14 pagesPrepearing Teeth For RPDShreyans DamadeNo ratings yet
- Densit Osoasa A Palatului DurDocument8 pagesDensit Osoasa A Palatului DurDiana DrutaNo ratings yet
- Transfer of Information For Esthetic and Functional Predictability in Severe Wear Cases.Document11 pagesTransfer of Information For Esthetic and Functional Predictability in Severe Wear Cases.jorefe12No ratings yet
- 1Document7 pages1Claudiu LefterNo ratings yet
- Overdenture Abutments Under A Fixed Partial Denture: Case Report of A Preventive Prosthodontic ApproachDocument4 pagesOverdenture Abutments Under A Fixed Partial Denture: Case Report of A Preventive Prosthodontic ApproachDame rohanaNo ratings yet
- Articol Pentru Teme 14-18Document9 pagesArticol Pentru Teme 14-18Diamanta Yalomit CirsteaNo ratings yet
- Artigo MedeirosDocument6 pagesArtigo MedeirosEugénio MartinsNo ratings yet
- Maxillary Immediate Denture: A Case Report: International Journal of Medical and Health ResearchDocument3 pagesMaxillary Immediate Denture: A Case Report: International Journal of Medical and Health Researchwaf51No ratings yet
- Bodily Distalization of Molars With Absolute AnchorageDocument12 pagesBodily Distalization of Molars With Absolute AnchorageAnamika AttrishiNo ratings yet
- Diagnostic Wax-Up Technique for Restorative DentistryDocument9 pagesDiagnostic Wax-Up Technique for Restorative Dentistryilich sevillaNo ratings yet
- What Is RPD SurveyingDocument7 pagesWhat Is RPD SurveyingBrandon AviciiNo ratings yet
- PIIS0022391304004056Document1 pagePIIS0022391304004056Najeeb UllahNo ratings yet
- 2020 - Stereolithographic Surgical Guide With A Combination of Tooth and Bone SupportDocument13 pages2020 - Stereolithographic Surgical Guide With A Combination of Tooth and Bone SupportVõHoàngThủyTiênNo ratings yet
- Lyu 2018Document7 pagesLyu 2018Andres CoboNo ratings yet
- Conventional Implant With Orthodontic Treatment For Anterior Missing Tooth ManagementDocument2 pagesConventional Implant With Orthodontic Treatment For Anterior Missing Tooth ManagementErwin SutonoNo ratings yet
- Band and Pontic: A Modified Band and Loop Space Maintainer - Clinical InnovationDocument3 pagesBand and Pontic: A Modified Band and Loop Space Maintainer - Clinical InnovationIJAR JOURNALNo ratings yet
- Safe Zone AjoDocument7 pagesSafe Zone AjojoeNo ratings yet
- Loss of Anterior Interdental Tissue SolutionsDocument5 pagesLoss of Anterior Interdental Tissue Solutionsjinny1_0No ratings yet
- Isrn Dentistry2012-259891 PDFDocument7 pagesIsrn Dentistry2012-259891 PDFAdriana Paola Vega YanesNo ratings yet
- Fabrication of Occlusal RimsDocument4 pagesFabrication of Occlusal RimsHarsha Reddy100% (1)
- Dawson - Why Porcelain BreaksDocument2 pagesDawson - Why Porcelain BreaksjarodzeeNo ratings yet
- OshidaDocument8 pagesOshidaKaren Viviana Noreña GiraldoNo ratings yet
- The Maintenance of Pulp Health 17 Years After Root Fracture in A Maxillary Incisor Illustrating The Diagnostic Benefits of Cone Bean Computed TomographyDocument7 pagesThe Maintenance of Pulp Health 17 Years After Root Fracture in A Maxillary Incisor Illustrating The Diagnostic Benefits of Cone Bean Computed TomographyArturo Trejo VeraNo ratings yet
- Maxillary Immediate Denture: A Case Report: International Journal of Medical and Health ResearchDocument3 pagesMaxillary Immediate Denture: A Case Report: International Journal of Medical and Health Researchnur aslindahNo ratings yet
- Imp 1Document5 pagesImp 1pradeepgade1No ratings yet
- Fabrication of Interim Acrylic Partial DenturesDocument3 pagesFabrication of Interim Acrylic Partial DenturesFaheemuddin MuhammadNo ratings yet
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- Glow Oxygluta.pdfDocument1 pageGlow Oxygluta.pdfPadmini ReddyNo ratings yet
- Imaging TechniqueDocument3 pagesImaging TechniquePadmini ReddyNo ratings yet
