You might also like
- What Are The Main Ethical Issues in Human Subjects ResearchDocument4 pagesWhat Are The Main Ethical Issues in Human Subjects ResearchMarkLawrenceLanderoValdezNo ratings yet
- Ethical Issues in Clinical TrialsDocument16 pagesEthical Issues in Clinical TrialsPranjal KothaleNo ratings yet
- IICRDocument17 pagesIICRMukund SharmaNo ratings yet
- Problem of Brain Drain in IndiaDocument3 pagesProblem of Brain Drain in IndiaHardik PatelNo ratings yet
- Ethics in Research FMCHDocument44 pagesEthics in Research FMCHPatricia Hariramani100% (1)
- Orphan DrugsDocument3 pagesOrphan Drugslisawong87No ratings yet
- Ethical Issues in Clinical Trials: Dr. Devesh D. GosaviDocument86 pagesEthical Issues in Clinical Trials: Dr. Devesh D. Gosavidevesh gosaviNo ratings yet
- Research Methodology PDFDocument250 pagesResearch Methodology PDFRafzeenaNo ratings yet
- Ethics Committee Roles and Responsibilities - by Dr. Shiva Murthy NDocument30 pagesEthics Committee Roles and Responsibilities - by Dr. Shiva Murthy NDr. Shiva Murthy NNo ratings yet
- Cohort DesignDocument41 pagesCohort DesignHope EkwensiNo ratings yet
- Clinical Study: Design and Methods: Hail M. Al-Abdely, MDDocument64 pagesClinical Study: Design and Methods: Hail M. Al-Abdely, MDkazugawaNo ratings yet
- Elements of Informed Consent - Lu PaiDocument31 pagesElements of Informed Consent - Lu PaiAl YsSa Ricafort Millabas100% (1)
- Clinical ResearchDocument5 pagesClinical ResearchDeepti ShrivasNo ratings yet
- New Drugs and Clinical Trials Rules, 2019 - A Regulatory Overview - India Corporate LawDocument7 pagesNew Drugs and Clinical Trials Rules, 2019 - A Regulatory Overview - India Corporate LawMeghna SinghNo ratings yet
- Ich GCP: HistoryDocument57 pagesIch GCP: HistoryChandrashekhar Singh100% (1)
- ##2022 Informed Consent NotesDocument11 pages##2022 Informed Consent NotesSANTHIYA A/P MOHANA SUNDARAM MoeNo ratings yet
- Interview and Schedule MethodDocument19 pagesInterview and Schedule MethodMANISH KUMARNo ratings yet
- Suraksha Independent Ethics CommitteeDocument8 pagesSuraksha Independent Ethics CommitteeclinfoxNo ratings yet
- Research Ethics For LectureDocument38 pagesResearch Ethics For LectureamitksknpNo ratings yet
- Ethical Issues in Clinical ResearchDocument33 pagesEthical Issues in Clinical ResearchSenthil ThyagarajanNo ratings yet
- Modules - Special Crime Investigation With Interogation-2Document11 pagesModules - Special Crime Investigation With Interogation-2Krizia Faye Pillos ManuelNo ratings yet
- Research and Ethical CommitteeDocument8 pagesResearch and Ethical Committeefarha naazNo ratings yet
- Effectiveness of Therapeutic Communities - A Comparison of PrisonDocument38 pagesEffectiveness of Therapeutic Communities - A Comparison of PrisonJan Lorence AlbanoNo ratings yet
- ICH E6-R3 GCP-Principles Draft 2021 0419Document7 pagesICH E6-R3 GCP-Principles Draft 2021 0419ramya sandraNo ratings yet
- Experimental Psychology Lecture Activity Worksheet No. 1 Module 2: Research EthicsDocument1 pageExperimental Psychology Lecture Activity Worksheet No. 1 Module 2: Research EthicsCarollyne cruzNo ratings yet
- Research BulletsDocument18 pagesResearch BulletsVong Albios DogomeoNo ratings yet
- G.S.Bajpai & Preetika SharmaDocument30 pagesG.S.Bajpai & Preetika SharmaBajpai GSNo ratings yet
