You might also like
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- A Dual-Purpose Guide For Optimum Placement of Dental ImplantsDocument4 pagesA Dual-Purpose Guide For Optimum Placement of Dental ImplantskadrologyNo ratings yet
- Imp 1Document5 pagesImp 1pradeepgade1No ratings yet
- An Easy Way of Chair-Side Stent Fabrication For Accurate Placement of Miniscrew ImplantDocument3 pagesAn Easy Way of Chair-Side Stent Fabrication For Accurate Placement of Miniscrew ImplantJORGE CARLOS MELGAR GUTIERREZNo ratings yet
- Immediateimplantplacementbeckeretalperio2k2008 PDFDocument11 pagesImmediateimplantplacementbeckeretalperio2k2008 PDFNiaz AhammedNo ratings yet
- Content ServerDocument7 pagesContent ServerEidy A HerasNo ratings yet
- Use of Diagnostic and Surgical Stent A SimplifiedDocument7 pagesUse of Diagnostic and Surgical Stent A Simplifiedwaf51No ratings yet
- 2 - 2023 - Novel Technique For Placement of Immediate Implant in Mandibular RegionDocument5 pages2 - 2023 - Novel Technique For Placement of Immediate Implant in Mandibular RegionVõHoàngThủyTiênNo ratings yet
- Development of Implant Soft Tissue Emergence ProfileDocument5 pagesDevelopment of Implant Soft Tissue Emergence ProfilemishNo ratings yet
- RSGDocument5 pagesRSGHugoMoralesTecnicoDentalNo ratings yet
- Bone Ring 1Document6 pagesBone Ring 1Pradusha RevuruNo ratings yet
- Dabreo 1990Document3 pagesDabreo 1990SaptarshiMondalNo ratings yet
- Ijss Feb Ra01Document5 pagesIjss Feb Ra01Ruxandra FitaNo ratings yet
- AJDSM Volume 22 Issue 3 Pages 247-251Document5 pagesAJDSM Volume 22 Issue 3 Pages 247-251MarisbebelaNo ratings yet
- Implant-Retained Cantilever Fixed Prosthesis: Where and WhenDocument4 pagesImplant-Retained Cantilever Fixed Prosthesis: Where and WhenSitiKhadijahNo ratings yet
- Current Methods For Soft Tissue Enhancement of The Esthetic ZoneDocument11 pagesCurrent Methods For Soft Tissue Enhancement of The Esthetic Zonecmfvaldesr7No ratings yet
- AsdfaDocument4 pagesAsdfaFree PizzaNo ratings yet
- Bodily Distalization of Molars With Absolute AnchorageDocument12 pagesBodily Distalization of Molars With Absolute AnchorageAnamika AttrishiNo ratings yet
- Immediate Implant Placement PDFDocument11 pagesImmediate Implant Placement PDFFerdinan PasaribuNo ratings yet
- Pneumocephalus As A Fatal But Very RareDocument27 pagesPneumocephalus As A Fatal But Very RareHossam ThabetNo ratings yet
- 1 s2.0 S0377529115300626 MainDocument6 pages1 s2.0 S0377529115300626 MainNémethBálintNo ratings yet
- Biomed 2Document5 pagesBiomed 2Olesea CutitaruNo ratings yet
- Double Jaw Immediate Load Hybrids: Case Abstract: Scott E. Keith, DDS, MsDocument3 pagesDouble Jaw Immediate Load Hybrids: Case Abstract: Scott E. Keith, DDS, MsShyam BhatNo ratings yet
- Complications With Osseointegrated Implants PDFDocument5 pagesComplications With Osseointegrated Implants PDFDental Del NorteNo ratings yet
- Loss of Anterior TissuesDocument5 pagesLoss of Anterior Tissuesjinny1_0No ratings yet
- Diastema Closure With Direct Composite: Architectural Gingival ContouringDocument6 pagesDiastema Closure With Direct Composite: Architectural Gingival ContouringDiego SarunNo ratings yet