- Situation of India in The COVID-19 Pandemic: India's Initial Pandemic ExperienceDocument18 pagesSituation of India in The COVID-19 Pandemic: India's Initial Pandemic ExperiencePadmini ReddyNo ratings yet
- SJ BDJ 2014 858Document5 pagesSJ BDJ 2014 858Padmini ReddyNo ratings yet
- Anatomy Respect in Implant Dentistry. Assortment, Location, Clinical ImportanceDocument33 pagesAnatomy Respect in Implant Dentistry. Assortment, Location, Clinical ImportancePadmini ReddyNo ratings yet
- Complication ManagementDocument6 pagesComplication ManagementPadmini ReddyNo ratings yet
- Presurgical Nasoalveolar Molding in A 4-Day-Old Infant With Unilateral Cleft Lip, Alveolus, and Palate DeformityDocument5 pagesPresurgical Nasoalveolar Molding in A 4-Day-Old Infant With Unilateral Cleft Lip, Alveolus, and Palate DeformityPadmini ReddyNo ratings yet
- Fabrication of Complete/partial Dentures (Different Final Impression Techniques and Materials) For Treating Edentulous Patients (Protocol)Document18 pagesFabrication of Complete/partial Dentures (Different Final Impression Techniques and Materials) For Treating Edentulous Patients (Protocol)Padmini ReddyNo ratings yet
- Seminar on Post and Core SystemsDocument46 pagesSeminar on Post and Core SystemsPadmini Reddy100% (1)
- MacOS Platform SSL Version Secure Transport Debug LogsDocument57 pagesMacOS Platform SSL Version Secure Transport Debug LogsPadmini ReddyNo ratings yet
- Mds TN QuesDocument14 pagesMds TN QuesPadmini ReddyNo ratings yet
- Removable Partial Dentures Designing: Forces As Primary ConcernDocument6 pagesRemovable Partial Dentures Designing: Forces As Primary ConcernPadmini ReddyNo ratings yet
- Occlusal Rims FabDocument8 pagesOcclusal Rims FabSalon LamichhaneNo ratings yet
- Rice Surf Paneer Mushroom Bread Milk Dahi Carrot FlossDocument1 pageRice Surf Paneer Mushroom Bread Milk Dahi Carrot FlossPadmini ReddyNo ratings yet
- Prosthodontic Rehabilitation of Acquired Maxillofacial DefectsDocument24 pagesProsthodontic Rehabilitation of Acquired Maxillofacial DefectsPadmini ReddyNo ratings yet
- A Review On Stresses-Induced by Removable Partial DenturesDocument5 pagesA Review On Stresses-Induced by Removable Partial DenturesKrupali JainNo ratings yet
- Distal Extension Removable Partial Denture ProsthesisDocument17 pagesDistal Extension Removable Partial Denture ProsthesisPadmini ReddyNo ratings yet
- BacteriaDocument8 pagesBacteriaanamika_roy_5No ratings yet
- Ijamscr 15 215 - 308 312 PDFDocument5 pagesIjamscr 15 215 - 308 312 PDFShraddha AgarwalNo ratings yet
- Resilliance of TMJDocument4 pagesResilliance of TMJPadmini ReddyNo ratings yet
- Laboratory Fabrication Procedures of A Metal Partial Denture FrameworkDocument4 pagesLaboratory Fabrication Procedures of A Metal Partial Denture FrameworkPadmini ReddyNo ratings yet
- Extraoral Implants As Retentive AidDocument8 pagesExtraoral Implants As Retentive AidSatya AsatyaNo ratings yet
- Ceramic LaminateDocument13 pagesCeramic LaminatePadmini ReddyNo ratings yet
- Biomechanics of RPD 1Document9 pagesBiomechanics of RPD 1Padmini ReddyNo ratings yet
- Best Approach To RPD Design Best Approach To RPD DesignDocument34 pagesBest Approach To RPD Design Best Approach To RPD DesignPadmini ReddyNo ratings yet
- Removable Partial Dentures PDFDocument6 pagesRemovable Partial Dentures PDFPadmini ReddyNo ratings yet
- Enhanced Retention of A Maxillofacial Prosthetic Obturator Using Precision Attachments: Two Case ReportsDocument7 pagesEnhanced Retention of A Maxillofacial Prosthetic Obturator Using Precision Attachments: Two Case ReportsPadmini ReddyNo ratings yet
- A Review On Stresses-Induced by Removable Partial DenturesDocument5 pagesA Review On Stresses-Induced by Removable Partial DenturesKrupali JainNo ratings yet
- Nitte University Journal March 2012 - 54 - 60 PDFDocument7 pagesNitte University Journal March 2012 - 54 - 60 PDFPadmini ReddyNo ratings yet