- Knowledge Attitude and Practices Regarding Respiratory SymptomsDocument8 pagesKnowledge Attitude and Practices Regarding Respiratory SymptomsK162404 Nauraiz SubhanNo ratings yet
- Legal Issues in Clinical ResearchDocument48 pagesLegal Issues in Clinical ResearchAhmed MashalyNo ratings yet
- Research Protocol TemplateDocument6 pagesResearch Protocol TemplateAshref BelhajNo ratings yet
- Ethical Issues in Scientific Research An Anthology PDFDocument2 pagesEthical Issues in Scientific Research An Anthology PDFRobertNo ratings yet
- Crisis ManagementDocument6 pagesCrisis ManagementPranita MehtaNo ratings yet
- Safety Monitoring in Clinical TrailDocument3 pagesSafety Monitoring in Clinical TrailShivananda PradhanNo ratings yet
- A Scientific Research Be Gins With A Single Carefully Observed Event and Progresses Ultimately To The Formulation of Theories and LawsDocument6 pagesA Scientific Research Be Gins With A Single Carefully Observed Event and Progresses Ultimately To The Formulation of Theories and LawsPayal SharmaNo ratings yet
- Phases in Clinical TrialsDocument4 pagesPhases in Clinical TrialsManish SarasvatiNo ratings yet
- Informed ConsentDocument32 pagesInformed ConsentSara Montañez Barajas0% (1)
- Clinical Research: Presented By: Deepali KhetmalisDocument16 pagesClinical Research: Presented By: Deepali KhetmalisAmol KokaneNo ratings yet
- Human Research Protection Program Informed Consent ProcessDocument6 pagesHuman Research Protection Program Informed Consent ProcessNurul KurniawatiNo ratings yet
- Good Scientific Practice and Ethical Principles in Scientific Research and Higher EducationDocument5 pagesGood Scientific Practice and Ethical Principles in Scientific Research and Higher EducationIrene NiandariNo ratings yet
- REVIEWER3 IsDocument4 pagesREVIEWER3 IsNicole FuraqueNo ratings yet
- ICH GCP & Indian Clinical Trial GuidelineDocument97 pagesICH GCP & Indian Clinical Trial GuidelineRanjeet PrasadNo ratings yet
- Knowledge, Attitudes, and Practices of Selected Regions in The Philippines On Electronic Medical RecordsDocument4 pagesKnowledge, Attitudes, and Practices of Selected Regions in The Philippines On Electronic Medical RecordsEman GloriaNo ratings yet
- What Is The Inductive MethodDocument5 pagesWhat Is The Inductive MethodLlight Acosta100% (1)
- Publication Misconduct: DR - Preeta Lall Asst. Professor - Economics Rajiv Gandhi Govt. College, Simga Disstt. BalodabazarDocument56 pagesPublication Misconduct: DR - Preeta Lall Asst. Professor - Economics Rajiv Gandhi Govt. College, Simga Disstt. Balodabazarsanjay kumarNo ratings yet
- PocsoDocument14 pagesPocsoyasin pt100% (1)
- Experimental Psychology & The Scientific MethodDocument73 pagesExperimental Psychology & The Scientific MethodRuru LavariasNo ratings yet
- University of Utah Kaplan Lab ReportDocument9 pagesUniversity of Utah Kaplan Lab ReportLindsay Whitehurst0% (1)
- Chapter 3 - Understanding Research EthicsDocument16 pagesChapter 3 - Understanding Research Ethicsniaz kilamNo ratings yet
- Study DesignsDocument24 pagesStudy DesignsJasmen Sabroso PasiaNo ratings yet
- Demand Diversity - COVID-19 ResearchDocument39 pagesDemand Diversity - COVID-19 ResearchCOUCH Health50% (2)
- The Right To HealthDocument52 pagesThe Right To HealthGlobal Justice AcademyNo ratings yet