- Ferula 1Document6 pagesFerula 1AlexNo ratings yet
- 1 s2.0 S0022391312001205 MainDocument5 pages1 s2.0 S0022391312001205 MainErwin SutonoNo ratings yet
- CCR3 4 831 PDFDocument7 pagesCCR3 4 831 PDFArmareality ArmarealityNo ratings yet
- Variations in Bracket Placement in The Preadjusted Orthodontic ApplianceDocument6 pagesVariations in Bracket Placement in The Preadjusted Orthodontic ApplianceAna Maria Clara HernándezNo ratings yet
- Accuracy of Miniscrew ImplantDocument8 pagesAccuracy of Miniscrew ImplantShaivi ShrivastavaNo ratings yet
- Rosa 2014Document6 pagesRosa 2014Michal PerkowskiNo ratings yet
- 7 - 2020 - A Digital Intraoral Implant Scan Technique Using A Combined Healing Abutment and Scan Body SystemDocument4 pages7 - 2020 - A Digital Intraoral Implant Scan Technique Using A Combined Healing Abutment and Scan Body SystemVõHoàngThủyTiênNo ratings yet
- Bone ReactionDocument9 pagesBone ReactionFourthMolar.comNo ratings yet
- CCD 4 509Document3 pagesCCD 4 509gbaez.88No ratings yet
- The Biotransfer Approach: The Use of An Alveolar Cast Die For The Fabrication of The Emergence Profile On Implant-Supported Interim RestorationsDocument4 pagesThe Biotransfer Approach: The Use of An Alveolar Cast Die For The Fabrication of The Emergence Profile On Implant-Supported Interim RestorationsClaudioNo ratings yet
- Horizontal Ridge Augmentation Using Particulate BoneDocument12 pagesHorizontal Ridge Augmentation Using Particulate Bonecmfvaldesr7No ratings yet
- Ac 72Document5 pagesAc 72Giovani TardiniNo ratings yet
- Prosthetic Rehabilitation Using Extra Coronal Attachments: Case ReportDocument4 pagesProsthetic Rehabilitation Using Extra Coronal Attachments: Case ReportLakshmi Sarvani ValluriNo ratings yet
- Evaluation of Interarch Space For ImplanDocument4 pagesEvaluation of Interarch Space For Implanwaf51No ratings yet
- I S M B M o L A: CDocument7 pagesI S M B M o L A: CAshraf KamalNo ratings yet
- TMP 371 BDocument4 pagesTMP 371 BFrontiersNo ratings yet
- An 2/2 Implant Overdenture: Case ReportDocument3 pagesAn 2/2 Implant Overdenture: Case ReportasclepiuspdfsNo ratings yet
- Document PDFDocument4 pagesDocument PDFBagis Emre GulNo ratings yet
- Analysis of Influence of Lip Line and Lip Support in Esthetics and SelectionDocument3 pagesAnalysis of Influence of Lip Line and Lip Support in Esthetics and SelectionDaniel AtiehNo ratings yet
- Botticelli 2004Document9 pagesBotticelli 2004medNo ratings yet
- A Tooth-Stabilized Surgical Template For AlveolectomyDocument3 pagesA Tooth-Stabilized Surgical Template For Alveolectomyheri asriyadiNo ratings yet
- A New Design For A Hybrid PDocument16 pagesA New Design For A Hybrid PDavid CLNo ratings yet
- Articol Pentru Teme 14-18Document9 pagesArticol Pentru Teme 14-18Diamanta Yalomit CirsteaNo ratings yet
- The Hybrid Denture1Document9 pagesThe Hybrid Denture1SitiKhadijah100% (1)
- Survey and DesignDocument4 pagesSurvey and DesignPadmini ReddyNo ratings yet
- Asds 06 1448Document7 pagesAsds 06 1448Joao Carlos JuniorNo ratings yet
- 2007 JomiDocument7 pages2007 JomiCássio BernardNo ratings yet
- The Team ApproachDocument2 pagesThe Team ApproachThe SmileNo ratings yet