- Best Home Oxygen Concentrators-Lowest Prices & Fast Shipping (Oxygen Machines) - 2021 - YuwellDocument1 pageBest Home Oxygen Concentrators-Lowest Prices & Fast Shipping (Oxygen Machines) - 2021 - YuwellPelayanan ResusitasiNo ratings yet
- HHG4M - Lifespan Development Textbook Lesson 2Document95 pagesHHG4M - Lifespan Development Textbook Lesson 2Lubomira SucheckiNo ratings yet
- Organizational Behaviour Group Assignment-2Document4 pagesOrganizational Behaviour Group Assignment-2Prateek KurupNo ratings yet
- Proposed Panel Antenna: Globe Telecom ProprietaryDocument2 pagesProposed Panel Antenna: Globe Telecom ProprietaryJason QuibanNo ratings yet
- SolarBright MaxBreeze Solar Roof Fan Brochure Web 1022Document4 pagesSolarBright MaxBreeze Solar Roof Fan Brochure Web 1022kewiso7811No ratings yet
- Communications201101 DLDocument132 pagesCommunications201101 DLAle SandovalNo ratings yet
- Project Report Software and Web Development Company: WWW - Dparksolutions.inDocument12 pagesProject Report Software and Web Development Company: WWW - Dparksolutions.inRavi Kiran Rajbhure100% (1)
- Barelwiyah, Barelvi Chapter 1 (Part 2 of 5)Document31 pagesBarelwiyah, Barelvi Chapter 1 (Part 2 of 5)Dawah ChannelNo ratings yet
- SeparatorDocument2 pagesSeparatormmk111No ratings yet
- How Do I Prepare For Public Administration For IAS by Myself Without Any Coaching? Which Books Should I Follow?Document3 pagesHow Do I Prepare For Public Administration For IAS by Myself Without Any Coaching? Which Books Should I Follow?saiviswanath0990100% (1)
- Continuous Sampling PlanDocument2 pagesContinuous Sampling PlanAnonymous wA6NGuyklDNo ratings yet
- Environmental Threats Differentiated Reading Comprehension Ver 1Document20 pagesEnvironmental Threats Differentiated Reading Comprehension Ver 1Camila DiasNo ratings yet
- EST I - Literacy Test I (Language)Document20 pagesEST I - Literacy Test I (Language)Mohammed Abdallah100% (1)
- Dyna 2000 LiteDocument2 pagesDyna 2000 LiteRNKNo ratings yet
- POPULARITY OF CREDIT CARDS ISSUED BY DIFFERENT BANKSDocument25 pagesPOPULARITY OF CREDIT CARDS ISSUED BY DIFFERENT BANKSNaveed Karim Baksh75% (8)
- District Wise List of Colleges Under The Juridiction of MRSPTU BathindaDocument13 pagesDistrict Wise List of Colleges Under The Juridiction of MRSPTU BathindaGurpreet SandhuNo ratings yet
- Cyber Security 2017Document8 pagesCyber Security 2017Anonymous i1ClcyNo ratings yet
- DLL Grade7 First 1solutions ConcentrationDocument5 pagesDLL Grade7 First 1solutions ConcentrationJaneth de JuanNo ratings yet
- Kennedy 1945 Bibliography of Indonesian Peoples and CulturesDocument12 pagesKennedy 1945 Bibliography of Indonesian Peoples and CulturesJennifer Williams NourseNo ratings yet
- Ringkasan LaguDocument4 pagesRingkasan LaguJoe PyNo ratings yet
- Hydrocarbon: Understanding HydrocarbonsDocument9 pagesHydrocarbon: Understanding HydrocarbonsBari ArouaNo ratings yet
- Reversing a String in 8086 Micro Project ReportDocument4 pagesReversing a String in 8086 Micro Project ReportOm IngleNo ratings yet
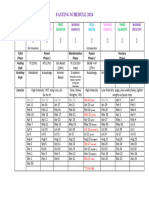
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Building Primitive Traps & SnaresDocument101 pagesBuilding Primitive Traps & SnaresJoseph Madr90% (10)
- Useful Relations in Quantum Field TheoryDocument30 pagesUseful Relations in Quantum Field TheoryDanielGutierrez100% (1)
- Solutions: Spheres, Cones and CylindersDocument13 pagesSolutions: Spheres, Cones and CylindersKeri-ann MillarNo ratings yet
- Project Report On AdidasDocument33 pagesProject Report On Adidassanyam73% (37)
- 3 - Content - Introduction To Java, JVM, JDK PDFDocument8 pages3 - Content - Introduction To Java, JVM, JDK PDFAnonymous zdY202lgZYNo ratings yet
- Omobonike 1Document13 pagesOmobonike 1ODHIAMBO DENNISNo ratings yet
- 16 Week Mountain Marathon Training Plan: WWW - Brutalevents.co - UkDocument2 pages16 Week Mountain Marathon Training Plan: WWW - Brutalevents.co - UkCristina CrsNo ratings yet