- Mental Health Act: Implementing Rules and Regulations of Republic Act No. 11036Document20 pagesMental Health Act: Implementing Rules and Regulations of Republic Act No. 11036RJ BalladaresNo ratings yet
- Silo - Tips Chapter 1 History and Ethical PrinciplesDocument50 pagesSilo - Tips Chapter 1 History and Ethical PrinciplesCaroline Silveira BauerNo ratings yet
- Good Clinical Practice - Harshad MoreDocument24 pagesGood Clinical Practice - Harshad MoreHarshad MoreNo ratings yet
- Ethical Considerations During Research 1Document22 pagesEthical Considerations During Research 1Dr Bazmi InamNo ratings yet
- Ethics, Qualitative And Quantitative Methods In Public Health ResearchFrom EverandEthics, Qualitative And Quantitative Methods In Public Health ResearchNo ratings yet
- Chapter 2-Ethical Issues in Nursing ResearchDocument43 pagesChapter 2-Ethical Issues in Nursing Researchalhader libraryNo ratings yet
- Ethical Consideration in Nursing ResearchDocument1 pageEthical Consideration in Nursing Researcheinna loraineNo ratings yet
- What Special Protections Are Required To Enable Vulnerable Populations To Participate in Research?Document63 pagesWhat Special Protections Are Required To Enable Vulnerable Populations To Participate in Research?Josue ColónNo ratings yet
- WBSR IiDocument45 pagesWBSR IiAbhiram BanerjeeNo ratings yet
- Contractual EmployeeDocument3 pagesContractual EmployeeAbhiram BanerjeeNo ratings yet
- Dmo, AtiDocument22 pagesDmo, AtiAbhiram BanerjeeNo ratings yet
- WBSR - IDocument46 pagesWBSR - IAbhiram BanerjeeNo ratings yet
- Statistical Confirmation of The Repertory: A Historic Step Towards Evidence-Based PracticeDocument37 pagesStatistical Confirmation of The Repertory: A Historic Step Towards Evidence-Based PracticeAbhiram BanerjeeNo ratings yet
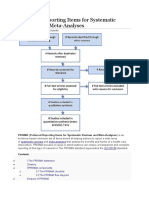
- Preferred Reporting Items For Systematic Reviews and Meta-AnalysesDocument3 pagesPreferred Reporting Items For Systematic Reviews and Meta-AnalysesAbhiram BanerjeeNo ratings yet
- Cru (H) SiliguriDocument11 pagesCru (H) SiliguriAbhiram BanerjeeNo ratings yet
- Leave RulesDocument10 pagesLeave RulesAbhiram BanerjeeNo ratings yet
- Clinical Research ManualDocument285 pagesClinical Research ManualAbhiram Banerjee100% (5)
- Short Summary of CCRH-VC ProjectDocument2 pagesShort Summary of CCRH-VC ProjectAbhiram BanerjeeNo ratings yet
- Homeopathy The Human Medicine Leon VannierDocument5 pagesHomeopathy The Human Medicine Leon VannierAbhiram Banerjee100% (2)
- Research Methods: A Framework For Evidence-Based Clinical PracticeDocument22 pagesResearch Methods: A Framework For Evidence-Based Clinical PracticeAbhiram BanerjeeNo ratings yet
- A Garden of Eden in The Squares of Jerusalem, Zachariah 8,4-6Document12 pagesA Garden of Eden in The Squares of Jerusalem, Zachariah 8,4-6elverefur3587No ratings yet
- Examination of Nutrition Knowledge, Attitude, and Dietary Behaviors of College Student Vegetarians, Semi-Vegetarians, and Non-VegestariansDocument11 pagesExamination of Nutrition Knowledge, Attitude, and Dietary Behaviors of College Student Vegetarians, Semi-Vegetarians, and Non-VegestariansMeilindaNo ratings yet