- Use of Titanium Mesh For Staged Localized Aeveolar Ridge AugmentationDocument12 pagesUse of Titanium Mesh For Staged Localized Aeveolar Ridge AugmentationAnonymous bOhsjs1Y7mNo ratings yet
- Australian Dental Journal - 2008 - Blum - A Quick and Simple Method To Obtain A Radiographic Evaluation of RemainingDocument3 pagesAustralian Dental Journal - 2008 - Blum - A Quick and Simple Method To Obtain A Radiographic Evaluation of RemainingPatricia CauanNo ratings yet
- Ultrasonic Versus Drills Implant Site Preparation: A Histologic Analysis in Bovine RibsDocument4 pagesUltrasonic Versus Drills Implant Site Preparation: A Histologic Analysis in Bovine RibsAnusha BorraNo ratings yet
- Clinical Application of Various Surgical Guides For Optimal Implant PlacementDocument9 pagesClinical Application of Various Surgical Guides For Optimal Implant PlacementMrinmayee ThakurNo ratings yet
- Provisional RestorationsDocument4 pagesProvisional RestorationsMyri Gebert SchererNo ratings yet
- 2022 - Effect of Guiding Sleeve Design On Intraosseous Heat Generation During Implant Site PreparationDocument8 pages2022 - Effect of Guiding Sleeve Design On Intraosseous Heat Generation During Implant Site PreparationVõHoàngThủyTiênNo ratings yet
- 1 s2.0 S0022391323003761 MainDocument3 pages1 s2.0 S0022391323003761 MainVõHoàngThủyTiênNo ratings yet
- The Impact of Surgical Guide Fixation and Implant Location On Accuracy of Static ComputerDocument10 pagesThe Impact of Surgical Guide Fixation and Implant Location On Accuracy of Static ComputerGustavo IsmaelNo ratings yet
- 2019 - in Vitro Comparison Between Metal Sleeve-Free and Metal SleeveDocument10 pages2019 - in Vitro Comparison Between Metal Sleeve-Free and Metal SleeveVõHoàngThủyTiênNo ratings yet
- 2018 - The Influence of Guided Sleeve Height, Drilling Distance and Drilling Key Length On The Accuracy of Static ComputerAssisted Implant SurgeryDocument7 pages2018 - The Influence of Guided Sleeve Height, Drilling Distance and Drilling Key Length On The Accuracy of Static ComputerAssisted Implant SurgeryVõHoàngThủyTiênNo ratings yet
- S - 2022 - Open-Sleeve Templates For Computer-Assisted Implant Surgery at Healed or Extraction SocketsDocument11 pagesS - 2022 - Open-Sleeve Templates For Computer-Assisted Implant Surgery at Healed or Extraction SocketsVõHoàngThủyTiênNo ratings yet
- Chenetal 2009aJOMIDocument33 pagesChenetal 2009aJOMI63127No ratings yet
- 2 - 2023 - Novel Technique For Placement of Immediate Implant in Mandibular RegionDocument5 pages2 - 2023 - Novel Technique For Placement of Immediate Implant in Mandibular RegionVõHoàngThủyTiênNo ratings yet
- A Systematic Review of The Accuracy of Digital Surgical Guides For Dental ImplantationDocument23 pagesA Systematic Review of The Accuracy of Digital Surgical Guides For Dental ImplantationehabidentNo ratings yet
- 2020 - Stereolithographic Surgical Guide With A Combination of Tooth and Bone SupportDocument13 pages2020 - Stereolithographic Surgical Guide With A Combination of Tooth and Bone SupportVõHoàngThủyTiênNo ratings yet