- Margaret Sharon Worsham v. A.H. Robins Company, 734 F.2d 676, 11th Cir. (1984)Document21 pagesMargaret Sharon Worsham v. A.H. Robins Company, 734 F.2d 676, 11th Cir. (1984)Scribd Government DocsNo ratings yet
- Practical Advice For Pure Land Practitioners - HuijingDocument16 pagesPractical Advice For Pure Land Practitioners - HuijingHerbert Edgar WyndhamNo ratings yet
- Static Force AnalysisDocument16 pagesStatic Force AnalysisMohamed Ashraf HindyNo ratings yet
- Instrument of Government (1772) - WikipediaDocument3 pagesInstrument of Government (1772) - WikipediaMr. MeNo ratings yet
- Composite Member EI ValueDocument4 pagesComposite Member EI ValueArjun RajaNo ratings yet
- Lecture HW 5 ProbText Moran2003 Chp11 FluidStaticsDocument2 pagesLecture HW 5 ProbText Moran2003 Chp11 FluidStaticsPanawit HanpinitsakNo ratings yet
- Decay Heat CalculationDocument12 pagesDecay Heat CalculationUdit OjhaNo ratings yet
- The Way of Tthe Cross - CPdODocument23 pagesThe Way of Tthe Cross - CPdOACCobraGNo ratings yet
- GIC TestDocument5 pagesGIC TestRishabh AgarwalNo ratings yet
- Iodine Content in Clove OilDocument5 pagesIodine Content in Clove OilleahNo ratings yet
- Compresor Atlas Copco GA30Document16 pagesCompresor Atlas Copco GA30Florin Maria Chirila100% (1)
- Europump Atex Guide - II-rev2019 1.0Document14 pagesEuropump Atex Guide - II-rev2019 1.0Antonio MakkarovNo ratings yet
- Acoplamiento Ventriculo Arterial Sepsis PDFDocument6 pagesAcoplamiento Ventriculo Arterial Sepsis PDFRoger Ludeña SalazarNo ratings yet
- Deber FiscioDocument3 pagesDeber FiscioEstefy LaglaNo ratings yet
- VLD 6000 AIS Airborne Transponder PDFDocument2 pagesVLD 6000 AIS Airborne Transponder PDFShin Ami IgamiNo ratings yet
- Fm-npd-16 (Temp. Change Request Note)Document1 pageFm-npd-16 (Temp. Change Request Note)akash.vd.1603No ratings yet
- TXDVXX 12Document7 pagesTXDVXX 12Pedro RochaNo ratings yet
- Impact of Thermal Aging On The Intermetallic Compound Particle Size andDocument9 pagesImpact of Thermal Aging On The Intermetallic Compound Particle Size andAamir JanNo ratings yet
- Test Accounting Kiến thức Những chủ điểm quan trọng trong phần AccountingDocument20 pagesTest Accounting Kiến thức Những chủ điểm quan trọng trong phần AccountingTrần MaiNo ratings yet
- Changes Guide: Premier Elite Series - From V2.11 To V3.00Document16 pagesChanges Guide: Premier Elite Series - From V2.11 To V3.00NaveenKumarReddyNo ratings yet
- Ella Brown - Video Questions - Electric Charge Crash Course Physics #25Document4 pagesElla Brown - Video Questions - Electric Charge Crash Course Physics #25Ella BrownNo ratings yet
- Presentation Rheinmetall Hand GrenadesDocument24 pagesPresentation Rheinmetall Hand Grenadesn0dazeNo ratings yet
- Chemistry Test 11 Chap 1-5Document2 pagesChemistry Test 11 Chap 1-5Sabitra RudraNo ratings yet
- JLG ANSI & CSA Standards Readiness GuideDocument8 pagesJLG ANSI & CSA Standards Readiness GuideAlfredo VSNo ratings yet
- 3a. CONOPS Vigilancia ADS-B Base Terrestre COCESNADocument37 pages3a. CONOPS Vigilancia ADS-B Base Terrestre COCESNADairo FerrerNo ratings yet
- Company Contact Person Mob Contact No IndustryDocument1 pageCompany Contact Person Mob Contact No IndustryDhirajNo ratings yet
- Capacity and Facilities DesignDocument59 pagesCapacity and Facilities DesignAnshikaNo ratings yet
- TestosteroneDocument113 pagesTestosteroneresche6017No ratings yet