- 2019 - in Vitro Comparison Between Metal Sleeve-Free and Metal SleeveDocument10 pages2019 - in Vitro Comparison Between Metal Sleeve-Free and Metal SleeveVõHoàngThủyTiênNo ratings yet
- 2011 - Key Principles That Enhance Success When Restoring Endodontically Treated TeethDocument7 pages2011 - Key Principles That Enhance Success When Restoring Endodontically Treated TeethVõHoàngThủyTiênNo ratings yet
- S - 2022 - Open-Sleeve Templates For Computer-Assisted Implant Surgery at Healed or Extraction SocketsDocument11 pagesS - 2022 - Open-Sleeve Templates For Computer-Assisted Implant Surgery at Healed or Extraction SocketsVõHoàngThủyTiênNo ratings yet
- S - 2019 - Influence of Implant Macrodesign and Insertion Connection Technology On The Accuracy of Static Computer-Assisted Implant SurgeryDocument7 pagesS - 2019 - Influence of Implant Macrodesign and Insertion Connection Technology On The Accuracy of Static Computer-Assisted Implant SurgeryVõHoàngThủyTiênNo ratings yet
- 2018 - The Influence of Guided Sleeve Height, Drilling Distance and Drilling Key Length On The Accuracy of Static ComputerAssisted Implant SurgeryDocument7 pages2018 - The Influence of Guided Sleeve Height, Drilling Distance and Drilling Key Length On The Accuracy of Static ComputerAssisted Implant SurgeryVõHoàngThủyTiênNo ratings yet
- Protecting All Children's Teeth: CariesDocument45 pagesProtecting All Children's Teeth: CariesTUTOR ENAM CD TIGANo ratings yet
- APolycromaticCompositeLayeringApproachforSolvingaComplexClassIV DirectVenner DiastemaCombination Part2Document7 pagesAPolycromaticCompositeLayeringApproachforSolvingaComplexClassIV DirectVenner DiastemaCombination Part2Ayu RafaniaNo ratings yet
- APolycromaticCompositeLayeringApproachforSolvingaComplexClassIV DirectVenner DiastemaCombination Part2Document7 pagesAPolycromaticCompositeLayeringApproachforSolvingaComplexClassIV DirectVenner DiastemaCombination Part2Ayu RafaniaNo ratings yet
- Carcinosarcoma of Parotid Gland Malignant Mixed TuDocument4 pagesCarcinosarcoma of Parotid Gland Malignant Mixed TuVõHoàngThủyTiênNo ratings yet
- Case ReportDocument52 pagesCase ReportVõHoàngThủyTiênNo ratings yet
- Clinical Tips & Tricks Anterior Restorations. FiltekTM. Supreme Plus. Universal RestorativeDocument40 pagesClinical Tips & Tricks Anterior Restorations. FiltekTM. Supreme Plus. Universal RestorativeVõHoàngThủyTiênNo ratings yet
- Dietschi 2016 PDFDocument7 pagesDietschi 2016 PDFPanchyRojasNo ratings yet
- APolycromaticCompositeLayeringApproachforSolvingaComplexClassIV DirectVenner DiastemaCombination Part1Document7 pagesAPolycromaticCompositeLayeringApproachforSolvingaComplexClassIV DirectVenner DiastemaCombination Part1VõHoàngThủyTiênNo ratings yet
- Design: Dung d ịch bù nước qua đường uốngDocument2 pagesDesign: Dung d ịch bù nước qua đường uốngVõHoàngThủyTiênNo ratings yet
- Necrotising Ulcerative Gingivitis: A Literature Review: James Dufty / Nikolaos Gkranias / Nikos DonosDocument10 pagesNecrotising Ulcerative Gingivitis: A Literature Review: James Dufty / Nikolaos Gkranias / Nikos DonosmayaNo ratings yet
- Phrma Seniority List 01Document38 pagesPhrma Seniority List 01vasan980100% (1)
- BOSIET With EBS Course Descriptor & Joinning InstructionDocument5 pagesBOSIET With EBS Course Descriptor & Joinning InstructionNisamudheenNo ratings yet
- Mental Hygiene Reaction PaperDocument2 pagesMental Hygiene Reaction PaperMary Louise Vapor UyvicoNo ratings yet
- PRE OP ChecklistDocument1 pagePRE OP ChecklistDR.No ratings yet
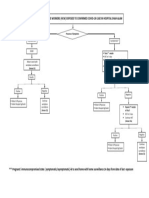
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- 1st Quarter 2022 CBDRP-Reporting-Forms - IfugaoDocument53 pages1st Quarter 2022 CBDRP-Reporting-Forms - IfugaoJeda MonayaoNo ratings yet
- Drug Delivery SystemDocument14 pagesDrug Delivery SystemAmit PrasadNo ratings yet
- Psychia Ncp-MetchelDocument9 pagesPsychia Ncp-MetchelCarmelita SaltNo ratings yet
- TFN 3F Concept of HealthDocument2 pagesTFN 3F Concept of HealthkushiroNo ratings yet
- Australasian Health Facility Guidelines 2013Document49 pagesAustralasian Health Facility Guidelines 2013aegysabetterwayNo ratings yet
- ReportDocument7 pagesReportapi-482961632No ratings yet
- Addiction World Conference AWC 2024Document2 pagesAddiction World Conference AWC 2024addictionNo ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- Applying To The AmcDocument72 pagesApplying To The AmcgracieMD100% (1)
- Burning Mouth Syndrome and Treatment With ParoxetinDocument2 pagesBurning Mouth Syndrome and Treatment With ParoxetinFitri AngginiNo ratings yet
- JobsDocument8 pagesJobsPalani Samy TNo ratings yet
- Prescription - Apollo 2471659105066202Document2 pagesPrescription - Apollo 2471659105066202JEENEET CHEMISTRYNo ratings yet
- Code of SanitationDocument8 pagesCode of SanitationNikki Nina Arabe BarcinasNo ratings yet
- Baidyanath Ayurvedic LTD: Presented By: Group 7 Pragati Punith Ritesh Shwethakumari Uma YashawanthDocument25 pagesBaidyanath Ayurvedic LTD: Presented By: Group 7 Pragati Punith Ritesh Shwethakumari Uma YashawanthPragati A SubbannavarNo ratings yet
- Explanation Essay Example and ActivityDocument6 pagesExplanation Essay Example and ActivityAlesther Vhon D. PedronNo ratings yet
- Institutional Review Board/Independent Ethics Committee (Irb/Iec)Document40 pagesInstitutional Review Board/Independent Ethics Committee (Irb/Iec)Swati chauhanNo ratings yet
- Sarver Mission PossibleDocument13 pagesSarver Mission PossibleAndrea Cárdenas Sandoval100% (1)
- E-Learning, Telemadicin, Tele Nursing AssignmentDocument22 pagesE-Learning, Telemadicin, Tele Nursing AssignmentBhawna Joshi100% (2)
- List of HospitalsDocument13 pagesList of HospitalsRajeev VenegallaNo ratings yet
- Talay Behavioral Center Outreach ProgramDocument1 pageTalay Behavioral Center Outreach ProgramiMaibelle BelleNo ratings yet
- PDF Introduction To Surveillance RA 11332Document35 pagesPDF Introduction To Surveillance RA 11332Dan Joseph AguilarNo ratings yet
- TOP Dialysis Centres in MumbaiDocument2 pagesTOP Dialysis Centres in MumbaiTerminal VelocityNo ratings yet
- Bridging The Gap Between Medical Literacy and Language BarrierDocument6 pagesBridging The Gap Between Medical Literacy and Language BarrierstanleyNo ratings yet
- Oet Speakingr PDFDocument133 pagesOet Speakingr PDFAlphonsa Thomas100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)